Congenital Abnormalities of the Optic Disk
Gary C. Brown
Melissa M. Brown
VASCULAR ANOMALIES OF THE OPTIC DISK
Prepapillary Vascular Loops
First described by Liebrich in 1871 (1), prepapillary vascular loops were originally thought to be remnants of an incompletely regressed hyaloid system. Most evidence now suggests they occur as a separate entity (2,3,4). Despite the fact these anomalies appear dark, thus venous, approximately 95% of prepapillary loops are arterial (3).
Clinically, the vessels appear as loops that extend from the optic disk into the vitreous cavity and then back to the disk (Fig. 15.1). In contrast to a single hyaloid artery, each prepapillary loop has at least one ascending and one descending branch. Loops can assume a spiral or corkscrew shape, a figure-of-eight appearance, or manifest with a simple hairpin turn configuration (3). Spontaneous movement, coincident with the heartbeat, is seen in approximately half of cases, whereas approximately 30% are encased by a white, glial-appearing sheath (Fig. 15.2).
Arterial prepapillary loops average approximately 1.5 mm in height and project in the vitreous cavity into Cloquet’s canal, rather than into the vitreous gel (3). In contrast to a persistent hyaloid artery, arterial prepapillary loops achieve a maximum height of approximately 5 mm and do not extend anteriorly to the posterior capsule of the lens.
Bilaterality is present in 9% to 17% of cases (2), and cilioretinal arteries have been noted in up to 75% of affected eyes. Systemic associations have not been routinely noted.
Histopathologically, a prepapillary arterial loop has been shown to contain intima, but not an internal elastic lamina (Fig. 15.3) (5). The vessel lies beneath a loose connective tissue sheath continuous with the internal limiting membrane of the retina.
Mann (4) has suggested that prepapillary arterial loops arise at approximately the 100 mm stage (3.5 to 4 months) of gestation. At this time, mesenchymal cells, the precursors of retinal capillary endothelial cells, and retinal vessels, inadvertently grow anteriorly into the supporting tissue of Bergmeister’s papilla overlying the optic nerve head. They then proceed back down onto the disk and on their course into the developing retina. Bergmeister’s papilla subsequently regresses, leaving the vascular abnormality within Cloquet’s canal.
The major complication associated with prepapillary arterial loops is retinal artery obstruction in the distribution of the area supplied by the loop (Fig. 15.4) (2). Reported in approximately 10% of cases of prepapillary loops described in the literature, the obstruction has been hypothesized to occur secondary to turbulent flow, which predisposes to endothelial damage and thrombus formation. Vitreous hemorrhage and hyphema also have been noted (3).
Congenital prepapillary venous loops are usually single vessels that extend 0.5 mm or less into the vitreous cavity (Fig. 15.5). Acquired prepapillary venous loops are more common and often multiple, typically seen in adults, and found in conjunction with retinal venous obstruction or diseases associated with retinal venous obstruction, such as glaucoma, meningioma, or increased intracranial pressure (Fig. 15.6).
Persistent Hyaloid Artery
A persistent hyaloid artery presents clinically as a single vessel traveling from the optic disk—through Cloquet’s canal— anteriorly to the posterior capsule of the lens (Fig. 15.7) (2). The point of attachment to the posterior capsule, most often located inferonasal to the visual axis, is known as Mittendorf’s dot.
Hyaloid artery remnants are seen in the eyes of premature infants in up to 95% of cases, but are observed in only 3% of full-term infants (6). The incidence in children and adults is lower, but exact figures are lacking. Most commonly, a persistent hyaloid artery in a child is bloodless, but in rare instances it can contain blood and be associated with vitreous hemorrhage (7). Ocular associations reported with persistent hyaloid artery include persistent hyperplastic primary vitreous, coloboma of the optic disk, optic nerve hypoplasia, and posterior vitreous cysts (2).
 FIGURE 15.1. Congenital prepapillary arterial loop with a figure-of-eight configuration. |
 FIGURE 15.2. White, fibroglial sheath (arrow) surrounding a prepapillary arterial loop extending into Cloquet’s canal. The cilioretinal artery at the 3:30 o’clock position off the optic disk is sheathed and shows temporal pallor, both occurred secondary toxemia of pregnancy 15 years previously. |
Persistent Bergmeister’s Papilla
Although not a vascular abnormality in the strictest sense, Bergmeister’s papilla develops around the posterior aspect of the fetal hyaloid artery. It is therefore included herein.
Between the first and second months of gestation, neuroectodermal cells within the optic cup at the superior end of the embryonic fissure differentiate into the primitive epithelial papilla (8). This primitive epithelial papilla becomes the optic nerve head when axons traveling from retinal ganglion cells to the respective lateral geniculate nuclei within the thalamus of the brain pass through it.
At the end of the fourth month of gestation, neuroectodermal glial cells on the surface of the optic disk multiply and form a sheath around the hyaloid artery that extends anteriorly for approximately one-third the length of the vessel (Fig. 15.8). The sheath is maximally developed at approximately 5.5 months of gestation, after which atrophy occurs. The degree of regression determines, in part, the physiologic cupping of the optic disk.
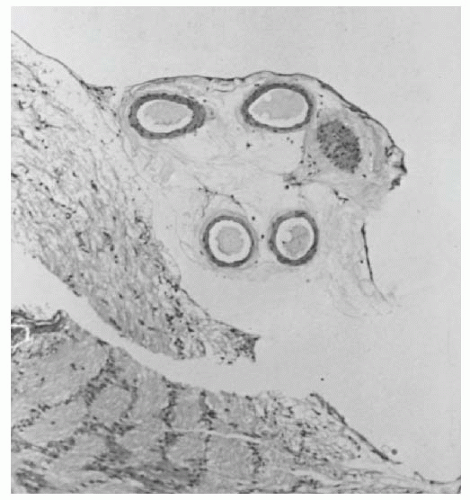 FIGURE 15.3. Histopathology of prepapillary arterial loop. The vessel is located with amorphous connective tissue beneath the internal limiting membrane of Elschnig. |
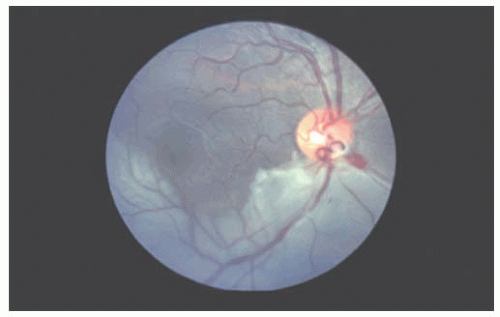 FIGURE 15.4. Inferior branch retinal artery obstruction in the right eye of an 18-year-old youth with a prepapillary arterial loop. (Reprinted from Brown GC, Magargal LE, Augsburger JJ, et al. Preretinal arterial loops and retinal arterial occlusion. Am J Ophthalmol 1978;87:646-651, with permission of Ophthalmic Publishing Company.) |
Incomplete regression of Bergmeister’s papilla causes a persistent Bergmeister’s papilla, also known as epipapillary veil. Clinically, the entity appears as a tuft of glial tissue most commonly located on the nasal aspect of the nerve head (Fig. 15.9). Absence of physiologic cupping can also be seen in affected eyes. The visual acuity is unaffected by the abnormality, and systemic associations are generally lacking.
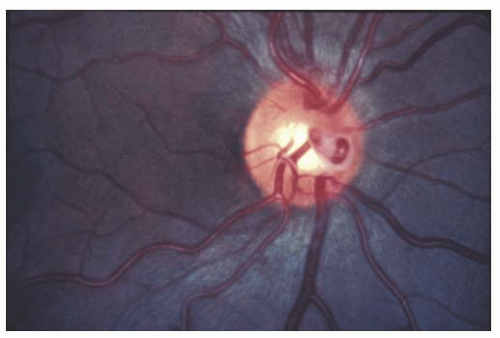 FIGURE 15.5. Single congenital prepapillary venous loop in the right eye on the nasal side of this right optic disk. The white fibroglial tissue overlying the loop has the clinical appearance of a Bergmeister’s papilla. (Reprinted with permission from Brown GC, Tasman WS. Congenital anomalies of the optic disc. New York: Grune & Stratton, 1983:53.) |
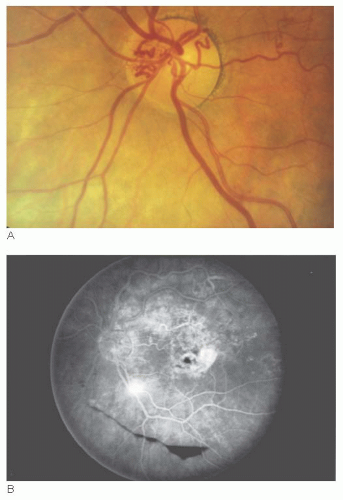 FIGURE 15.6. A: Multiple acquired prepapillary venous loops. B: Fluorescein angiogram corresponding to (A) reveals evidence of a previous superotemporal retinal branch vein obstruction. (Reprinted with permission from Brown GC, Tasman WS. Congenital anomalies of the optic disc. New York: Grune & Stratton, 1983:54-55.) |
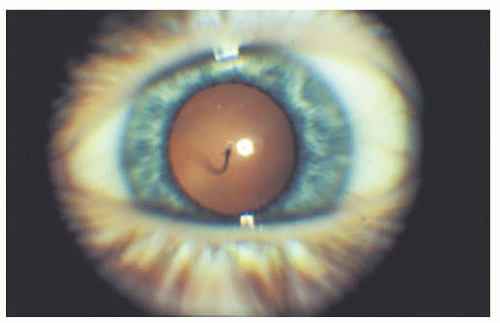 FIGURE 15.7. Single loop of a persistent hyaloid artery extending anteriorly within Cloquet’s canal to insert on the posterior capsule of the lens. |
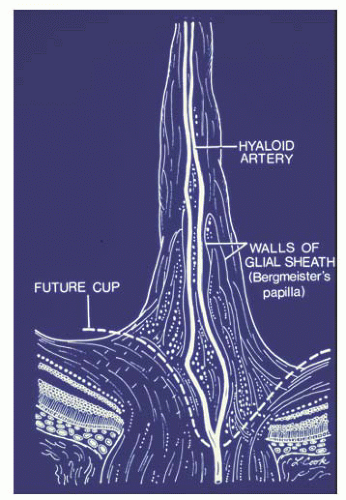 FIGURE 15.8. Bergmeister’s papilla at its maximum height during the fifth month of gestation. It usually regresses by birth. The dotted white line shows the future cup of the optic disk. |
Enlarged Vessels
Causes of enlarged vessels on the optic disk in children include arteriovenous (AV) malformations, retinal capillary hemangiomas (von Hippel tumors), and retinoblastoma. Because the latter two conditions are most appropriately classified as tumors, they will not be addressed in this section. Choroidal melanoma also has been noted to cause enlarged vessels on the optic disk (9), but the tumor is generally not seen in children.
AV malformations in the retina can be mild, moderate, or severe, and thus have been correspondingly classified by Archer and associates (10) as grades I, II, and III abnormalities. A grade I AV communication, the mildest variant, has also been called a congenital retinal macrovessel by Brown et al.
(11). A congenital macrovessel is a single enlarged retinal vessel, usually a vein, that traverses both sides of the horizontal raphe (Fig. 15.10). Some of these vessels are associated with readily apparent AV communications, whereas others are not. Transient cysts in the central fovea have been seen in association with congenital retinal macrovessels, but appear to affect the visual acuity minimally.
(11). A congenital macrovessel is a single enlarged retinal vessel, usually a vein, that traverses both sides of the horizontal raphe (Fig. 15.10). Some of these vessels are associated with readily apparent AV communications, whereas others are not. Transient cysts in the central fovea have been seen in association with congenital retinal macrovessels, but appear to affect the visual acuity minimally.
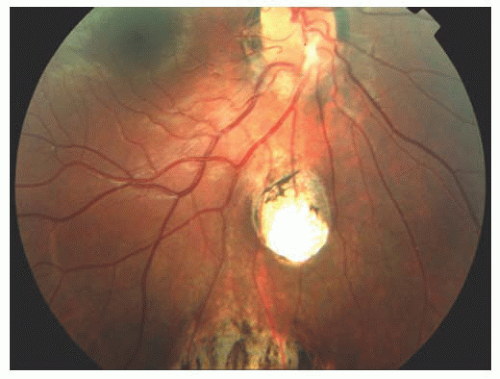 FIGURE 15.9. Yellowish, persistent Bergmeister’s papilla (star) overlying the inferonasal optic disk. Incomplete retinochoroidal colobomatous lesions are present inferior to the optic disk. |
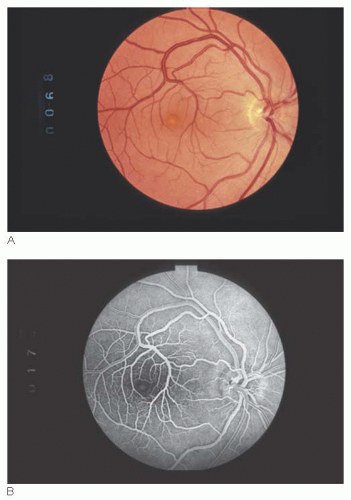 FIGURE 15.10. A: Congenital retinal macrovessel. Enlarged vein drains the retina, both superior and inferior to the horizontal raphe. Visual acuity in the eye was 20/20, despite the presence of a yellow foveolar cyst. B: Fluorescein angiogram of the central macula seen in (A). The small circular area of central hyperfluorescence in the foveal avascular zone corresponds to the retinal cyst. Vessel forming the superior border of the foveal avascular zone is an arteriovenous (AV) communication. |
Grade II and III AV communications have also been called racemose angiomas or racemose hemangiomas. The grade II variant is moderate and is usually associated with normal vision (Fig. 15.11), whereas with grade III AV communications the vision can be severely reduced due of replacement of optic nerve tissue by enlarged vascular elements (Fig. 15.12) (12,13). Both grade II and III AV communications can be associated with AV communications in the face, scalp, mandible, and central nervous system. The eponym Wyburn-Mason syndrome has been applied to retinal AV communications associated with systemic AV
communications (14). Rundles and Falls (15) found that, among 34 cases of congenital retinal AV malformations reported through 1951, 18 (53%) had associated central nervous system and/or dermatologic involvement.
communications (14). Rundles and Falls (15) found that, among 34 cases of congenital retinal AV malformations reported through 1951, 18 (53%) had associated central nervous system and/or dermatologic involvement.
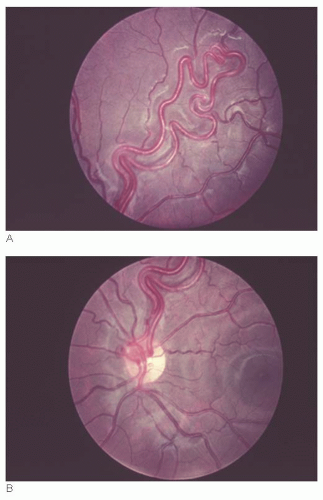 FIGURE 15.11. Grade II arteriovenous (AV) communication in a 12-year-old boy. Visual acuity in the eye was 20/20. (Reprinted with permission from Brown GC, Tasman WS. Congenital anomalies of the optic disc. New York: Grune & Stratton, 1983:75.) |
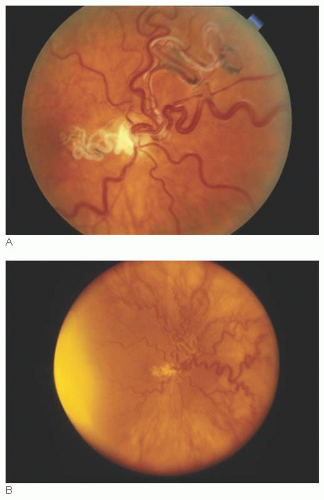 FIGURE 15.12. A: Grade III arteriovenous (AV) communication. Visual acuity in the eye was no light perception, presumably because of the replacement of the normal optic nerve tissue by vessel (courtesy of Dr. Jerry A. Shields). B: Grade III AV communication shown in (A) with equator-plus photography. Multiple AV communications are present. The patient also had a maxillary AV communication that caused severe bleeding after tooth extraction. The yellow illuminating light is at the left of the photograph (courtesy of Dr. Jerry A. Shields). |
COLOBOMATOUS AND OTHER EXCAVATED DEFECTS
Congenital Pit of the Optic Disk
Found in approximately 1 per 11,000 patients (16), a congenital pit of the optic nerve head appears as a localized depression that can be yellow-white (Fig. 15.13), gray (Fig. 15.14), black (Fig. 15.15), or other variants in color.
The defects generally range in size from 0.25 to 0.40 disk diameters. More than 50% are located on the temporal aspect of optic disk, versus inferiorly, nasally, or centrally (Fig. 15.16). Although found anywhere on the optic disk, they occasionally have a peripapillary location.
The defects generally range in size from 0.25 to 0.40 disk diameters. More than 50% are located on the temporal aspect of optic disk, versus inferiorly, nasally, or centrally (Fig. 15.16). Although found anywhere on the optic disk, they occasionally have a peripapillary location.
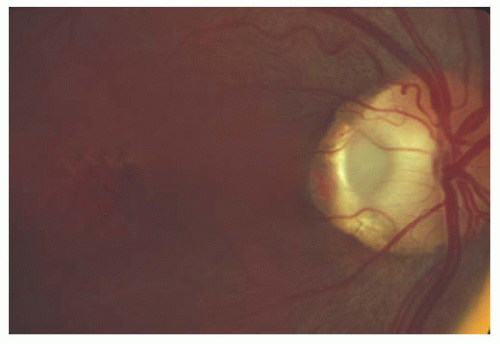 FIGURE 15.13. Right eye of a patient with a yellow/white, temporal congenital optic pit and prominent, peripapillary, retinal pigment epithelial changes adjacent to the pit. A serous detachment of the sensory retina involves the macular, and a lamellar macular hole is present with the internal limiting membrane intact over it. (Reprinted with permission from Brown GC, Tasman WS. Congenital anomalies of the optic disc. New York: Grune & Stratton, 1983:107.) |
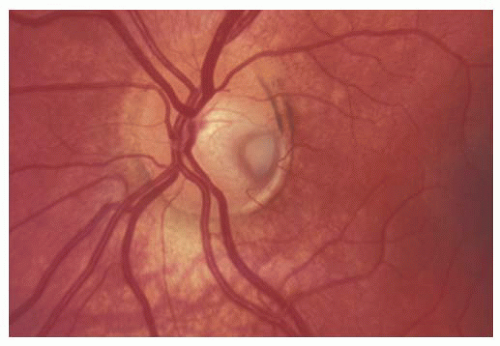 FIGURE 15.14. Gray congenital pit of the optic nerve head with peripapillary atrophy. |
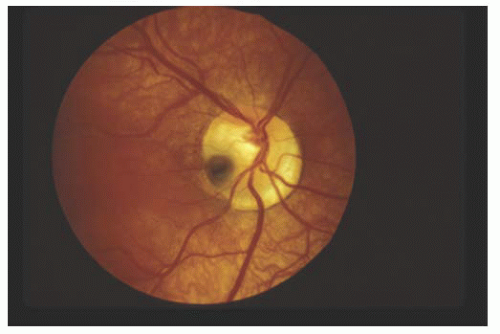 FIGURE 15.15. Black congenital pit of the optic nerve head with an adjacent macular retinal detachment. The background choroidal vessels are more obscured in the region of the retinal detachment. |
Peripapillary retinal pigment epithelial disturbances are present in 95% of eyes with optic pits that are not centrally located (see Fig. 15.13) (17). Peripapillary choroidal neovascularization has been seen rarely in these cases (18). In unilateral cases, the nerve head with the pit is larger than a normal contralateral nerve head in 85% of patients. Most pits are single, but approximately 5% of affected eyes have more than one defect on the disk. Cilioretinal arteries are frequently associated.
Approximately 40% of eyes with a congenital optic pit have an associated or previous serous detachment of the sensory retina and/or posterior retinoschisis (see Fig. 15.13) (17




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
