Congenital laryngeal anomalies are relatively rare. However, they may present with life-threatening respiratory problems in the newborn period. Associated problems with phonation and swallowing may prevent a baby from thriving. Stridor is the most common presenting symptom of congenital laryngeal abnormalities. Often, it is associated with dysphagia, aspiration, and failure to thrive. Endoscopy is essential for evaluation and diagnosis in most cases. The differential diagnosis includes laryngeal cysts, atresia and stenosis, vocal fold immobility, and subglottic hemangiomas. In this article, the authors discuss in detail the evaluation and treatment for each condition.
Congenital laryngeal anomalies are relatively rare ( Fig. 1 ). However, they may present with life-threatening respiratory problems in the newborn period. Associated problems with phonation and swallowing may prevent a baby from thriving. Stridor is a common presenting sign in laryngeal obstruction . The source of the obstruction can be suspected based on the characteristics of the stridor. Supraglottic or glottic obstruction generally present as inspiratory stridor. Biphasic stridor suggests a narrowing between the glottis and extrathoracic trachea. Turbulent airflow in the distal trachea or main bronchi can produce expiratory stridor.
Embryology
Much of our current understanding of the embryologic development of the larynx comes from the works of Tucker and colleagues , Zaw-Tun and Hollinger and colleagues . Based on the Carnegie staging system, the development of the larynx is divided into two periods: the embryonic and the fetal period . The embryonic period comprises the first 8 weeks of intrauterine development. The larynx first appears around day 25 to 28 of gestation as an epithelial thickening along the ventral aspect of the foregut, called the respiratory primordium. As the respiratory primordium develops, the respiratory diverticulum, an outpouching of the foregut lumen, grows into it. The respiratory diverticulum develops in the area of the primitive pharyngeal floor at the level of the adult glottis. The pharyngeal floor and the primitive pharyngeal floor are divided by the primitive laryngopharynx, which develops into the adult supraglottis.
Over time, the respiratory diverticulum extends inferiorly and is separated from the developing heart and liver by the septum transversum, and from the esophagus by the tracheoesophageal septum. The tracheoesophageal septum grows in a caudal to cranial direction. If cranial advancement is impeded, a tracheolaryngeal or laryngeal cleft or tracheoesophageal fistula may form. Abnormal development of the respiratory diverticulum itself may result in tracheal agenesis, tracheal stenosis, or complete tracheal rings.
Obliteration of the ventral lumen of the primitive laryngopharynx gives rise to the epithelial lamina. Located dorsal to the epithelial lamina is the pharyngoglottic duct, which develops into the interarytenoid notch and posterior glottis. Located anterior to the epithelial lamina is the laryngeal cecum, which becomes the laryngeal vestibule. The epithelial lamina then recanalizes to allow for the laryngeal cecum and the pharyngoglottic duct to unite. Failure to recanalize may result in laryngeal webs or stenosis.
During the fetal period, the vocal processes form from the arytenoids, the goblet cells and submucosal glands develop, and the epiglottic cartilage matures into a fibrocartilaginous structure . The fetal period lasts approximately 32 weeks. Toward the end of gestation, the cricoid cartilage changes from interstitial to perichondrial growth.
Anomalies
Laryngomalacia
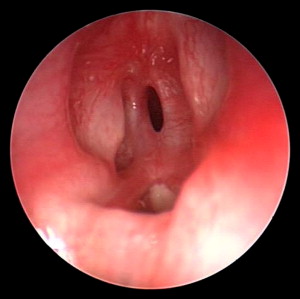
Laryngomalacia is the leading cause of stridor in infants, and accounts for approximately 60% to 75% of congenital laryngeal anomalies ( Fig. 2 ) . Laryngomalacia was first described by Jackson and Jackson in 1942 as a disorder in which supraglottic tissue collapses onto the glottis upon inspiration . This disorder typically produces a high-pitched, inspiratory stridor during the first 2 weeks of extrauterine life and spontaneously resolves by age 12 to 24 months . In severe cases of laryngomalacia, a child may suffer from apneic events, pulmonary hypertension, or failure to thrive. In such cases, surgical intervention is warranted, including supraglottoplasty, division of the aryepiglottic folds, or epiglottopexy .
Laryngomalacia is diagnosed by flexible fiberoptic endoscopy . It is classified as type 1, type 2, or type 3, based on patterns of supraglottic collapse . In type 1 laryngomalacia, redundant supraglottic mucosa prolapses; type 2 is characterized by shortened aryepiglottic folds; and type 3 displays posterior displacement of the epiglottis.
Type 1 laryngomalacia is treated with supraglottoplasty, in which redundant epiglottic, aryepiglottic folds, or arytenoids mucosa is excised . This procedure may be performed using microsurgical instruments, a carbon dioxide (CO 2 ) laser, or the laryngeal microdebrider CO 2 laser supraglottoplasty allows for precise excision of the redundant tissue, with minimal bleeding . Endoscopic supraglottoplasty with a laryngeal microdebrider allows for the negative pressures associated with inspiration to be simulated by suction, and thus allows the surgeon to better visualize and excise the redundant tissue . Type 2 laryngomalacia is treated best with an incision in the aryepiglottic folds to allow expansion of the airway . Typically, a wedge is excised from the aryepiglottic folds; however, Loke and colleagues demonstrated that a simple incision dividing the aryepiglottic folds is sufficient for alleviation of airway obstruction. The division of the aryepiglottic folds may be performed with microlaryngeal scissors or the CO 2 laser. Type 3 laryngomalacia can be treated effectively by way of epiglottopexy, in which the epiglottis is tacked to the base of the tongue, thereby rectifying the posterior displacement of the epiglottis . Not all cases can be classified easily into a single category; thus, a combination of surgical options may be used for treatment.
Gastroesophageal reflux disease (GERD) has been associated with laryngomalacia . It is unclear whether GERD causes laryngomalacia by inducing diffuse edema of the larynx, or laryngomalacia causes GERD by inducing high negative intrapleural pressure and thereby preventing the lower esophageal sphincter from functioning properly. In either case, it is beneficial to treat laryngomalacia patients suffering from GERD with antireflux measures.
Congenital vocal fold immobility
The second most common congenital laryngeal disorder is vocal fold movement disorder, which accounts for approximately 10% to 20% of all congenital laryngeal anomalies Unilateral vocal fold immobility (VFI) typically presents with a weak, breathy cry, feeding difficulties, and aspiration Bilateral VFI, the less common of the two, typically presents with biphasic stridor and a preserved cry . Some neonates with bilateral VFI require intubation at birth because of severe respiratory distress, whereas others have little or no airway compromise.
Most cases of VFI are idiopathic in nature; however, the disorder may result from birth trauma, central or peripheral nervous system anomalies, or cardiovascular anomalies . Central and peripheral nervous system disorders may result in unilateral or bilateral VFI . Central nervous system disorders associated with VFI include brain stem or cerebral dysgenesis, hydrocephalus, encephalocele, leukodystrophy, meningomyelocele, hydrocephalus, spina bifida, cerebral palsy, and Arnold-Chiari malformation (ACM). Though ACM is associated most commonly with bilateral VFI, it can cause unilateral VFI . Peripheral nervous system disorders associated with VFI include myasthenia gravis, fascioscapulohumeral myopathy, and spinal muscular atrophy. Cardiovascular anomalies associated with VFI include ventricular septal defect, Tetralogy of Fallot, cardiomegaly, Ortner syndrome, vascular rings, double aortic arch, and patent ductus arteriosus .
Hereditary bilateral VFI has been identified . In 1978, Mace and colleagues suggested autosomal dominant inheritance in some cases of bilateral VFI. In 2001, Manaligod and colleagues identified chromosome 6q16 as the locus responsible for hereditary bilateral VFI. No genetic cause has been identified in the case of unilateral VFI .
Endoscopy is essential in evaluating the airway and vocal fold motion . A combination of awake flexible laryngoscopy and rigid bronchoscopy under anesthesia has been advocated . In a complete evaluation, the arytenoids should be palpated to determine the mobility of the cricoarytenoid joints . Adjunctive tests include video contrast esophagography to assess swallowing function, and laryngeal electromyography to help differentiate between vocal fold fixation and paralysis . Infants with bilateral, vocal fold movement impairment should undergo cranial imaging (CT, ultrasonography, or MRI) to rule out brainstem pathology, a careful physical examination of the neck, and a chest radiograph or CT to look for mediastinal pathology.
In patients who have VFI secondary to another medical disorder, the underlying cause should be treated . In most cases, idiopathic congenital VFI spontaneously resolves within the first 6 to 12 months of life, although recovery has been documented up to 11 years later . As such, treatment of neonates should be conservative. In cases of significant airway compromise, a tracheotomy may be required until spontaneous recovery of vocal fold motion occurs .
In patients who have unilateral VFI and are prone to aspiration, a nasogastric feeding tube or gastrostomy tube may be placed to ensure adequate nutritional intake . Injection medialization of the paralyzed vocal fold with absorbable gelatin sponge (Gelfoam) or collagen is also effective in reducing aspiration in older children . Type I thyroplasty offers an alternative to injection medialization . Much controversy surrounds the use of these procedures in the pediatric population. In infants and young children, medialization of a paretic vocal fold may worsen in the airway. The effects of medialization laryngoplasty on the growing laryngeal framework are unknown .
In patients who have bilateral VFI, treatment options include vocal fold lateralization, partial cordectomy, arytenoidectomy by way of endoscopic or external approach, and expansion of the cricoid cartilage by way of anterior cricoid split (ACS) with graft placement . Friedman and colleagues have demonstrated the use of the CO 2 laser to perform a posterior transverse partial cordectomy in which a portion of the posterior vocal fold is removed after releasing the vocal ligament and vocalis muscle from the arytenoid cartilage. The CO 2 laser has been used successfully for this procedure in the adult population for many years. It may be a viable option in children with significantly compromised airways and little or no prospect for the return of adequate vocal fold function.
Laryngeal cysts
Laryngeal cysts present with variable degrees of airway obstruction, hoarseness, and dysphagia . DeSanto and colleagues classified laryngeal cysts as saccular, ductal, or thyroid cartilage foraminal cysts. In 1997, Arens and colleagues created a new classification system in which the location of the cyst and histomorphology were taken into consideration. In this classification system, laryngeal cysts were classified as congenital, retention, or inclusion cysts.
Recently, Forte and colleagues proposed a new classification system for congenital laryngeal cysts in an attempt to guide treatment based on classification. In this system, classification is based on the extent of the cyst and the embryologic tissue of origin. Cysts confined to the larynx and consisting of only endodermal elements are classified as type I and can be completely excised endoscopically. Cysts with extralaryngeal extension are classified as type II and typically, for complete excision, an open approach is used. Type II cysts are subdivided further into type IIa and IIb. Type IIa cysts originate embryologically from endodermal elements, whereas type IIb cysts originate from both endodermal and mesodermal elements, as seen in laryngotracheal duplication cysts or diverticula. The authors use the DeSanto classification system in the later discussion.
Saccular cysts
The saccule is a membranous pouch located between the ventricular fold and the inner surface of the thyroid cartilage . The normal mucous membrane surface of the saccule is covered with openings to 60 or 70 mucous glands. Compression of the saccule by surrounding muscles allows these mucous secretions to lubricate the surfaces of the vocal folds.
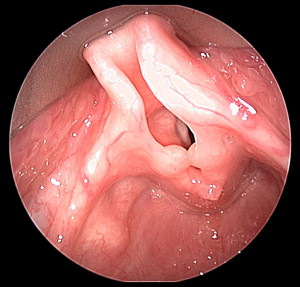
Saccular cysts result from obstruction of the laryngeal saccule orifice in the ventricle, with resultant mucus retention in the saccule ( Fig. 3 ) . Although saccular cysts may be identified radiographically, endoscopy is the gold standard for diagnosis . Endoscopic evaluation reveals a cystic lesion containing thick, mucoid fluid emanating from behind the aryepiglottic fold in the case of lateral cysts, or from the ventricles and protruding into the laryngeal lumen in the case of anterior cysts . Needle aspiration may be useful in diagnosing the lesion, but drainage of the cyst offers only temporary treatment . Marsupialization may be adequate for the treatment of small saccular cysts. However, in the case of recurrence or large cysts, endoscopic or open excision of the cyst is required to remove the cystic tissue completely .

Vallecular cysts
Most neonates with vallecular cysts ( Fig. 4 ) present with stridor within the first few weeks of birth . Other symptoms include cough, feeding difficulties, cyanotic episodes, and failure to thrive. Among the many theories regarding the pathogenesis of vallecular cysts, the most likely states that they are the result of an obstruction of mucosal glands located at the base of the tongue . Mucosal secretions from glands surrounding the cyst cause the cyst to increase in size.

CT may be useful in demonstrating the location and extent of the cyst; however, endoscopy is important in accurately diagnosing vallecular cysts and ruling out other vallecular lesions such as dermoids, teratomas, lingual thyroid, lymphangiomas, or hemangiomas . Endoscopic evaluation reveals a smooth mass localized in the vallecular space. Radionuclide thyroid scans might help to localize functioning thyroid tissue.
Definitive treatment of vallecular cysts consists of endoscopic excision or marsupialization . Aspiration of the cyst may be useful in securing a tenuous airway, but uniformly leads to recurrence.
Thyroglossal duct cysts
Although they are found most commonly in the neck, thyroglossal duct cysts may also present in the vallecula and cause airway obstruction . These cysts are lined by pseudostratified ciliated or squamous epithelium. Adjacent stroma contain mucous glands and thyroid follicles. Histologic identification of thyroid follicles helps to differentiate thyroglossal duct cysts from vallecular cysts.
Ductal cysts
Cysts resulting from an obstruction of submucosal mucous glands are referred to as ductal cysts . These cysts commonly occur in the vallecula and vocal folds. As with other cysts, treatment consists of marsupialization or complete excision of the lesion.
Laryngoceles
Laryngoceles are the result of an abnormal dilation of the laryngeal saccule . Unlike saccular cysts, laryngoceles communicate with the laryngeal lumen . Laryngoceles intermittently fill with air and expand the saccule, which impinges on the laryngeal lumen, causing airway obstruction and a weak cry. The dilated saccule may enlarge and extend into the neck through the thyrohyoid membrane.
Radiographic studies may reveal an air-containing sac in the aryepiglottic fold or out into the neck. Endoscopic evaluation is important to rule out other laryngeal lesions, such as laryngeal duplication cysts, hamartomas, choristomas, and teratomas that may have similar appearances and presentations . Endoscopic marsupialization is sufficient to control most internal laryngoceles . When there is an external component, an open approach may be necessary to remove the lesion completely .
Laryngeal atresia and stenosis
Laryngeal atresia
Laryngeal atresia is an extremely rare condition that results from the failure of the larynx and trachea to recanalize during embryogenesis . Typical presentation at birth is severe respiratory distress despite strong respiratory effort. Laryngeal atresia can be diagnosed prenatally based on ultrasonographic evaluation, by identifying the signs of congenital high airway obstruction syndrome (CHAOS), such as hyperechogenic enlarged lungs, a flattened or inverted diaphragm, a fluid-filled, dilated airway distal to the obstruction, fetal hydrops, and polyhydramnios . Color flow Doppler ultrasonography is useful in localizing the level of the obstruction by detecting the absence of flow in the trachea during fetal breathing.
An emergent tracheotomy is required immediately upon birth to secure an airway. Prenatal diagnosis of CHAOS allows for the use of the ex utero intrapartum treatment (EXIT) procedure to evaluate and secure the airway at birth . In this procedure, placental support is maintained after birth until the airway is secure. Generally, laryngotracheal reconstruction is performed at a later stage .
Associated anomalies include tracheoesophageal fistula, esophageal atresia, urinary tract abnormalities, limb defects, encephalocele, horseshoe kidney, and low-set ears . In neonates with an associated tracheoesophageal fistula, it is possible to secure the airway temporarily by way of esophageal intubation.
Congenital subglottic stenosis
Congenital subglottic stenosis is diagnosed when there is a narrowing of the laryngeal lumen in the cricoid region and no history of intubation or surgical trauma. Most investigators consider a diameter of less than 4 mm in a full-term newborn and 3 mm in a premature infant to be insufficient . However, some investigators quote a diameter of less than 3.5 mm in a newborn . Congenital subglottic stenosis was described by Holinger in 1954 as a malformation of the cricoid cartilage . The transverse and anteroposterior luminal diameters at the midportion of the cricoid cartilage are normally equal . Holinger described an elliptic cricoid cartilage in which the transverse diameter was significantly smaller .
Congenital subglottic stenosis can be classified as either membranous or cartilaginous . Membranous stenosis is the more common and milder type of congenital stenosis. It results from submucosal gland hypoplasia with excessive fibrous connective tissue. Cartilaginous stenosis has three common variants: an abnormally shaped cricoid cartilage with lateral shelves, and an elliptic shape, or a normally shaped cricoid cartilage with a decreased diameter.
Usually, congenital subglottic stenosis is diagnosed in the first few months of life. Symptoms of subglottic stenosis range from mild dyspnea to severe airway obstruction . Stridor tends to be biphasic or primarily inspiratory in nature. In mild cases, symptoms manifest only during respiratory tract infections, when edema and thickened secretions further compromise the airway. Recurrent or persistent croup is a typical finding in children with subglottic stenosis. Children with Down syndrome have a high incidence of congenital airway narrowing . Often, these children are asymptomatic but prove difficult to intubate for anesthesia.
The severity of the subglottic stenosis usually is determined by the Myer-Cotton grading system . Endotracheal tubes of various sizes are placed sequentially, with the second graduated mark at the level of the vocal cords. The endotracheal tube, which results in a leak pressure of less than 30 cm H 2 O, is considered to be the individual’s tube size. The patient’s tube size and age are compared with established norms and a grade is assigned.
Plain radiographs are of limited value in assessing the subglottis . Anterior-posterior cervical airway radiographs reveal a classic hourglass narrowing at the level of the subglottis .
Congenital subglottic stenosis becomes less critical as the larynx grows. Symptoms resolve by a few years of age in most cases . Thus, for grade I stenosis, a watch and wait approach is deemed appropriate . For more severe cases of congenital subglottic stenosis, surgical intervention may be necessary . Fewer than 50% of children require a tracheotomy and most who do can be decannulated once the airway improves sufficiently . Other surgical options, such as anterior laryngotracheal decompression or reconstruction, have been advocated to avoid the potential complications of tracheotomy, including an increased risk of infection, accidental decannulation, tracheotomy tube plugging, and retardation in speech and language development . Dilation and endoscopic laser surgery are ineffective, particularly in cartilaginous stenosis .
Cotton and Seid described the ACS procedure as an alternative to tracheotomy in 1980 . The success rate of this procedure for the treatment of neonates with subglottic stenosis ranges from 58% to 100%, with few complications. The ACS procedure entails the division of the cricoid cartilage, the first two tracheal rings, and the caudal thyroid cartilage in the midline. In 1991, Richardson and colleagues demonstrated that the use of a rib cartilaginous graft in conjunction with ACS resulted in improved efficacy. Since then, auricular cartilage, hyoid bone, and thyroid alar cartilage all have been used to expand the narrowed subglottis .
Subglottic hemangiomas
Hemangiomas are congenital vascular lesions that undergo rapid growth in the first months after birth . Their size stabilizes between 12 and 18 months. Finally, most hemangiomas involute, generally by 5 years of age .
Congenital subglottic hemangiomas are rare, but potentially fatal, lesions ( Fig. 5 ). They account for 1.5% of congenital laryngeal abnormalities . They have a female/male ratio of 2:1 . Presentation may be similar to that of subglottic stenosis, with recurrent croup and biphasic stridor . Other symptoms may include a barking cough, hoarseness, cyanosis, hemoptysis, dysphagia, and failure to thrive . Approximately 50% of infants have cutaneous hemangiomas as well .
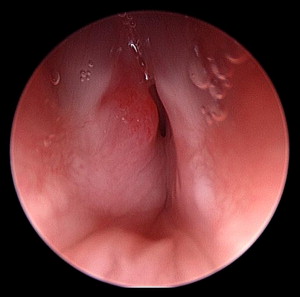
Hemangiomas are suspected by history, physical examination, and, typically, endoscopic appearance . Plain radiographs of the neck may show asymmetric narrowing of the subglottis . Flexible endoscopy may suggest the diagnosis and is useful in ruling out other laryngeal abnormalities . Rigid endoscopy reveals a red-to-blue, compressible, sessile lesion that most commonly is located posterolaterally in the subglottis . Histologic confirmation carries the risk of hemorrhage. Microscopically, hemangiomas are composed of small, thin-walled vessels of capillary size that are lined by a single layer of flattened or plump endothelial cells and surrounded by a discontinuous layer of pericytes and reticular fibers.
Many options are available for the treatment of subglottic hemangiomas. Traditionally, a watchful waiting approach with or without a tracheotomy has been taken . A tracheotomy secures the airway until the hemangioma naturally regresses. With advances in therapy to decrease the size of the lesion, tracheotomy can be avoided and associated complications prevented . Treatment options include radiation therapy, cryotherapy, sclerotherapy, alpha-2A interferon therapy, systemic or intralesional corticosteroid use, open surgical resection, and laser ablation .
Radiation therapy, cryotherapy, and sclerotherapy have been discontinued because of their adverse effects . Radiation therapy was introduced first in 1919 by New and Clark . The treatment showed potential. However, because of the risk of damage to normal airway mucosa and an increased risk of malignancy, the treatment was abandoned in the late 1970s . Cryotherapy was used first by Schechter and Biller in 1972, with transient responses . The extent of tissue damage, however, is unpredictable with this therapy and may result in subglottic stenosis . As such, this therapy has fallen out of favor. Sclerotherapy has been deemed not only ineffective as a cure but also associated with complications such as hemoglobinuria, nerve injury, ulceration, and cardiovascular collapse . Currently, research is being conducted to improve sclerosant agents and delivery methods that would result in greater efficacy and fewer adverse effects.
In 1994, Ohlms and colleagues reported successful treatment of subglottic hemangiomas in eight patients, using interferon alpha-2a. However, this treatment option has fallen out of favor as a first line treatment because of the risk of spastic diplegia .
The use of systemic corticosteroids has been proven effective in 25% of cases . A diminished rate of proliferation, softening of the tumor, and a fading of the color should occur between a few days and a few weeks of initiating therapy . It is important to gradually taper off steroids to prevent rebound growth . This method is most effective for treating small lesions; however, long-term steroid use is not without complications. Adverse effects of long-term use include Cushing’s syndrome, hypertension, immune deficiency, and growth retardation . Intralesional steroid injection has the benefits of systemic corticosteroid therapy without the adverse effects . However, local steroid injection requires multiple treatments .
Open surgical resection for the treatment of subglottic hemangiomas was described first by Sharp in 1949 . Currently, it is recommended for certain airway-threatening lesions, including large, obstructing hemangiomas in the proliferating phase; bilateral subglottic hemangiomas; and hemangiomas with extralaryngeal extension . In 1974, Evans and Todd described surgical excision of hemangiomas followed by laryngotracheoplasty. All three of their patients required a tracheotomy and postoperative stenting. Advances in laryngotracheoplasty procedures allow for open surgical resection to be performed, as either a single-stage procedure with short-term endotracheal intubation or as a staged procedure with delayed decannulation after the subglottis has healed completely .
CO 2 laser ablation in the treatment of subglottic hemangiomas was described by Simpson and colleagues in 1979 . In 1980, Healy and colleagues demonstrated the efficacy of CO 2 laser ablation with one or two applications in 11 patients. This treatment has produced mixed results, ranging from reports of earlier decannulation and low complication rates, to minimal benefits and high complication rates . Complications include significant scar tissue and subglottic stenosis .
The use of the potassium-titanyl-phosphate (KTP) laser has also shown potential in the treatment of subglottic hemangiomas . The KTP laser with a wavelength of 532 nm is absorbed preferentially by hemoglobin. Unlike CO 2 lasers, its light can be transmitted through flexible fiberscopes . The KTP laser has significant tissue penetration and can cause thermal damage to the cricoid and tracheal cartilages . In a series of six patients, Madgy and colleagues reported a grade 1 subglottic stenosis in one patient after laser ablation with a KTP laser.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


