Esophageal Atresia & Tracheoesophageal Fistula
- Coughing, cyanosis, or vomiting with onset of feeds.
- Association with VACTREL.
- Inability to pass the feeding tube.
- Orogastric tube curled in upper chest or neck on chest -x-ray.
- Intestinal gas indicates esophageal atresia with tracheoesophageal fistula; no gas represents isolated esophageal atresia.
Esophageal atresia and tracheoesophageal fistula (TEF) have a prevalence of 1 in 3000 live births. The male-to-female ratio is equal. Infants with these conditions are often premature, and polyhydramnios is commonly diagnosed prenatally.
Esophageal atresia and TEF are classified based on the presence of atresia and the relation of the fistula location to the atresia. Older classification methods have been replaced with anatomical descriptions (Figure 35–1). The incidence of these two conditions is found in Table 35–1.
Figure 35–1.
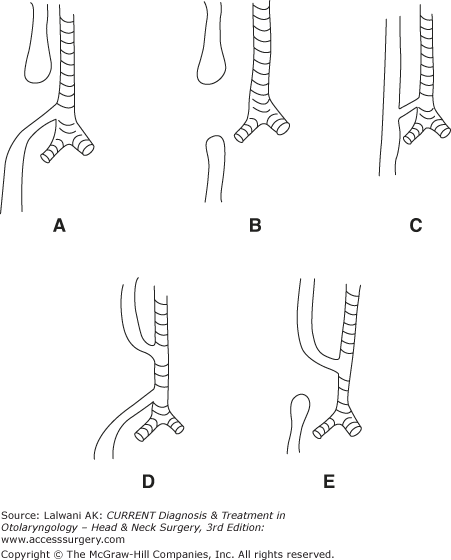
Types of esophageal atresia and tracheoesophageal fistula. (A) Type 1, esophageal atresia with distal tracheoesophageal fistula; (B) Type 2, esophageal atresia without tracheoesophageal fistula; (C) Type 3, tracheoesophageal fistula without esophageal atresia; (D) Type 4, esophageal atresia with proximal and distal tracheoesophageal fistula; and (E) Type 5, esophageal atresia with proximal tracheoesophageal fistula.
| Atresia with distal TEF | 85.4% |
| Atresia without TEF | 7.3% |
| TEF without atresia | 2.8% |
| Atresia with proximal and distal TEF | 2.1% |
| Atresia with proximal TEF | <1.0% |
Types of esophageal atresia and tracheoesophageal fistula: (A) Type 1, esophageal atresia with distal tracheoesophageal fistula; (B) Type 2, esophageal atresia without tracheoesophageal fistula; (C) Type 3, TEF without esophageal atresia; (D) Type 4, esophageal atresia with proximal and distal tracheoesophageal fistula; and (E) Type 5, esophageal atresia with proximal tracheoesophageal fistula.
Esophageal atresia with a distal TEF is the most common anomaly, comprising 85.4% cases. The lower esophageal segment begins as a fistula that arises from the distal trachea near the carina. The proximal esophageal pouch is found as a blind-ending segment near the thoracic inlet. The blood supply to the superior esophageal segment is via the thyrocervical trunk, whereas branches of the gastric arteries supply the distal esophageal segment.
Isolated esophageal atresia comprises 7.3% of cases. The lower pouch is usually only 1–2 cm above the diaphragm, whereas the upper pouch ends near the thoracic inlet, creating a long gap between the two ends that can complicate repair. This anomaly does not allow amniotic fluid to pass to the remainder of the developing gut, explaining the finding of polyhydraminos prenatally. However, esophageal atresia with a relatively narrow distal TEF can produce similar findings.
Isolated trasheoesophageal fistula is the third most common anomaly, comprising 2.8% of cases. The location of the fistula is variable, occurring between the cricoid cartilage and carina. More than one fistula can occur. The fistula angles downward from the trachea to the esophagus.
Esophageal atresia with proximal and distal TEF is less common and comprises 2.1% of cases.
Esophageal atresia with proximal TEF is the least commonly encountered anomaly, comprising <1% of cases. The fistula angles downward from the trachea to the esophagus. The space between the two esophageal ends is pronounced.
By the 26th day of embryologic development, the dorsal foregut has separated from the ventral trachea. A primary mechanism of esophageal atresia develops by an unknown etiology. Animal models demonstrate a branch of a tracheal trifurcation growing caudally, which connects to the stomach, creating the fistula. Esophageal atresia and tracheoesophageal fistula, seen in association with other embryologic abnormalities, is referred to by the acronym VACTERL (vertebral, anal, cardiac, tracheoesophageal, renal, and limb abnormalities). Patients with esophageal atresia and tracheoesohpageal fistula have approximately a 50% chance of having one of these associated anomalies, prompting the physician to rule out these other processes. Cardiac anomalies are the most commonly associated defects.
The esophagus of patients with esophageal atresia and TEF has a decreased number of Auerbach plexuses, explaining the neuronal element of altered esophageal motor function and partly explaining the chronic nature of dysmotility seen with these patients.
Pulmonary development may be impeded via two pathways. Firstly, direct pressure on the trachea by a distended proximal esophagus can contribute to tracheomalacia. Secondly, a fistula drains amniotic fluid out of the pulmonary tree. This fluid pressure has been implicated in playing a part in the parenchymal lung development.



