INTRODUCTION
Embryologic developmental anomalies are fairly common in the pediatric population. Failure of involution embryologic structures and duplication of structures can lead to fistulas, sinuses, and cysts. These include first, second, third, and fourth branchial cleft anomalies (BCAs), as well as preauricular cysts and sinuses and thyroglossal duct cysts (TGDCs). A fistula has an opening from the pharynx to the skin. A sinus is an incomplete fistula and has an opening to either the pharynx or skin. A cyst is an enclosed structure with no opening to the pharynx or skin. Failure of migration or incomplete or excessive migration of embryologic structures results in ectopic structures such as lingual thyroid and ectopic thyroid. Failure of involution of the embryologic thyroglossal duct leads to formation of TGDCs anywhere along the pathway from the base of tongue, submental region, and the anterior neck. Dermoid and epidermoid cysts arise from ectodermal tissues. They represent early embryonic displacements of epithelial nests.
These congenital anomalies may remain asymptomatic, not be obvious on clinical exam, and never require any treatment. Alternatively, enlargement of the lesion may lead to concern for possible malignancy or cosmetic deformity. Mild infections, drainage, or abscess formation may also occur. Enlarging and infected lesions and lesions that interfere with normal functions are possible indications for surgical excision.
Infected cysts and sinuses may be treated with oral or intravenous antimicrobial agents. More severe infections may require needle aspiration possibly guided by ultrasound or computed tomography (CT). Failure of these lesions to respond to these interventions and severe infections and abscesses may require incision and drainage. However, incision and drainage should be used as the last resort when other lesser measures have failed. The reason for avoiding incision and drainage if possible is to avoid violation of tissue planes and violation of the walls of the congenital anomaly, which may possibly make complete excision at a later date more difficult due to scarring and unclear extent of the lesion. The definitive surgical excision may usually be delayed until 3 to 4 years of age unless the severity warrants earlier excision, which may be necessary at any age.
TGDCs are the most common congenital neck anomaly in children. For BCAs, the second BCA is most common. In a series of 97 BCAs, 18% were first BCAs, 69% were second BCAs, and 7% were third BCAs (
1). Thirty-two percent of these lesions had infections previous to surgery and 71% of those had more than one infection. Fistulas and sinuses were infected more frequently (67%) than cysts (21%).
Diagnostic studies include CT with contrast, magnetic resonance imaging (MRI) with gadolinium contrast, ultrasound, and fine-needle aspiration. Of course the most definitive diagnostic test is surgical excision with pathologic examination.
There have been recent reports showing efficacy of fineneedle aspiration and sclerotherapy for selected second BCAs and TGDCs in adults with OK-432. In one series, 7/12 (58%) BCAs treated with OK-432 had complete resolution of the lesion (
2). In another series, 14/23 (61%) BCAs had complete resolution of the lesion (
3). Unilocular lesions had a higher success rate than multilocular lesions, which had only partial or no response to OK-432. In a third series, OK-432 was successful for resolution for 9/18 (50%) second BCAs and 5/11 (46%) TGDCs (
4). Fever, pain, and odynophagia may occur following OK-432 sclerotherapy.
First Branchial Cleft Anomalies
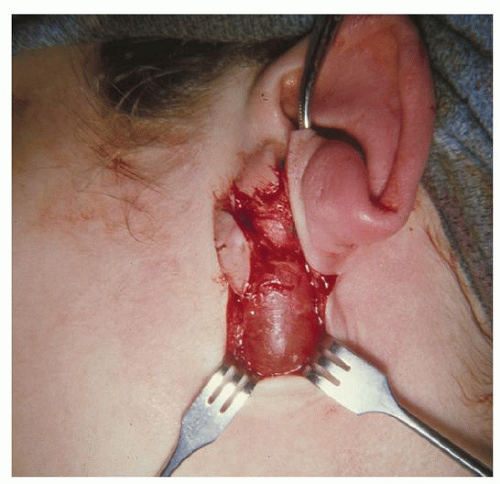
First BCAs are not very common and are often confused with other less complex lesions. Any mass that is located near the lobule of the ear may be a first BCA. The differential diagnosis includes lymph nodes, sebaceous cysts,
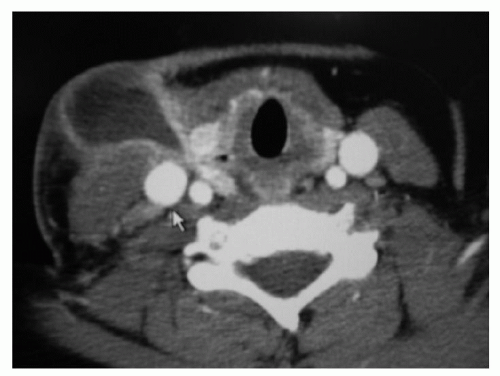
dermoid cysts, lymphatic vascular malformations, and parotid and other tumors. CT and MRI are critical prior to any surgical intervention other than fine-needle aspiration. Solid lesions are likely to be lymph nodes and tumors. Multilocular lesions are likely to be lymphangiomas. Cystic lesions filled with solid rather than fluid material are likely to be dermoids. Fluid-filled cystic lesions may be simple cysts; however, it is possible that the fluid-filled cystic lesion may represent a first BCA (
Fig. 106.1).
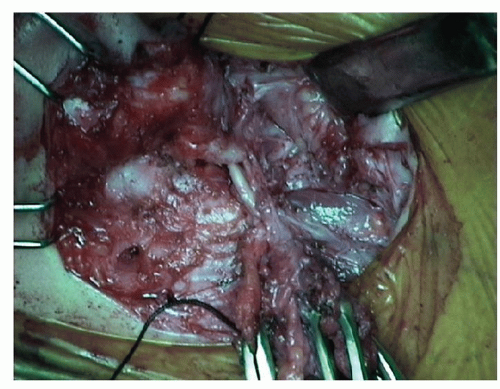
If a first BCA is suspected, and a surgery for removal is planned, the critical point to keep in mind is that there may be a deep portion of the lesion that may run medial or lateral to the main trunk of the facial nerve or between branches (
5,
6). If the deep portion of first BCA lesion is not removed along with the cystic portion, recurrence is likely. Since the deep tract of the first BCA runs in proximity to the facial nerve, injury of the facial nerve is possible unless the facial nerve is first identified and preserved. Then the entire first BCA lesion can be safely removed. Facial nerve monitoring and intraoperative testing are helpful for the dissection (
Fig. 106.2) (
Table 106.1).
Thus, it is wise to suspect that any cystic lesion in proximity to the lobule is possibly a first BCA with a deep tract extending to the facial nerve. The lesion should be approached carefully, and if a deep tract is noted, then the facial nerve is identified and preserved prior to removal of the deep tract.
First BCAs occur in two varieties as described by Work (
7). A Work type 1 first BCA contains only ectoderm, often has a pit in the external auditory canal, and is considered a duplication of the external auditory canal. A Work type 2 lesion will contain derivatives of two germ cell layers, ectoderm and mesoderm.
Since the relationship of the first BCAs and the facial nerve may not be recognized, it is not uncommon for a surgeon to encounter a lesion that recurs following an inadequate resection by another surgeon. In one series of 18 first BCAs, 65% had undergone incomplete surgery prior to referral (
5). The scarring resulting from the first surgery makes the dissection and preservation of the facial nerve more difficult, which may result in a very challenging surgery. Occasionally, a first BCA may present along the anterior border of the sternocleidomastoid muscle slightly lower in the neck than the inferior aspect of the lobule. It is therefore also possible to confuse a first BCA with a second BCA that usually occurs along the anterior border of the sternocleidomastoid muscle in the midneck area.
Second Branchial Cleft Anomalies
Second BCAs are the most common of the three types of branchial cleft lesions. As noted above, these lesions commonly occur along the anterior border of the
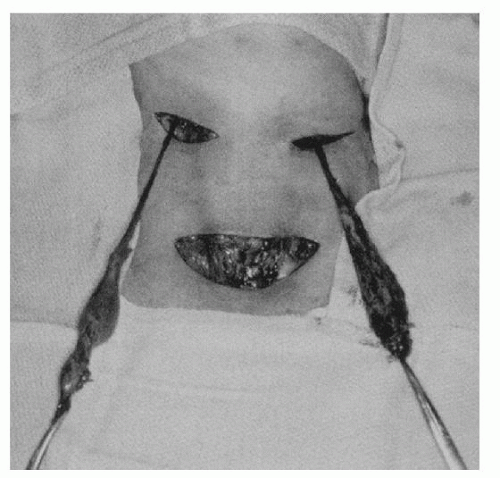
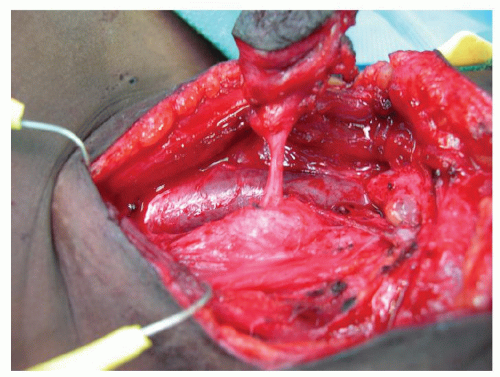
sternocleidomastoid muscle in the midneck region. Like the first BCAs, the second BCAs may also have a deep tract (
Fig. 106.3). It is critical to understand the anatomic path of the second BCAs for safe and complete excision. The deep tact runs between the internal and external carotid arteries and superior to the glossopharyngeal and hypoglossal nerves and finally ends at the tonsillar fossa (
Table 106.1).
A particular cyst or sinus may or may not have a deep extension. The surgeon must be prepared to dissect out a possible deep tract that ends at the tonsillar fossa and then tie off the tract. If the deep portion is not dissected out and excised, recurrence of the lesion is more likely. Gently placing a lacrimal probe into the skin opening of a sinus or fistula can help determine the direction and depth of the tract, which may aid dissection, but care must be taken to avoid rupturing the tract. Other surgeons prefer to inject methylene blue into the tract to aid dissection, but again rupturing the tract can lead to staining of uninvolved tissues and a more difficult dissection. If a branchial remnant is infected, intravenous antimicrobial agents should be administered. If an uninfected lesion is breached, a culture should be taken and intravenous antimicrobials should be administered. Antimicrobials are not required for clean cases with no breach of the lesion.
Although some surgeons advocate excision of the tonsil on the side of the lesion, most surgeons do not excise the tonsil and tie off the tract close to the tonsillar fossa.
Third Branchial Cleft Anomalies
The third and fourth BCAs are rare, often misdiagnosed, and thus often recurrent. The most common presentation is a cystic mass or abscess along the anterior border of the sternocleidomastoid muscle in the mid- to lower neck. Over 90% occur on the left side (
8,
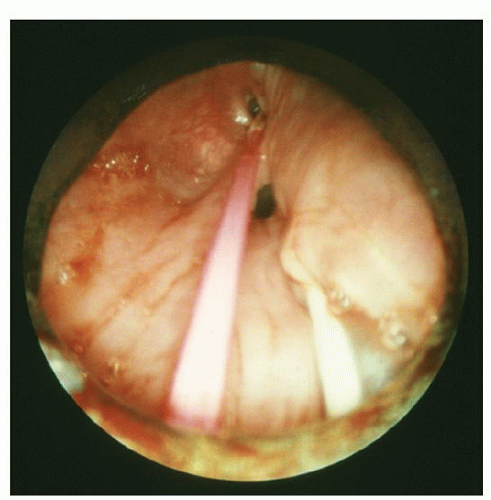
9). These lesions are often misdiagnosed as recurrent neck abscesses or thyroid abscesses or cysts. The key to diagnosis is to understand the potential for these lesions to have a deep tract that extends near the thyroid gland to end as a sinus in the pyriform sinus. Simple incision and drainage often leads to recurrence of the abscesses. The diagnosis is made by several means. One is a thorough pharyngoscopy at the time of incision and drainage that shows a sinus tract in the apex of the pyriform sinus (
Fig. 106.4). CT scan may show an airfilled structure in the apex of the pyriform sinus or a cystic structure with a deep extension approaching the pyriform sinus (
Fig. 106.5). Modified barium swallow may show a barium-filled sinus in the apex of the piriform sinus.
To properly excise the third BCAs, the anatomic course of the tract must be known. The tract of this anomaly passes posterior to the internal and external carotid arteries and between the ninth and twelfth cranial nerves and ends in the apex of the pyriform sinus (
Table 106.1). A small catheter placed in the sinus opening in the apex of the pyriform sinus is helpful prior to excision since palpation of the catheter makes the tract easier to identify during excision (
Figs. 106.4 and
106.6). Hemithyroidectomy may
be required for some third branchial cleft lesions that are intimately associated with the thyroid gland.