Congenital cervical anomalies are important to consider in the differential of head and neck masses in children and adults. These lesions can present as palpable cystic masses, infected masses, draining sinuses, or fistulae. Thyroglossal duct cysts are most common, followed by branchial cleft anomalies, dermoid cysts, and more rarely median cervical clefts. Other topics discussed include median ectopic thyroid, cervical teratomas, and branchiootorenal syndrome. Appropriate diagnosis and management of these lesions requires a complete understanding of their embryology and anatomy. Correct diagnosis, resolution of infectious issues before definitive therapy, and complete surgical excision are essential to prevent recurrence.
Congenital cervical cysts, sinuses, and fistulae must be considered in the diagnosis of head and neck masses in children and adults. These include, in descending order of frequency, thyroglossal duct cysts, branchial cleft anomalies, dermoid cysts, and median cervical clefts. A thorough understanding of the embryology and anatomy of each of these lesions is necessary to provide accurate preoperative diagnosis and appropriate surgical therapy, which are essential to prevent recurrence. The following sections review each lesion, its embryology, anatomy, common presentation, evaluation, and the key points in surgical management.
Thyroglossal duct anomalies
Thyroglossal duct anomalies are the second most common pediatric neck mass, behind adenopathy in frequency . Thyroglossal duct remnants occur in approximately 7% of the population, although only a minority of these is ever symptomatic .
Embryology
The thyroid gland forms from a diverticulum (median thyroid anlage) located between the anterior and posterior muscle complexes of the tongue at week 3 of gestation. As the embryo grows, the diverticulum is displaced caudally into the neck and fuses with components from the fourth and fifth branchial pouches (lateral thyroid anlagen). The descent continues anterior to or through the hyoid bone with the median anlage elongating into the thyroglossal duct ( Fig. 1 ) . By weeks 5 to 8 of gestation, the thyroglossal duct obliterates, leaving a proximal remnant, the foramen cecum, at the base of the tongue and a distal remnant, the pyramidal lobe of the thyroid . If the duct fails to obliterate before the formation of the mesodermal anlage of the hyoid bone, it persists as a cyst .

Clinical presentation and diagnosis
Two thirds of thyroglossal duct anomalies are diagnosed within the first 3 decades of life, with more than half being identified before age 10 years . The most common presentation is that of a painless cystic neck mass near the hyoid bone in the midline ( Figs. 2 and 3 ) . Although they are most commonly found immediately adjacent to the hyoid (66%), they can also be located between the tongue and hyoid, between the hyoid and pyramidal lobe, within the tongue, or within the thyroid . The mass usually moves with swallowing or protrusion of the tongue. Approximately one third present with a concurrent or prior infection, which is the more common presentation in adults . One fourth of patients present with a draining sinus that results from spontaneous drainage or surgical drainage of an abscess . This drainage can result in a foul taste in the mouth if the spontaneous drainage occurred by way of the foramen cecum. These lesions also fluctuate in size. Other rare presentations can be severe respiratory distress or sudden infant death syndrome from lesions at the base of the tongue, a lateral cystic neck mass, an anterior tongue fistula, or coexistence with branchial anomalies .

The preoperative evaluation for a patient who has a suspected thyroglossal duct cyst includes a complete history and physical examination, preoperative ultrasound, and a screening thyroid stimulating hormone (TSH) level. Patients who have history, examination findings, or elevated TSH levels suggesting hypothyroidism or a solid mass should undergo scintiscanning to rule out a median ectopic thyroid . When median ectopic thyroid is present, all of the patient’s functional thyroid tissue can be located within the cyst, and its removal would render the patient permanently dependent on thyroid replacement. The management of median ectopic thyroid is controversial. Some investigators believe these patients can be treated with exogenous thyroid hormone to suppress the gland, whereas others advocate for resection for reasons that are discussed later . Although median ectopic thyroid only occurs in 1% to 2% of thyroglossal duct cysts, some authors advocate for scintiscans in all patients .
Treatment
Elective surgical excision is the treatment of choice for uncomplicated thyroglossal duct cysts to prevent infection of the cyst. The Sistrunk procedure is performed, rather than simple excision, to reduce recurrence risk . With the patient in supine position and the neck extended, a transverse incision is made over the mass. The dissection is carried down to the cyst, then caudally to identify the tract to the pyramidal lobe. If present, it is excised en bloc with the cyst. The surgeon then dissects cranially toward the hyoid bone and a block of tissue around the proximal tract is also excised. The central portion of the hyoid bone is also excised and the tract is further dissected with a core of tissue from the muscle at the base of the tongue to the foramen cecum ( Fig. 4 ) . After confirming adequate proximal dissection by pressure on the base of the tongue from the mouth, the tract is ligated and transected. Intrathyroidal thyroglossal duct cysts should also undergo a Sistrunk procedure if there is a transhyoidal fistulous tract, but can be treated with hemi-thyroidectomy if no tract can be identified .

Infected cysts or sinuses are first managed by relieving the infection. The cysts are usually infected by way of the mouth, thus the most common organisms are Haemophilus influenza , Staphylococcus aureus , and Staphylococcus epidermidis . Antibiotics directed toward those organisms should be started. Needle aspiration may allow for decompression and identification of the organism. Formal incision and drainage should be avoided, if possible, to prevent seeding of ductal cells outside the cyst, which increases recurrence . If incision and drainage is necessary, the incision should be placed so it can be completely excised with an ellipse at the time of definitive resection. Once the infection clears and the incision heals, the patient may undergo an elective Sistrunk procedure .
If a solid mass is encountered during excision of a suspected thyroglossal duct cyst, it should be sent for frozen section to rule out a median ectopic thyroid. If the biopsy returns as normal thyroid tissue and the patient has functional thyroid tissue in the normal location, it should be excised by the Sistrunk procedure . If the mass is possibly the patient’s only functional thyroid tissue, the management becomes controversial. One option involves leaving the ectopic thyroid, either in situ or repositioning it laterally below the strap muscles or into the rectus abdominus or quadriceps muscles. This option aims to not render the patient permanently hypothyroid; however, most patients still require long-term thyroid hormone therapy to treat hypothyroidism or control the size of the ectopic thyroid tissue for cosmetic or functional reasons. This need for long-term therapy and the possibility of malignant degeneration have led some to recommend excision of the median ectopic thyroid regardless of the presence of additional thyroid tissue .
Thyroglossal duct cysts are lined with ductal epithelium or contain solid thyroid tissue. Less than 1.0% have malignant tissue, usually well-differentiated thyroid carcinoma. This malignancy occurs more often in adults, but has been reported in children as young as 6 years old . It is usually identified incidentally at the time of surgery for a suspected thyroglossal duct cyst. Papillary carcinoma is seen most often, although all types of thyroid carcinoma except medullary carcinoma have been reported . If there is no evidence of capsular invasion or distant or regional metastasis, the Sistrunk procedure has been associated with a 95% cure rate, although careful follow-up is necessary . Other investigators recommend completion thyroidectomy regardless of capsular invasion citing the benefits of full pathologic examination of the gland, facilitation of radioactive iodine ablation, and increased sensitivity of radioisotope screening for recurrence . If capsular invasion is present, completion thyroidectomy, nodal dissection, and radioiodine ablation should be pursued as indicated by type and stage of disease .
Recurrence of thyroglossal duct cyst after complete excision using the Sistrunk procedure is reported to be 2.6% to 5% . Several factors have been identified predisposing patients to increased risk for recurrence. Failure to completely excise the cyst (especially simple excision alone) can result in recurrence rates of 38% to 70% . In children less than 2 years old, intraoperative cyst rupture and presence of a cutaneous component increases the risk for recurrence. Preoperative or concurrent infection of the cyst has been historically reported as a risk factor because of the increased difficulty of complete resection, although a recent review found that postoperative infections rather than preoperative infections were associated with increased recurrence . Recurrent thyroglossal cyst excision has a higher risk for recurrence (20%–35%) and requires a wider en bloc resection .
Branchial cleft anomalies
Branchial anomalies compose approximately 30% of congenital neck masses and can present as cysts, sinuses, or fistulae . They are equally common in males and females and usually present in childhood or early adulthood.
Embryology
By the end of the fourth week of gestation, there are four well-defined pairs of arches and two rudimentary arches. These are lined externally by ectoderm, internally by endoderm, with mesoderm in between. The mesoderm contains the dominant artery, nerve, cartilage rod, and muscle for each arch. Each arch is separated by clefts externally and pouches internally. In fish these structures form gills, but in humans the clefts and pouches are gradually obliterated by mesenchyme to form the mature head and neck structures ( Fig. 5 ) . Branchial anomalies result from incomplete obliteration of the clefts and pouches.

Each arch transforms throughout gestation into a defined anatomic pattern. Knowledge of this pattern of transformation and its relationship to normal structures in the neck is essential in the diagnosis and treatment of these anomalies. Branchial anomalies are classified by the cleft or pouch of origin and this is determined by the internal opening of the sinus and its relationship to nerves, arteries, and muscles. A thorough understanding of these relationships is needed to prevent injury to surrounding structures and ensure complete resection . The essential embryology and anatomy is described for each cleft in later discussion.
Pathology
Branchial anomalies can be lined with either respiratory or squamous epithelium. Cysts are often lined by squamous epithelium, whereas sinuses and fistulae are more likely to be lined with ciliated, columnar epithelium . Lymphoid tissue, sebaceous glands, salivary tissue, or cholesterol crystals in mucoid fluid can also be seen. Squamous cell cancer can be found within branchial lesions in adults, although it is rare. It is difficult to distinguish between a primary lesion arising from within an anomaly and a metastatic lesion from an occult primary .
Diagnosis
Branchial anomalies can present as cysts, sinuses, or fistulae. Cysts are remnants of the cervical sinus without an external opening. Sinuses are the persistence of the cervical sinus with its external opening, whereas a fistula also involves persistence of the branchial groove with breakdown of the branchial membrane resulting in a pharyngocutaneous fistula . The specific presentation for each cleft is described in later discussion.
The evaluation of these lesions begins with a complete history and physical, which may include upper airway endoscopy to locate the pharyngeal opening. The pyriform sinus and the tonsillar fossa should be carefully examined. In adults, fine needle aspiration should be performed to rule out metastatic carcinoma or clarify the diagnosis . This clarification is not necessary in children and incisional biopsy should not be performed because this makes the resection more difficult. Ultrasound, CT, and MRI can be used to help define the lesion and its course, but CT is the current study of choice. Current tomography is able to demonstrate the fistula in up to 64% of cases . Barium esophagram can also be helpful with a 50% to 80% sensitivity for third and fourth branchial fistulae .
Treatment
The definitive treatment of all branchial anomalies is complete surgical excision. Unresected cysts and sinuses have a high risk for infection and incomplete resection results in high rates of recurrence . Timing of resection is controversial with some advocating for early resection to prevent infection whereas others support waiting until age 2 to 3 years . Twenty percent of lesions have been infected at least once before the time of surgery . As with thyroglossal duct cysts, acute infections should first be treated with antibiotics, needle aspiration, and, if necessary, incision and drainage, followed by complete resection after resolution of the infection. Specific considerations for the resection of each type of anomaly are discussed later.
First cleft anomalies
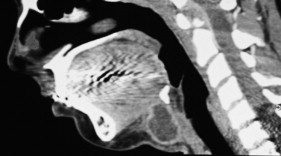
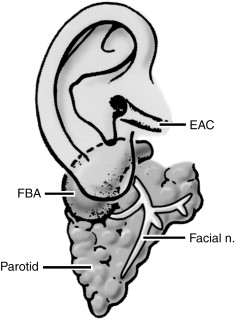
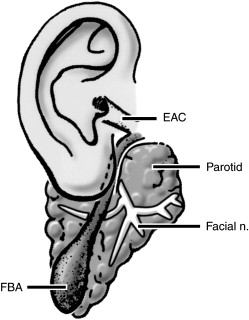
First branchial cleft anomalies account for only 1% of branchial cleft malformations . The first arch, or mandibular arch, forms the mandible, part of the maxillary process of the upper jaw, and portions of the inner ear. The first cleft and pouch form the external auditory canal, eustachian tube, middle ear cavity, and mastoid air cells. First cleft anomalies may involve either the external auditory canal or, occasionally, the middle ear . First cleft anomalies course close to the parotid gland, especially the superficial lobe, traveling above, between, or below the facial nerve branches. First cleft anomalies are classified as Type I or Type II ( Figs. 6 and 7 ). Type I lesions are duplications of the membranous external auditory canal, are composed of ectoderm only, course lateral to the facial nerve, and present as swellings near the ear. Type II lesions have ectoderm and mesoderm, can contain cartilage, pass medial to the facial nerve, and present as preauricular, infra-auricular, or postauricular swellings inferior to the angle of the mandible or anterior to the sternocleidomastoid muscle .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


