Congenital Anomalies of the Nose
John P. Bent
David E. Conrad
Midline congenital nasal lesions are rare, occurring in one out of every 20,000 to 40,000 births (1). Whenever an infant presents with a midline nasal mass, the diagnostic considerations include nasal dermoid, glioma, and encephalocele. These congenital and relatively uncommon lesions share aberrant skull base development, namely, errors in formation of the anterior neuropore. Consequently, the nasal mass often maintains a central nervous system (CNS) connection. As a result, workup must proceed judiciously but promptly, because both reckless and delayed intervention carries risks.
Radiologic advances have tremendously facilitated the management of congenital nasal anomalies. Magnetic resonance imaging (MRI) and/or computed tomography (CT) allows detailed evaluation of the pathology and any associated defects at the skull base. As a result, surgical planning, including the potential role, if any, for the neurosurgeon can be carefully scripted. A variety of approaches gives the surgeon added flexibility, and despite the sensitive location of these defects, most affected children carry an excellent prognosis.
EMBRYOLOGY
To understand the intricacies of congenital midline nasal masses, one must comprehend the normal development of the anterior neuropore (primitive frontonasal region). The two important steps of this process are the formation of the neural tube from ectoderm and the subsequent migration of neural crest cells into mesenchyme to form the skull base and face (Fig. 96.1).
A midline neural groove appears along the dorsal surface of the embryo by the third week of gestation. Shortly thereafter, the ectodermal plate thickens, ultimately forming a neural tube. This precursor to the CNS fuses during the fourth week, with closure beginning in the midportion of the embryo before progressing both anteriorly and posteriorly. Neuropores at the caudal and cranial ends of the neurotube close last. The anterior neuropore, composed of a midline funnel-shaped dural diverticulum, forms at the optic recess of the sphenoid sinus, while the area immediately proximal to the anterior neuropore forms the frontal, nasal, and ethmoid structures.
As neural tube closure progresses, neural crest cells in the lateral portions of the neural tube migrate between the tube and the surface ectoderm into the mesenchyme that will eventually form bone and cartilage. The anterior neuropore is the most distal point of neural crest cell migration; the lack of neural crest cells and the relatively late tube closure predispose this region to developmental defects.
Once neural crest cells migrate into position, underlying mesenchyma organizes into skeletal structures, forming several important spaces (Fig. 96.2):
Fonticulus nasofrontalis—the fontanelle between the inferior frontal and nasal bones
Nasal capsule—the precursor to the nasal cartilages and septum, which is continuous with the ethmoid labyrinth
Prenasal space—between the nasal bones and nasal capsule
Foramen cecum—the region between the ethmoid and frontal bones, which connects with the prenasal space and the location where the cribriform plate condenses
Under normal conditions, these spaces involute during fetal growth.
Whether congenital anomalies of the nose are related to genetic or environmental factors, or both, remains unknown. Laboratory research suggests that extracellular proteins guide the adhesive and migration properties of the neural crest cells (1). Failure of normal neural crest cell embryology may lead to one of the following congenital lesions.
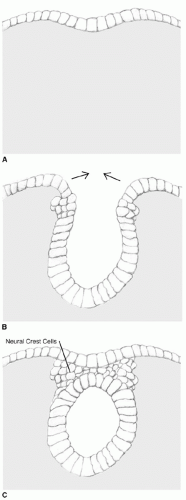 Figure 96.1 Neural tube formation. Dorsal view of embryo with developing neural groove. Note closure in midline first. A: Neural groove. B: Deepening groove. C: Neural tube separated from surface ectoderm; neural crest cells interspersed between surface and neural tube. |
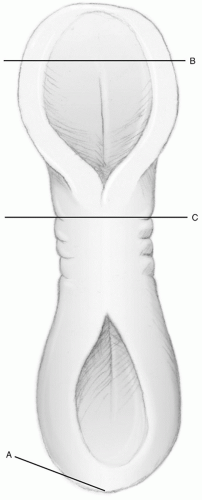 Figure 96.1 (Continued) A. Posterior neuropore, B. Anterior neuropore, C. Surface ectoderm covering neural groove. |
Dermoid
Surface ectoderm and neuroectoderm lie in direct contact before mesenchymal infiltration, particularly at the junction of bone plates. If developing skin adheres to fibrous tissues of the nasal capsule in the prenasal space or fonticulus, it may be drawn posteriorly and superiorly, forming a squamous epithelial lined tract toward the anterior skull base. Animal models suggest that the failure of separation between neuroectoderm and surface ectoderm may involve insufficient apoptotic cell death during the ventrodorsal patterning of the neural tube (2). Aberrant dural attachments could allow a tract connecting skin to the dura via the foramen cecum, surrounded by condensing bone
(Fig. 96.3). Once the tract forms, dermoid cysts may appear anywhere along the pathway. Alternative simplistic theories have suggested that dura becomes entrapped in the fetal septum, or pockets of epithelium become entrapped below the fusing ectoderm (3).
(Fig. 96.3). Once the tract forms, dermoid cysts may appear anywhere along the pathway. Alternative simplistic theories have suggested that dura becomes entrapped in the fetal septum, or pockets of epithelium become entrapped below the fusing ectoderm (3).
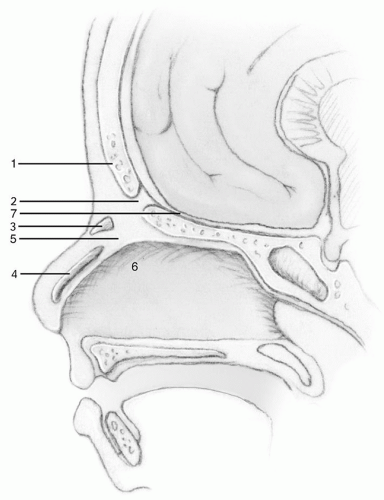 Figure 96.2 Normal embryonic anatomy of nose and anterior skull base. 1, frontal cartilage; 2, fonticulus nasofrontalis; 3, nasal bone; 4, nasal cartilage; 5, prenasal space; 6, nasal capsule; 7, dura. |
Glioma
Several theories also exist as to glioma embryogenesis. According to Gorenstein et al. (4), gliomas most likely form when cranial suture closure isolates brain tissue from the intracranial cavity. The fibrous stalk some gliomas maintain to the CNS supports this theory and suggests a developmental relationship between gliomas and encephaloceles. Less prominent theories of glioma formation include a nidus of ectopic neuroepithelia or an outgrowth of olfactory tissue through the cribriform plate (1).
Encephalocele
Like gliomas, encephaloceles probably originate from faulty closure of the skull; unlike gliomas, with encephaloceles the bone never closes, leaving a persistent intracranial-extracranial defect. As with dermoids and gliomas, the precise cause of this dysmorphism remains elusive. Speculation holds that anywhere along the line of neural tube closure, there may be a barrier or delay in neural crest cell migration. Subsequently, mesenchyme forms improperly, leaving the skull base open and allowing herniation of neural tissue (5). Because the midline is the furthest point of migration, this region naturally comprises the site of such defects. Figure 96.4 depicts the parallel between glioma and encephalocele formation.
CLINICAL AND PATHOLOGIC FEATURES
Dermoids contain both mesodermal and ectodermal components and, consequently, may have hair follicles, sweat gland, smooth muscle, and sebaceous tissue, in addition to their squamous epithelial lining. Nasal dermoid cysts represent approximately 8% to 10% of head and neck dermoids and 1% of all dermoids (6). Most dermoids have a sinus tract exiting via a minute skin opening along the nasal midline (Fig. 96.5). This feature distinguishes it from epidermal inclusion cysts, which also lack mesodermal components. The tract usually contains one, but occasionally
there are multiple cysts along its pathway. It may manifest cutaneously anywhere from the glabella to the columella but most typically exits over the dorsum at the osteocartilaginous junction. Craniofacial abnormalities, such as craniosynostosis, cleft lip and palate, and hemifacial microsomia, may also be present (7). Presenting symptoms may include a localized mass lesion over the nasal dorsum, erythema and tenderness, sebaceous or purulent discharge, or simply parental anxiety about cosmesis. Approximately 50% of patients will have a widened nasal dorsum and hypertelorism (8). The sinus tract may be short and the cyst small, but it may extend to the intracranial cavity through the foramen cecum. Cases with an intracranial connection pose an increased risk of meningitis.
there are multiple cysts along its pathway. It may manifest cutaneously anywhere from the glabella to the columella but most typically exits over the dorsum at the osteocartilaginous junction. Craniofacial abnormalities, such as craniosynostosis, cleft lip and palate, and hemifacial microsomia, may also be present (7). Presenting symptoms may include a localized mass lesion over the nasal dorsum, erythema and tenderness, sebaceous or purulent discharge, or simply parental anxiety about cosmesis. Approximately 50% of patients will have a widened nasal dorsum and hypertelorism (8). The sinus tract may be short and the cyst small, but it may extend to the intracranial cavity through the foramen cecum. Cases with an intracranial connection pose an increased risk of meningitis.
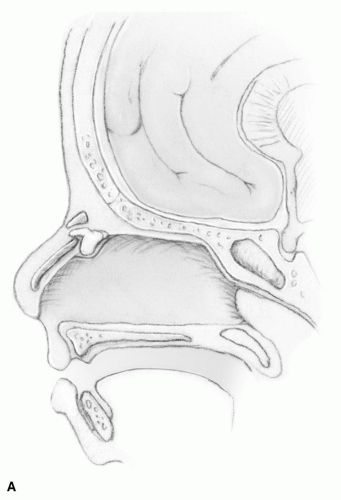 Figure 96.3 Congenital nasal dermoid development. A: Normal closure of fonticulus, foramen cecum, with a sinus tract extending to the beginning of the prenasal space. |
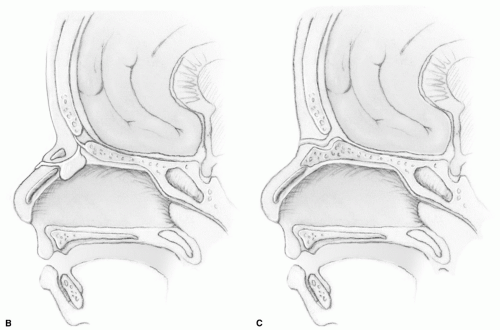 Figure 96.3 (Continued) B: Patent foramen cecum with fistula from the nasal dorsum through prenasal space. C: Patent fonticulus and sinus tract to glabellar skin. |
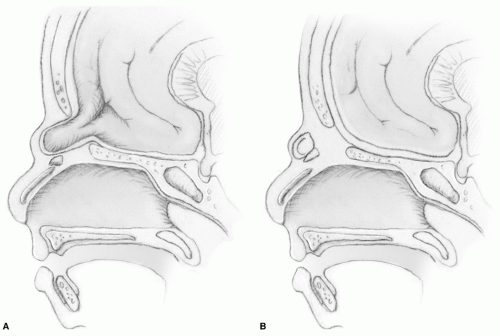 Figure 96.4 Glioma and congenital encephalocele development. A: Herniation of dura and glial tissue (encephalocele) through fonticulus. B: Intranasal glioma with connection to CNS. |
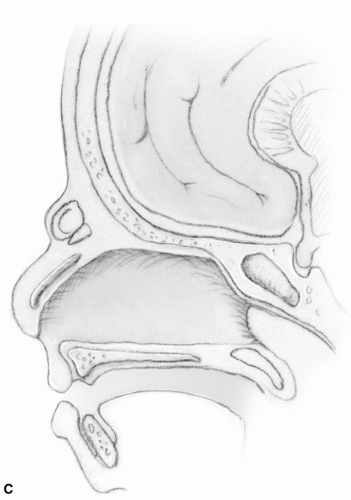 Figure 96.4 (Continued) C: Closure of bones to form glioma. |
Gliomas usually present early in life with symptoms of nasal obstruction. They have a 6:3:1 ratio of extranasal:intranasal:combined lesions (4




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
