bites), or a foreign body (6,7). In contrast to other orbital complications, medical comorbidities such as cystic fibrosis, HIV, leukemia, diabetes, and other immune deficiencies are risk factors for preseptal cellulitis (7). Preseptal cellulitis manifests as eyelid swelling, erythema, and tenderness. Occasionally these may progress to an eyelid abscess (Fig. 38.2) and can also be associated with edema of the orbital (postseptal) contents. There are no limitations of extraocular movements and no impairment of visual acuity. Sinonasal infections cause periorbital swelling due to impaired venous drainage of the ethmoidal vessels that are obstructed by inflammation and pressure.
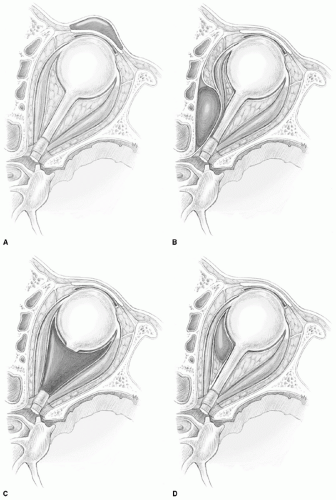 Figure 38.1 Chandler classification of orbital complications of sinusitis. A: Preseptal cellulitis (eyelid edema), (B) Subperiosteal abscess, (C) Orbital cellulitis, (D) Orbital abscess, |
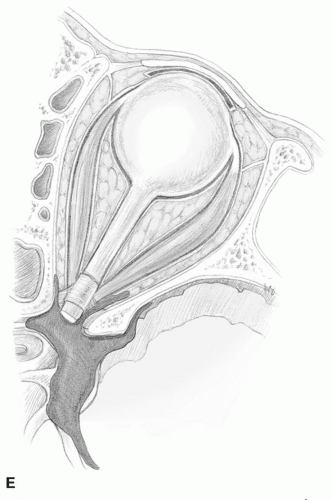 Figure 38.1 (Continued) (E) Cavernous sinus thrombosis. |
TABLE 38.1 ORBITAL COMPLICATIONS OF SINUSITIS | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
indicating optic neuritis and/or ischemia can occur as the disease progresses; these are prognostically worrisome findings. Not all cases of orbital cellulitis are due to sinusitis, however. Patients presenting with pain and diplopia and a history of recent orbital trauma or dental surgery should be assessed for orbital cellulitis. In diabetic patients with ketoacidosis and immunocompromised patients, more severe infections such as invasive fungal sinusitis should be considered. Orbital cellulitis is more concerning than preseptal cellulitis because it can evolve into an orbital abscess.
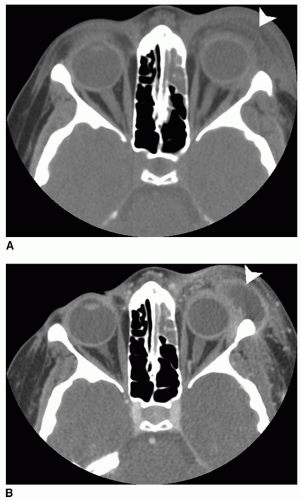 Figure 38.2 Preseptal abscess secondary to preseptal cellulitis. A: Axial CT scan taken on admission showing the patient with left ethmoid sinusitis and left preseptal cellulitis (arrow); patient also had frontal sinusitis (not pictured). B: Axial CT scan after 4 days of IV antibiotic treatment showing progression of infection to left preseptal abscess (arrow). The patient also developed an orbital subperiosteal abscess, scalp abscess, and small epidural abscess. |
 Figure 38.3 Axial CT scan demonstrating a left subperiosteal orbital abscess. The abscess is immediately adjacent to the lamina papyracea (the arrow is inside the abscess and identifies the lateral edge of the abscess); note the proptosis and the displacement of the orbital periosteum and medial rectus muscle. |
in the orbit results in orbital pain, chemosis, proptosis, and ophthalmoplegia. Cranial nerves III, IV, V1, V2, V3, and VI traverse the sinus and can all be affected. Extension of the phlebitis posteriorly into the cavernous sinus results in progression of symptoms in the opposite eye. This contralateral involvement is a distinguishing feature of cavernous sinus thrombosis. It can be associated with sepsis and meningismus or frank meningitis may be present.
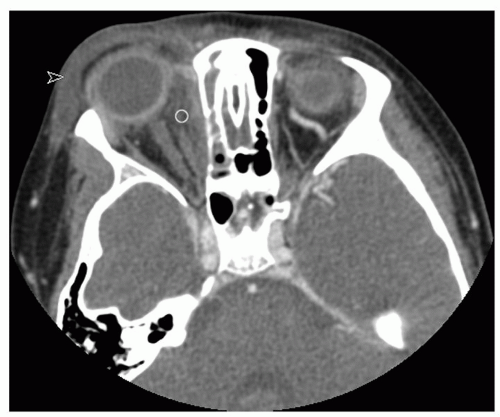 Figure 38.4 Axial CT scan showing right orbital cellulitis with diffuse orbital inflammatory changes that are intra- and extraconal (open circle); there is concurrent preseptal edema and inflammatory changes (arrow). |
series (5,6,7,22) (Table 38.2). Less common but consistent causes of complicated sinusitis are S. pneumoniae, other Streptococci, and anaerobic microorganisms. H. influenza, Eikenella, and other gram-negative bacilli are also implicated in some cases of complicated sinusitis.
TABLE 38.2 MICROBIOLOGY OF SINUSITIS AND RELATED COMPLICATIONS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|



