Complex Upper Airway Problems
Jay B. Tuchman
Deepak K. Mehta
The proper approach to any problem involves a well-constructed systematic plan, combined with diligent preparation and careful attention to detail, to successfully achieve the desired outcome. The principles of this methodology should certainly be adhered to when confronted with the complexities of airway management, and particularly when presented with the scenario of the difficult airway. The practitioner’s margin of error dwindles in patients with deteriorating clinical status and those at extremes of age or with a predisposition toward oxygen desaturation. An organized and focused preoperative airway evaluation, resulting in the advanced recognition of an impending difficult airway, can help avoid a catastrophic situation. Assessment should include a determination regarding possible difficulties with ventilation, intubation, patient cooperation, and/or tracheostomy (1). Failure to intubate a trachea will not result in a patient’s death, but inadequate preparation, allowing the consequences of “can’t intubate” to proceed along the slippery slope toward “can’t ventilate” may very well do so. Routine preparation and planning includes the availability of multiple sizes of basic equipment, optimal positioning for successful ventilation and intubation, and supplemental oxygenation (especially prior preoxygenation) throughout the airway management. The benefits of the proliferation of airway devices over the past few years should surely not be underestimated, but it is critical to realize that the choice of a particular advanced airway device does not constitute an adequate plan, and is undoubtedly not a panacea for avoiding the frightening “can’t intubate, can’t ventilate” clinical scenario. The development of the difficult airway algorithm of the American Society of Anesthesiology (ASA) is an embodiment of this multidimensional approach to management of the difficult airway (2). Basic management decisions include (a) awake intubation versus attempts after induction of general anesthesia, (b) noninvasive versus invasive initial approaches to intubation, and (c) preservation or ablation of spontaneous ventilation (1).
The algorithm includes a section for the awake approach to intubation, as well as an approach to situations involving failed intubation attempts after the induction of general anesthesia (Fig. 63.1). At all times, communication between services, involving a discussion of the multifaceted nature of the plan, as well as highlighting the particular involvement of each member of the operating room staff is of paramount importance in thwarting the development of this precarious scenario.
There are a multitude of pathologic characteristics associated with difficult airway management, including congenital features such as micrognathia, mandibular hypoplasia, macroglossia, cervical instability, limited mouth opening, midface hypoplasia, and facial distortion, as well as acquired conditions associated with infection, obesity, tumors, trauma, burns, and arthritis (3). The technique chosen must be tailored to the distinct disease presentation associated with the difficult airway. However, even within each situation, there may be multiple reasonable approaches, and it behooves the practitioner to be flexible and capable of changing course with alacrity, should the primary attempts prove unsuccessful. Utilizing the ASA difficult airway algorithm as a guide, we attempt to elucidate in this chapter the benefits of specific approaches, techniques and devices for particular airway scenarios, while simultaneously emphasizing the importance of a comprehensive plan for the management of each patient.
A decision to follow the pathway of awake airway management prior to anesthetic induction includes both the possibility of securing the airway via surgical access, or via noninvasive approaches such as flexible fiberoptic intubation, utilizing sedation, and topicalization of the airway (4).
In a patient with upper airway obstruction and acute respiratory distress, an urgent tracheostomy utilizing minimal sedation and maintaining spontaneous ventilation, with
infiltration of local anesthetic, might be appropriate. Other situations mandating an awake tracheostomy include patients unable to tolerate general anesthesia, or patients with supraglottic abscesses or masses, which may lead to aspiration of purulent material or airway distortion complicating endotracheal intubation. There are scenarios, however, where surgical access via tracheostomy may not be feasible, such as patients undergoing neck surgery, those with hematomas or abscesses of the neck, obese patients, and those with prior radiation or tumors (mnemonic SHORT) (5). It is always instructive to recognize that in the rare situation where airway manipulation may be so disastrous and lead to complete decompensation, the option of femoral-femoral cannulation under local anesthesia as preparation for possible cardiopulmonary bypass should be considered (6).
infiltration of local anesthetic, might be appropriate. Other situations mandating an awake tracheostomy include patients unable to tolerate general anesthesia, or patients with supraglottic abscesses or masses, which may lead to aspiration of purulent material or airway distortion complicating endotracheal intubation. There are scenarios, however, where surgical access via tracheostomy may not be feasible, such as patients undergoing neck surgery, those with hematomas or abscesses of the neck, obese patients, and those with prior radiation or tumors (mnemonic SHORT) (5). It is always instructive to recognize that in the rare situation where airway manipulation may be so disastrous and lead to complete decompensation, the option of femoral-femoral cannulation under local anesthesia as preparation for possible cardiopulmonary bypass should be considered (6).
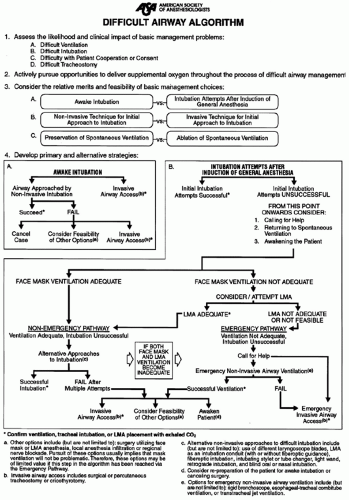 Figure 63.1 ASA difficult airway algorithm. Reproduced from American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003;98(5):1269-1277, with permission. |
The noninvasive approach of awake or sedated flexible fiberoptic intubation may be facilitated by the administration of small titrated doses of benzodiazepines, narcotics, ketamine, an antisialogogue such as glycopyrrolate, and a new agent, dexmedetomidine, resulting in a patient with reduced anxiety, decreased secretions, yet without respiratory depression. The antisialogogue also improves the effectiveness of topical anesthetics, by removing the barriers to mucosal contact. When combined with local anesthetic administered via injected nerve block techniques such as the Glossopharyngeal Nerve (GPN), Superior Laryngeal Nerve (SLN), and Recurrent Laryngeal Nerve (RLN) blocks, this may help achieve anesthesia of the nasopharynx, oropharynx, and hypopharynx in an awake, sedated patient. This allows for uncompromised airway exchange and oxygenation via spontaneous ventilation, maintenance of normal muscle tone with increased size and patency of the oropharynx, and improved upper and lower esophageal sphincter tone with intact protective airway reflexes, reducing the risk of severe gastroesophageal reflux and aspiration (3). The concern for pulmonary aspiration is a strong argument for the awake approach to intubation in patients with a difficult airway and full stomach, or those with obesity (7). However, limitations to the awake approach to intubation include young children, those with an allergy to local anesthetics, or others with an inability to cooperate due to mental retardation or dementia. Caution must also be exercised in situations where the possible negative consequences of awake attempts may be manifest, such as cardiac ischemia, increased intracranial or intraocular pressure, or neurologic damage from cervical spine instability (3).
A specific scenario of preemptive airway control unique to the fetal/neonatal population is the Ex Utero Intrapartum Treatment (EXIT) procedure (Fig. 63.2). Infants with a very low probability of survival, as suggested by prenatal ultrasound, due to tracheal obstruction or other airway abnormalities such as cystic hygroma, cervical teratoma, congenital goiter, or congenital high airway obstruction syndrome, are managed by maintaining uteroplacental circulation with only partial delivery. This allows time, prior to clamping of the umbilical cord, for procedures such as direct laryngoscopy, bronchoscopy, intubation, and tracheostomy to secure the airway and maintain continuous oxygenation, improving the chances of neonatal survival (8).
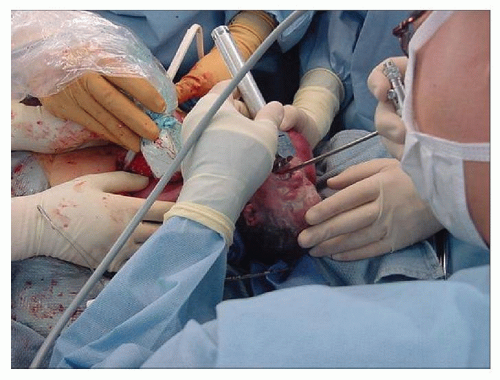 Figure 63.2 Bronchoscopy performed during EXIT procedure to secure fetal airway prior to delivery. |
When the decision has been made to attempt intubation after the induction of general anesthesia, and despite an appropriate plan, the initial approach has been unsuccessful, it is prudent to repeatedly consider calling for help, returning to spontaneous ventilation if not present, and possibly even awakening the patient. The advantages of assisted spontaneous ventilation include the maintenance of oropharyngeal muscle tone, avoiding total airway obstruction, and serving as a guide to locate the glottis. If face mask ventilation is still adequate despite unsuccessful intubation, alternative approaches to intubation should be considered (1).
If further attempts are made with a standard laryngoscope, optimum external laryngeal manipulation or backward, upward, rightward pressure on the thyroid cartilage may improve the grade of laryngoscopic view. Placing a flexible stylet inside the endotracheal tube (ETT) in a hockey-stick shape may facilitate ETT placement, even when only the epiglottis or arytenoid cartilages are seen. Particularly in children with micrognathia or macroglossia, where routine rigid laryngoscopy has been previously unsuccessful, the retromolar approach to direct laryngoscopy may be useful. The head is turned slightly to the left, and a straight Miller 1 blade (even in older children) is introduced while the right corner of the mouth is retracted (Fig. 63.3). Sweeping the tongue to the left, the laryngoscope is advanced between the tongue and lateral pharyngeal wall, overlying the molars, until the epiglottis is visualized (Fig. 63.4). The movement of the head and lateral placement of the blade allows for bypassing the tongue, a reduced need for soft tissue displacement, and improved line of site visualization (9).
Flexible fiberoptic bronchoscopy remains the gold standard for management of the difficult airway. Advantages of flexible fiberoptic bronchoscopy include those related to the
device and to the technique itself. The flexible bronchoscope allows flexibility and adaptability to varying airway anatomy with minimal manipulation, is applicable to both oral and nasal approaches in all age groups, and gives the practitioner the ability to provide both oxygen and topical anesthesia during intubation (10). The specific technique as described below decreases the trauma and cardiovascular response to airway instrumentation, has a consistently high success rate, and allows for confirmation of position. Improved digital technology obtains clearer images, even in the neonatal population, with the smallest scope sized 2.2 mm, and able to fit through a 2.5 ETT (9). Light sources and video systems have been incorporated into the newer bronchoscopes, allowing for increased portability, as well as the ability to display a larger image of the airway. The improved technology still comes at a high cost, with frequent maintenance necessary due to the fragility of the flexible scopes. There is a significant learning curve with the fiberoptic scope and maintenance of one’s skills requires continuous utilization (11).
device and to the technique itself. The flexible bronchoscope allows flexibility and adaptability to varying airway anatomy with minimal manipulation, is applicable to both oral and nasal approaches in all age groups, and gives the practitioner the ability to provide both oxygen and topical anesthesia during intubation (10). The specific technique as described below decreases the trauma and cardiovascular response to airway instrumentation, has a consistently high success rate, and allows for confirmation of position. Improved digital technology obtains clearer images, even in the neonatal population, with the smallest scope sized 2.2 mm, and able to fit through a 2.5 ETT (9). Light sources and video systems have been incorporated into the newer bronchoscopes, allowing for increased portability, as well as the ability to display a larger image of the airway. The improved technology still comes at a high cost, with frequent maintenance necessary due to the fragility of the flexible scopes. There is a significant learning curve with the fiberoptic scope and maintenance of one’s skills requires continuous utilization (11).
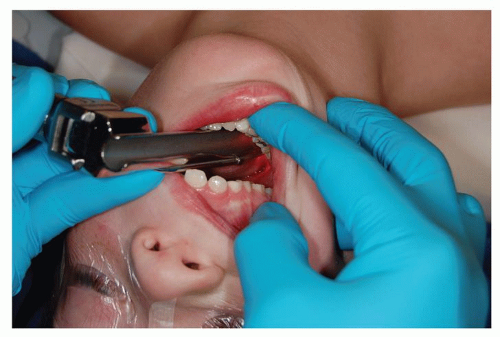 Figure 63.3 Placement of laryngoscope blade for retromolar technique. Courtesy of Larry Borland, MD. |
Optimal positioning for fiberoptic bronchoscopy requires the patient’s head to be slightly extended at the atlanto-occipital joint, while a jaw thrust, and at times tongue traction, is performed by an assistant, opening the posterior pharynx for an ideal view of the laryngeal opening. The flexible bronchoscope must be kept rigid, placing the tip of the scope in the midline. Specially designed oral airways may help facilitate midline placement during oral fiberoptic intubation, whereas nasal fiberoptic bronchoscopy will intrinsically allow for easier midline placement (10). The approach of choice for the pediatric patient is generally the nasal fiberoptic; however, due to the distinct possibility of adenoid shearing or epistaxis, premedication with topical vasoconstrictors is ordinarily undertaken. Nasal fiberoptic intubation can be greatly assisted by the modified nasal trumpet (Fig. 63.5), allowing spontaneous ventilation and the administration of volatile anesthetic, while fiberoptic intubation ensues via the other nares (Fig. 63.6). The modified nasal trumpet technique has
great utility in the pediatric population, or those with an inability to cooperate and tolerate an awake approach to intubation (9). Despite successful placement of the fiberoptic scope into the trachea, the practitioner may experience resistance to the ETT upon attempted advancement into the trachea. A helpful hint to avoid catching the ETT on the arytenoid cartilages is to place the ETT bevel down on the fiberoptic scope for oral intubations and bevel up for nasal intubations (mnemonic UNDO) (12). The major drawback of the fiberoptic scope is that excessive secretions or bleeding may render the scope completely unusable, particularly with the neonatal scope, which lacks a channel for suctioning or administering local anesthetic (10). This weakness argues strongly in favor of mandating the clinician to master a number of other techniques, as part of the comprehensive approach to airway management we have described above.
great utility in the pediatric population, or those with an inability to cooperate and tolerate an awake approach to intubation (9). Despite successful placement of the fiberoptic scope into the trachea, the practitioner may experience resistance to the ETT upon attempted advancement into the trachea. A helpful hint to avoid catching the ETT on the arytenoid cartilages is to place the ETT bevel down on the fiberoptic scope for oral intubations and bevel up for nasal intubations (mnemonic UNDO) (12). The major drawback of the fiberoptic scope is that excessive secretions or bleeding may render the scope completely unusable, particularly with the neonatal scope, which lacks a channel for suctioning or administering local anesthetic (10). This weakness argues strongly in favor of mandating the clinician to master a number of other techniques, as part of the comprehensive approach to airway management we have described above.
 Figure 63.4 Improved laryngoscopic view obtained with retromolar technique. Courtesy of Larry Borland, MD. |
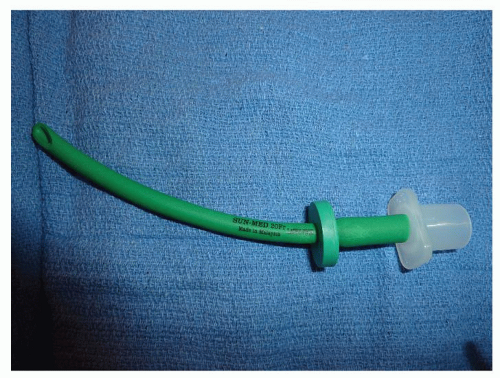 Figure 63.5 Modified nasal trumpet to help facilitate spontaneous ventilation while maintaining anesthetic depth for flexible fiberoptic laryngoscopy. |
 Figure 63.6 Flexible fiberoptic laryngoscopy facilitated by modified nasal trumpet. |
Aside from the standards of direct laryngoscopy and flexible fiberoptic laryngoscopy, this chapter focuses on six other main categories of devices that may be utilized, avoiding the need to resort to a surgical airway such as a cricothyroidotomy or tracheostomy. These include indirect laryngoscopes, rigid fiberoptic stylets, intubating or lighted stylets, video laryngoscopy, laryngeal mask airway (LMA)-guided intubation, and rigid fiberoptic bronchoscopy.
The first indirect rigid fiberoptic-enhanced laryngoscope (Fig. 63.7), the Bullard (Gyrus ACMI, Norwalk, OH), was originally designed for use in the difficult pediatric airway and is available in both adult and pediatric sizes. Although still quite expensive, this instrument, as well as other similar models such as the WuScope (Pentax, Orangeburg, NY) and Upsherscope (Mercury Medical, Clearwater, FL) cost less than the flexible scope, and are less prone to damage (13




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
