The development of the middle and inner ear highlights the intricacy of embryology. As early as 3 weeks after fertilization, the inner ear begins taking form. This process, along with development of the middle ear, continues throughout gestation. At birth, the middle ear, inner ear, and associated structures are almost adult size. An understanding of the embryologic development of the ear serves as a foundation for evaluating and managing congenital malformations of these structures. The focus of this article is the normal, abnormal, and arrested development of the middle and inner ear, with a clinical emphasis on malformed middle and inner ear structures and a discussion of associated syndromes.
Middle ear development
The external auditory canal develops from the first branchial groove, between the mandibular and hyoid arches (the first and second branchial arches, respectively). The tympanic ring develops from contact between the ectoderm of the first branchial groove and the first pharyngeal pouch. This contact point is interrupted by mesodermal growth (neural crest mesenchyme) at 8 weeks’ gestation. This mesenchyme thins to form the fibrous layer of the tympanic membrane. Thus, the tympanic membrane develops from all three embryologic layers, with ectoderm forming the lateral aspect, mesoderm forming the middle layer, and endoderm from the pharyngeal pouch forming the middle layer. The complete tympanic membrane fuses with the tympanic ring during gestational weeks 9 to 16, with ossification of the tympanic ring occurring after birth .
At week 3 of gestation, the middle ear forms from the tubotympanic recess. The tubotympanic recess develops from expansion of the first and possibly a small contribution from the second pharyngeal pouch. The tubotympanic recess becomes constricted by the second branchial arch during week 7, resulting in formation of the eustachian tube medially and the tympanic cavity laterally. The middle ear develops from the terminal end of the first pharyngeal pouch, which divides into four sacci representing distinct anatomic areas by the time of complete development. The saccus anticus (anterior pouch of Tröltsch), the saccus medius (epitympanum and petrous area), the saccus superior (posterior pouch of Tröltsch, inferior incudal space, and part of the mastoid), and saccus posterior (the round window, the oval window, and the sinus tympani) develop from the terminal end of the first pharyngeal pouch and expand to pneumatize the middle ear. Expansion of the sacci covers the ossicles and lines the tympanic and mastoid cavities. Extension of the tympanic cavity at 18 weeks’ gestation leads to formation of the epitympanum.
Ossicular development
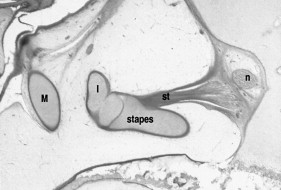
The ossicles, muscles, and tendons of the middle ear are formed from the mesenchyme of the middle ear and are covered by the epithelial lining from the first pharyngeal pouch. Blood vessels run under the epithelial lining, tethering structures in a mesenteric fashion. The tensor tympani muscle and tendon are derived from the first branchial arch and thus innervated by the mandibular branch of the trigeminal nerve. The stapedius muscle is derived from the second branchial arch mesoderm and innervated by the seventh cranial nerve ( Fig. 1 ).
Ossicular development starts at the fourth to sixth week as neural crest mesenchyme from the first and second branchial arches becomes further divided by the seventh cranial nerve. Differentiation of the neural crest mesenchymal tissue within the tympanic cavity results in formation of the individual ossicles. The head of the malleus and short crus and body of the incus are derived from the mesenchyme of the first branchial arch (mandibular arch). The manubrium of the malleus; long process of the incus; stapes head, neck, and crura; and the tympanic surface of the footplate are derived from the second branchial arch (hyoid arch). The medial stapes footplate and annular stapedial ligament are derived from the otic capsule. The bony otic capsule is adult size by 22 weeks’ gestation.
At 6 weeks’ gestation, the neural crest mesenchyme forms cartilaginous models of the ossicles, which subsequently grow to adult size by 15 to 18 weeks and completely ossify by 30 weeks. The incus and malleus, previously one collection of cells, separate with formation of the malleoincudal joint at 8 to 9 weeks. Mesenchymal resorption results in the ossicles being free, with the endodermal epithelium tethering the ossicles to the tympanic cavity in a mesentery-like fashion. The stapes ring forms around the transient stapedial artery at 5 to 6 weeks, followed by appearance of the otic capsule mesenchyme. The shape of the stapes becomes its characteristic stirrup shape during the 10th week, after which time the stapedial artery regresses. By the sixth month, the ossicles have achieved adult size; the middle ear cavity, the oval and round windows, and the tympanic membrane reach adult size at the time of birth.
Development of middle ear space and mastoid space
The tympanic cavity is covered by the tegmen tympani, which is an extension laterally of the otic capsule and medially from a band of fibrous tissue. The anterior epitympanic wall and the lateral tympanic cavity are formed from the tympanic process of the squamous temporal bone .
By 3 months of gestation, the mesenchyme filling the tympanic cavity becomes loose and vacuolated, allowing the tympanic cavity to expand. This expansion is complete by week 30; expansion of the epitympanum follows in the subsequent 4 weeks. The antrum extends laterally from the epitympanum beginning at 21 to 22 weeks, with near complete development by 34 weeks. Pneumatization of the mastoid air cells begins at approximately 33 weeks. Complete mastoid bone development occurs after birth. The lining epithelium expands the air cells, resulting in expansion of the antrum and the tympanic plate. The mastoid tip is not developed at birth but develops subsequently from the inferiorly directed traction of the sternocleidomastoid muscle, usually being complete by 1 year of age.
Inner ear development
The inner ear, consisting of the membranous labyrinth surrounded by a bony labyrinth, is adult size at the time of birth (except for changes in the periosteal layer and continued growth of the endolymphatic system). The membranous labyrinth (utricle, saccule, semicircular ducts, endolymphatic sac and duct, and cochlear duct), which is filled with endolymph, resides within the bony labyrinth, which is filled with perilymph. At 22 days of development, surface ectoderm on each side of the rhombencephalon thickens to form the otic placodes, which subsequently invaginate and form otocysts (otic and auditory vesicles), separating from the overlying ectoderm. Each vesicle divides into a ventral component that gives rise to the saccule and cochlear duct and a dorsal component that forms the utricle, semicircular canals, and endolymphatic duct. These epithelial structures are known as the membranous labyrinth .
In the sixth week of development, the cochlear duct forms from a tubular outgrowth of the saccule and penetrates surrounding mesenchyme to complete 2.5 turns by 8 weeks ( Fig. 2 ). The ductus reuniens is the remaining stalk that connects the saccule and the newly formed cochlear duct. The mesenchyme surrounding the cochlear duct differentiates into cartilage, and in the 10th week, this cartilaginous shell undergoes vacuolization to create the scala vestibuli and scala tympani, both perilymph spaces. The epithelial cells of the cochlear duct differentiate into an inner ridge (eventual spiral limbus) and outer ridge (eventual organ of Corti). The cells in these two ridges secrete a gelatinous substance that becomes the tectorial membrane . The cochlear modiolus, carrying the cochlear nerve, develops from membranous bone ( Fig. 3 ). Bone deposition occurs within the modiolus between 20 and 21 weeks between the basal and second turns of the cochlea, and by week 25, ossification is nearly complete .
The semicircular canals begin as evaginations of the utricular part of the otic vesicle during the sixth week. The walls of these outpocketings come into contact with one another to create three semicircular canals. During week 7, the crista ampullaris, a ridge-like structure composed of neuroepithelial cells, forms at the dilated (ampullated) end of each canal. These ampullated ends open into the utricle. The neuroepithelium and cristae are complete by week 11 .
The utricle (an otolithic organ) develops from the dorsal pouch of the auditory vesicle, whereas the saccule (the other otolithic organ) is derived from the ventral pouch. They begin to develop at about week 6 and are complete by about week 8. Neuroepithelial cells, present in the macula of the utricle and saccule, contain type I and type II hair cells, like the cristae in the semicircular canals. Similar to the cristae, development of this neuroepithelium is complete by week 11 .
The eighth nerve ganglion is formed from cells from the otic vesicle during the fourth week of gestation. The eighth nerve ganglion then divides into the pars superior (which gives rise to the superior branch of the vestibular nerve) and the pars inferior (which becomes the inferior portion of the vestibular nerve and the cochlear nerve). These cells remain bipolar throughout life, with one process terminating in the brain stem and the peripheral part terminating in the sensory areas of the inner ear .
Inner ear development
The inner ear, consisting of the membranous labyrinth surrounded by a bony labyrinth, is adult size at the time of birth (except for changes in the periosteal layer and continued growth of the endolymphatic system). The membranous labyrinth (utricle, saccule, semicircular ducts, endolymphatic sac and duct, and cochlear duct), which is filled with endolymph, resides within the bony labyrinth, which is filled with perilymph. At 22 days of development, surface ectoderm on each side of the rhombencephalon thickens to form the otic placodes, which subsequently invaginate and form otocysts (otic and auditory vesicles), separating from the overlying ectoderm. Each vesicle divides into a ventral component that gives rise to the saccule and cochlear duct and a dorsal component that forms the utricle, semicircular canals, and endolymphatic duct. These epithelial structures are known as the membranous labyrinth .
In the sixth week of development, the cochlear duct forms from a tubular outgrowth of the saccule and penetrates surrounding mesenchyme to complete 2.5 turns by 8 weeks ( Fig. 2 ). The ductus reuniens is the remaining stalk that connects the saccule and the newly formed cochlear duct. The mesenchyme surrounding the cochlear duct differentiates into cartilage, and in the 10th week, this cartilaginous shell undergoes vacuolization to create the scala vestibuli and scala tympani, both perilymph spaces. The epithelial cells of the cochlear duct differentiate into an inner ridge (eventual spiral limbus) and outer ridge (eventual organ of Corti). The cells in these two ridges secrete a gelatinous substance that becomes the tectorial membrane . The cochlear modiolus, carrying the cochlear nerve, develops from membranous bone ( Fig. 3 ). Bone deposition occurs within the modiolus between 20 and 21 weeks between the basal and second turns of the cochlea, and by week 25, ossification is nearly complete .
The semicircular canals begin as evaginations of the utricular part of the otic vesicle during the sixth week. The walls of these outpocketings come into contact with one another to create three semicircular canals. During week 7, the crista ampullaris, a ridge-like structure composed of neuroepithelial cells, forms at the dilated (ampullated) end of each canal. These ampullated ends open into the utricle. The neuroepithelium and cristae are complete by week 11 .
The utricle (an otolithic organ) develops from the dorsal pouch of the auditory vesicle, whereas the saccule (the other otolithic organ) is derived from the ventral pouch. They begin to develop at about week 6 and are complete by about week 8. Neuroepithelial cells, present in the macula of the utricle and saccule, contain type I and type II hair cells, like the cristae in the semicircular canals. Similar to the cristae, development of this neuroepithelium is complete by week 11 .
The eighth nerve ganglion is formed from cells from the otic vesicle during the fourth week of gestation. The eighth nerve ganglion then divides into the pars superior (which gives rise to the superior branch of the vestibular nerve) and the pars inferior (which becomes the inferior portion of the vestibular nerve and the cochlear nerve). These cells remain bipolar throughout life, with one process terminating in the brain stem and the peripheral part terminating in the sensory areas of the inner ear .
Anomalies of the middle ear
Congenital atresia of the external auditory canal and the spectrum of microtia and anotia are discussed elsewhere in this issue. In severe cases of external auditory canal atresia, a bony plate replaces the tympanic ring and forms the lateral wall of the middle ear cavity. It is important to recognize that external auditory canal atresia can be associated not only with pinna abnormalities but also with middle ear abnormalities. Because the external and middle ear share a common embryologic derivative—the first and second branchial arch—external ear abnormalities are often associated with middle ear abnormalities. A classification and scoring system to evaluate the severity of the middle ear abnormalities has been developed by Jahrsdoerfer but is beyond the scope of this article. This scoring system is ideally used to assess surgical candidacy and potentially predict postoperative success.
Ossicular abnormalities are numerous and include absent or maldevelopment of any of the ossicles, with subsequent altered anatomy of other middle ear structures (such as the course of the facial nerve). Malleus head fixation, possibly the most common ossicular abnormality, occurs secondary to incomplete pneumatization of the epitympanum.
Congenital absence of the long process of the incus, which results in a near maximal conductive hearing loss, has been reported. The mode of transmission in a pedigree of three female patients was autosomal dominant mutation or X-linked dominant inheritance . The authors’ institution reported a rare case of isolated, congenital, bilateral absence of the incus in a 3-year-old . In the reported cases, the use of middle ear prosthesis to reconstruct the ossicular chain has been successful in improving the hearing.
Congenital stapes disorders are often related to aberrant facial nerve development. During the crucial time period of 6 weeks post fertilization, if the facial nerve is displaced anteriorly, then the stapes are prevented from coming in contact with the otic capsule, resulting in a malformed stapes. Isolated congenital stapes ankylosis is a rare but reported entity that must be considered in a child who has a stable conductive hearing loss without other associated middle ear pathology . An association of stapes fixation with perilymphatic gusher and profound or mixed hearing loss has been identified as an X-linked inheritance pattern within gene POU3F4 .
Isolated atresia of the oval window has been reported and can best be identified by high-resolution CT imaging in patients who have congenital conductive hearing loss . A temporal bone study of nine patients noted oval window atresia to be associated with an aberrant course of the facial nerve, a malformed incus, and displaced stapes . These patients had audiograms consistent with a conductive, sensorineural, or mixed hearing loss pattern; the role of imaging in establishing the diagnosis was essential . Imaging with high-resolution CT should be strongly considered when a diagnosis of congenital conductive hearing loss is suspected .
Persistent stapedial artery has an interesting embryologic background. At approximately 10 weeks’ gestation, the stapedial artery—a remnant of the second branchial arch—regresses, leaving the normally stirrup-shaped stapes. When this regression does not occur, the persistent artery travels above the stapes footplate, between the anterior and posterior stapes crura, to the fallopian canal toward the geniculate ganglion and dura. During a middle ear exploration for presumed otosclerosis or potential cochlear implantation, the surgeon must be aware of this potential embryologic maldevelopment. The course of the carotid artery may be altered when a persistent stapedial artery is identified; the carotid may be tethered by the stapedial artery and it may be more lateral and posterior than normal. Physical examination in patients with a persistent stapedial artery may show a pulsatile mass in the mesotympanum . CT imaging findings of persistent stapedial artery include absence of the foramen spinosum on the ipsilateral side and abnormal soft tissue in the region of the tympanic segment of the facial nerve . In one series, three of five cases of persistent stapedial artery were associated with an aberrant course of the internal carotid artery .
In addition to ossicular abnormalities, congenital cholesteatoma is attributed to alteration in normal embryologic development. The finding of a cholesteatoma in the anterior mesotympanum is controversial, although most investigators believe it is due to the epithelial rest theory in which there is failure of atrophy of epidermoid rests . Epidermoid formation occurs during 10 to 33 weeks’ gestation and subsequently involutes. The epidermoids persist as collections of stratified squamous epithelium in the anterior-superior portion of the middle ear and tympanic membrane and, when they produce keratin, congenital cholesteatoma develops .
A high-riding jugular bulb may be seen in asymptomatic patients or in patients who have a conductive hearing loss. It presents as a bluish hue behind an intact tympanic membrane and may be mistaken for a middle ear effusion. Patients may also complain of a venous hum or debilitating tinnitus. Selective ligation of the jugular vein has been noted to result in cessation of tinnitus in some patients . CT scan can differentiate between middle ear effusion and a high-riding jugular bulb.
Congenital perilymphatic fistula has been associated with Mondini’s deformity of the cochlea . Sites of fistula include the oval window, fundus of the modiolus, fissulae ante fenstram, and round window . Patients who have congenital perilymphatic fistula are at increased risk for bacterial meningitis . Symptoms include fluctuating or progressive sensorineural or mixed hearing loss and intermittent unsteadiness or vertigo.
Middle ear exploration for anomalies of the middle ear
A study of the findings of middle ear explorations in 67 patients from the Hospital for Sick Children revealed 19 cases of stapes fixation and 42 patients who had ossicular malformation without stapes fixation . Almost one half of operative patients showed no improvement in the air-bone gaps postoperatively . Two thirds of patients who had a mobile stapes had a postoperative air-bone gap less than 30 dB.
An interesting association of middle and inner ear abnormalities in infants who had congenital heart defects was noted by Ulualp and colleagues . Their study examined the histopathology of temporal bones in infants who had syndromic and nonsyndromic congenital cardiac defects and noted that middle and inner ear anomalies included malformed stapes, persistent stapedial artery, dehiscent facial nerve canal, and outer hair cell loss.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


