space contains fat and the infraorbital nerve and vessels. The medial extraconal space is the most relevant space in sinus surgery and contains a plethora of vascular structures: distal portions of the posterior ethmoidal artery, the distal portion of the ophthalmic artery, and the anterior ethmoidal artery as well as fat. Of extreme importance is the relationship of the ophthalmic artery and the anterior ethmoidal artery. The ophthalmic artery courses anteriorly in the extraconal space just inferior to the superior oblique muscle before giving rise to the anterior ethmoidal artery near the anterior ethmoidal foramen along the medial orbital wall. Radiographically, this is best identified in the coronal plane along the convergence of the medial rectus muscle and the superior oblique muscle (Fig. 44.1). In approximately 10% of cases, this neurovascular bundle can be suspended from the anterior ethmoid skull base in a bony mesentery, often associated with a supraorbital ethmoid air cell (1). Considering the limen nasi as a fixed landmark, the artery is located approximately 55 degrees from the nasal floor and at 50 mm.
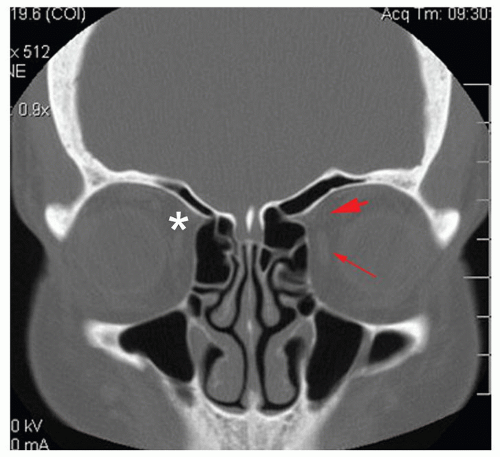 Figure 44.1 A coronal CT of the paranasal sinuses featuring the location of the anterior ethmoidal artery (asterisk) near the convergence of the medial rectus (arrow) and superior oblique (arrowhead) muscles. Note that in this patient, the anterior ethmoidal artery (asterisk) is located within a bony mesentery, suspended from the skull base. |
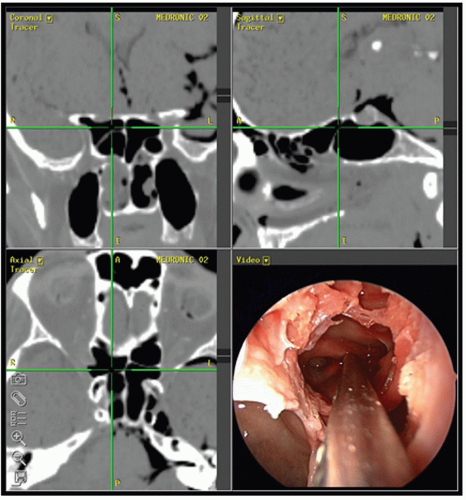 Figure 44.2 Triplanar images of an endoscopic dissection performed on a cadaver. The probe is pointing to the location of the opticocarotid recess where the carotid artery and the optic nerve are prominent within an Onodi (sphenoethmoid) cell. |
Two excellent articles relating to anatomic variations on CT scanning important to the sinus surgeon describe and enhance this anatomic discussion and are highly recommended (8,9). As the skull base transitions posteriorly to meet the planum sphenoidale, the ethmoid roof can be identified at the same level as the cribriform plate.
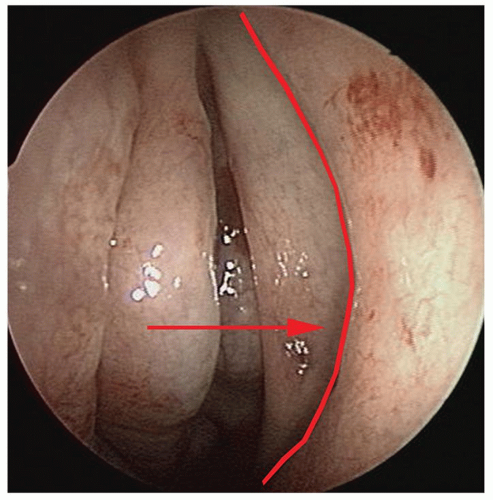 Figure 44.3 An endoscopic view of the middle meatus. The middle turbinate is medialized. A curvilinear line can be imagined at the junction of the uncinate process and the lacrimal bone. The maxillary sinus ostium (arrow) is located (in two-thirds of cases) at the junction of the inferior one-third and the superior two-thirds of this line. |
TABLE 44.1 SUMMARY OF IMPORTANT ANATOMIC RELATIONS | |
|---|---|
|
three-dimensional variance. The cribriform plate represents the lowest midline structure in the medial aspect of the nasal vault. The lateral mass of the ethmoid is suspended from the fovea ethmoidalis or ethmoid roof. Intervening between the ethmoid roof and cribriform plate is the lateral cribriform lamella, or simply lateral lamella. The length of the lateral lamella (and hence the depth of the cribriform plate) was noted by Keros (7) in several anatomic dissections. Keros classified the anterior skull base depth based upon the length of the lateral lamella: 1 to 3 mm (type I), 4 to 7 mm (type II), and 8 to 16 mm (type III). The skull base may also be asymmetric in design (Fig. 44.5). Some (10) have shown that type II anatomy is encountered most frequently and that patients with a lower skull base depth (i.e., type I) have a lower incidence of skull base injury.
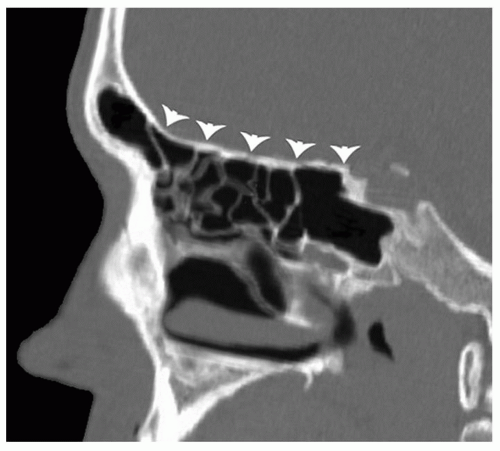 Figure 44.4 A sagittal reconstruction of the paranasal sinuses and anterior skull base. Note that the skull base (arrowheads) slopes in a downward fashion starting at the frontal recess and terminates at the planum sphenoidale (sphenoid roof). It is important to note this when operating within the posterior ethmoid sinuses. |
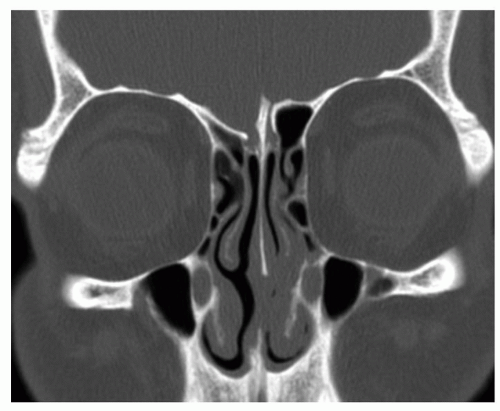 Figure 44.5 A coronal CT of the paranasal sinuses and anterior skull base. Keros categorized three types of skull base anatomy based on the length of the lateral lamella. However, the length of the lateral lamella may be different on each side. Therefore, the surgeon should always note any asymmetry in the skull base anatomy. |
proceeding through the basal lamella if the patient has a 2:1 or greater than 2:1 ratio. Therefore, the surgeon must consider this “angle of attack” when penetrating the basal lamella and entering the posterior ethmoid cavity. Entering the posterior ethmoids via the medial-inferior aspect of the coronal face of the basal lamella, along the roof of the maxillary sinus or floor of the ethmoid bulla, will provide a much safer avenue toward the sphenoid sinus and away from the skull base (Fig. 44.8).
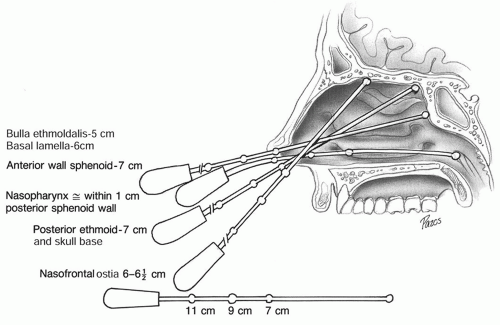 Figure 44.6 Beaded probe measurements to various areas of the nose from the nasal opening (nasal spine). (From Stankiewicz J. Complication of endoscopic sinus surgery. Otolaryngol Clin North Am 1989;22:749, with permission.) |
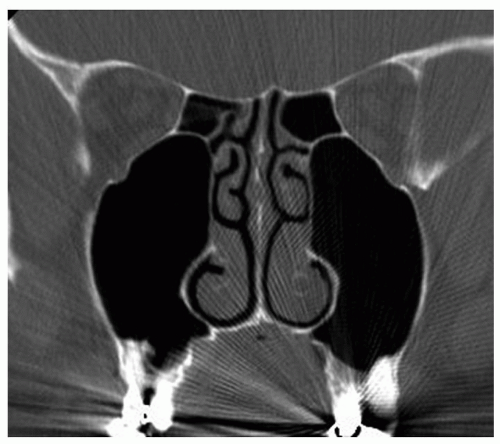 Figure 44.7 A coronal CT of the paranasal sinuses reveals significant asymmetry of the height of the maxillary sinus when compared to the height of the posterior ethmoid sinuses. A ratio (maxillary sinus height:ethmoid sinus height) ≥2:1, such as in this patient, places the posterior ethmoid skull base at high risk for injury when proceeding through the basal lamella. |
ethmoidectomy as “one of the easiest operations with which to kill a patient.” Most of the catastrophic complications are related to ethmoidectomy and frontal sinus surgery. Table 44.2 lists the complications of sinus surgery. May et al. (12) studied the complications of sinus surgery among large populations of patients noting CSF leak and blindness were the common major complications; orbital hematoma the most common minor complication.
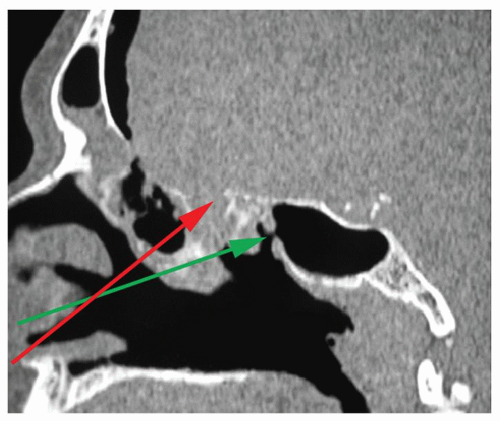 Figure 44.8 A sagittal reconstruction of the paranasal sinuses. This patient sustained an injury to the skull base that resulted in CSF rhinorrhea and pneumocephalus. This injury was due to high penetration of the basal lamella (red arrow). An angle of attack that penetrates the basal lamella at the roof of the maxillary sinus or base of the ethmoid bulla (green arrow) is safer when entering the posterior ethmoid sinuses. |
TABLE 44.2 COMPLICATIONS SINUS SURGERY | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
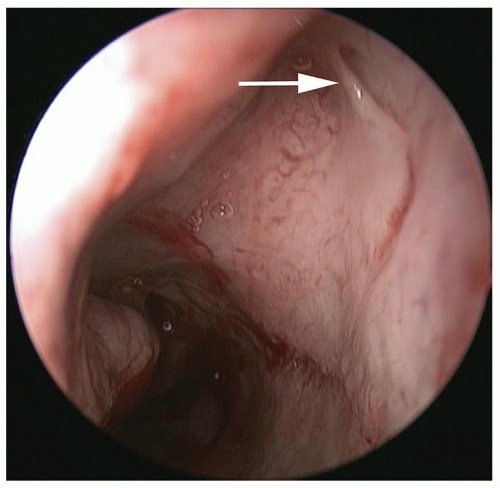 Figure 44.9 An endoscopic view of the inferior meatus. Hasner valve (arrow) is the termination of the lacrimal apparatus. Injury to Hasner valve can occur when performing an IMA as well as other procedures (turbinate fracture, turbinate resection, and endoscopic medial maxillectomy). |
respectively (13) and resolve within 1 to 2 weeks of the procedure. DeFreitas and Lucente (13) reviewed 670 Caldwell-Luc procedures and found a 9.1% and 3% incidence of facial paresthesias and dacryocystitis, respectively. Yarington (14) reported on 271 Caldwell-Luc procedures with a 3% overall complication rate. The most common complications were postoperative hypesthesia, devitalized teeth, and postoperative ethmoiditis. Blindness can occur with the Caldwell-Luc procedure if the orbit is entered, but this is a rare complication. DeFreitas and Lucente (13) also noted a recurrence of sinusitis and polyps in 12% and 5% of patients as well.
loss (average 384 mL) and an average hospitalization of 3.6 days. A total of 20.4% of patients had complications.
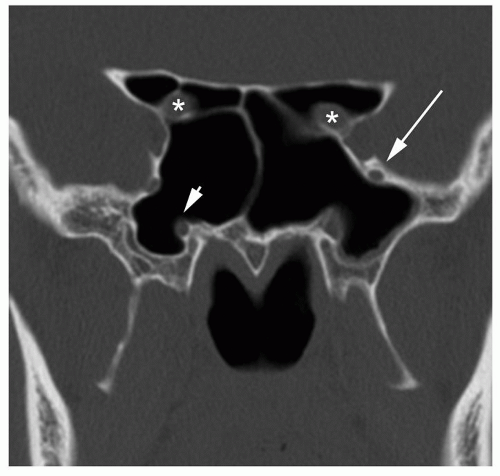 Figure 44.10 A coronal CT of the paranasal sinuses featuring the anatomy that relates to the sphenoid sinus. The optic nerve (asterisk), Vidian nerve (arrowhead), and maxillary nerve (arrow) can be easily seen in this image. Not as easily seen are the carotid arteries and the cavernous sinuses, which contain branches of the trigeminal nerve, the occulomotor nerve, the trochlear nerve, and the abducens nerve. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


