Purpose
To compare nylon monofilament suture with polytetrafluoroethylene sheet for frontalis suspension surgery to treat eyes with congenital ptosis.
Design
Retrospective, nonrandomized, comparative, interventional case series.
Methods
We reviewed the medical records of 49 patients who had undergone 79 eyelid frontalis suspension surgeries to treat congenital ptosis. All of the patients were younger than 16 years and had congenital ptosis with poor levator muscle function. They were treated with frontalis suspension surgery with either a nylon suture or a polytetrafluoroethylene sheet and were followed up for at least 1 year. A single rhomboid loop sling was used for the nylon suture surgery. For the polytetrafluoroethylene sheet, an incision was made in the eyelid crease, and one end of the sheet was fixed to the tarsus and the other was fixed to the frontalis muscle. The main outcome measures were postoperative recurrences and complications.
Results
We evaluated 37 eyelids of 25 patients after nylon suture surgery and 42 eyelids of 31 patients after polytetrafluoroethylene sheet surgery. Among these, 9 eyelids of 7 patients were included in both groups. The median postoperative follow-up period was 32 months in both groups. The recurrence rates were 62.2% for the nylon suture group and 0% for the polytetrafluoroethylene sheet group ( P < .001). The postoperative complication rates were 0% for the nylon suture group and 7.1% for the polytetrafluoroethylene sheet group ( P > .05).
Conclusions
Frontalis suspension using a polytetrafluoroethylene sheet with direct tarsus and frontalis muscle fixation is a reasonable technique with low rates of recurrences and complications.
Eyelid frontalis suspension surgery is a common operative procedure used to correct severe blepharoptosis in eyes with poor levator muscle function. Poor function is generally defined as an eyelid elevation of 4 mm or less. The main indication for frontalis suspension surgery is severe blepharoptosis secondary to myogenic, neurogenic, mechanical, and traumatic disorders. At present, congenital severe ptosis is repaired by frontalis suspension surgery, which consists of connecting the tarsal plate to the eyebrow with various types of sling materials.
Different methods are used to pass the sling material from the eyelid to the eyebrow area in the suborbicularis plane during frontalis suspension surgery. In addition, different types of loop designs, such as a single triangle, a single rhomboid, a single pentagon (Fox procedure), a double pentagon (Crawford procedure), and an open loop have been used. Autogenous fascia lata is generally considered to be the most effective sling material, with lower recurrences and lower rates of complications, for example, infections and granuloma formation. However, this technique requires the harvesting of the fascia lata, which carries the risk of postoperative donor-site complications such as local hypertrophy and scarring. Young children 3 years of age or younger are generally considered too young to undergo the surgery for the collection of a sufficiently long fascia lata, and ophthalmic surgeons are generally reluctant to perform this type of surgery because of the difficulty of harvesting the fascia lata. Preserved fascia lata is an alternative material for a frontalis sling. The main advantage of using preserved fascia lata is that an additional harvesting procedure is not necessary. It is particularly valuable for patients 3 years of age or younger. However, the recurrence rate is generally higher than that associated with autogenous fascia lata, with a long-term recurrence rate of approximate 50%.
Synthetic materials, such as monofilament and polyfilament nylon, monofilament polypropylene, silicone, and polytetrafluoroethylene (PTFE; Gore-tex; W.L. Gore & Associates Inc, Newark, Delaware, USA) have been used as alternative materials for frontalis suspension surgery. Frontalis suspension surgery with nylon suture or silicone rod has a relative high rate of recurrence of the ptosis, and it is generally considered to be a temporary treatment. However, the procedure has been used in young children with severe ptosis, and we have used nylon suture in young children to prevent occlusion amblyopia.
The recurrence rate after polytetrafluoroethylene use is relatively low and comparable with that after fascia lata surgery. However, soft tissue complications, such as infectious granuloma caused by the polytetrafluoroethylene strip or suture, have been reported. We have used polytetrafluoroethylene in the form of a sheet as an alternative method because of its stability and safety.
Although there have been many reports on the effect of frontalis suspension with synthetic materials, most reports tend to have a small number of cases and short follow-up periods. In addition, these studies used either sutures or strips of the materials with different looped designs for the surgeries. Because of these variations, it remains difficult to determine which type of synthetic material and which loop design is best for frontalis suspension surgery.
Thus, the purpose of this study was to determine the long-term results and incidence of complications of frontalis suspension surgery for the treatment of congenital ptosis. We compared the results using a nylon monofilament suture with those using a polytetrafluoroethylene sheet as the suspension materials.
Methods
This was a retrospective, nonrandomized, comparative, interventional case series study. Approval of this study was obtained from the Institutional Review Board of Seirei Hamamatsu General Hospital. The study was conducted in accordance to the tenets of Declaration of Helsinki. Informed consent for the surgery was obtained from the parents of the patients after a complete explanation of the procedures and possible complications.
We reviewed the medical records of all patients who had congenital ptosis with poor levator muscle function. All of the patients were treated with frontalis suspension surgery with either a nylon suture or a polytetrafluoroethylene sheet and were followed up for at least 1 year after the surgery. All operations were performed by the attending surgeons, and the surgeries were performed between April 2004 and March 2011 in the Department of Ocular Plastic and Orbital Surgery, Seirei Hamamatsu General Hospital, Hamamatsu-shi, Japan.
This study included only cases of simple congenital ptosis or blepharophimosis. Because acquired aponeurotic ptosis could develop in older adult patients with congenital ptosis with aging, we limited the patients to those younger than 16 years. The indications for surgery were congenital ptosis severe enough for the eyelids to cover the visual axis and block the view of the corneal light reflex when the eyes were in the primary position. These factors also were used to define whether a recurrence of the ptosis had occurred.
We divided the complications into 2 groups: postoperative recurrence of ptosis and occurrence of other complications including infection, granuloma formation, exposure, overcorrection, and undercorrection. To try to determine the cause of a recurrence when the nylon suture was used, we reviewed the movies of the reoperation to examine the condition of the nylon suture in the eyelids.
Surgical Techniques
Surgery was performed under general anesthesia, and the eyelid and eyebrow were anesthetized with 0.5% lidocaine with 1:100 000 epinephrine. Topical antibiotics were used during surgery, and antibiotic eye ointment was used after surgery.
For the nylon suture surgery, a single rhomboid loop was used for the sling ( Figure 1 ). First, 2 points approximately 10 mm apart were marked on the upper eyelid corresponding to the medial and lateral limbus of the cornea. The marks were approximately 3 to 4 mm higher than the lash line. Two other points were marked above the eyebrow in line with the 2 points marked on the eyelid. Then, 4 incisions 1 to 2 mm long were made through the skin and orbicularis muscle with a no. 11 scalpel at the marked points. One of the incisions above the eyebrow was enlarged slightly so that the knot of the suture could be buried in it at the end of surgery. A 4-0 or 5-0 nylon monofilament suture was passed through the tarsal tissue from one puncture incision in the eyelid to the other with an 18-mm round needle (a half-circle). A corneoscleral protector was placed under the eyelid during these procedures. The eyelid was everted to ensure that the needle did not penetrate through the eyelid. Then, the suture was passed from one eyelid incision site to the corresponding eyebrow exit site deep through suborbicularis tissue or under the orbital septum with a 37-mm cutting needle (a three-eighths circle). The suture was passed horizontally from one eyebrow puncture point to the other with an 18-mm round needle (a half-circle). The 2 ends of the suture were tightened and adjusted to achieve the desired eyelid elevation and contour. Then, the ends were tied and the knot was buried subcutaneously.

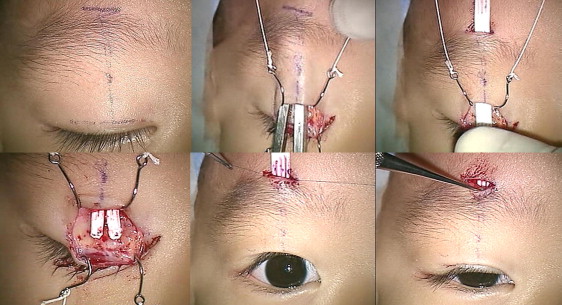
For the polytetrafluoroethylene sheet surgery, a 0.3-mm thick polytetrafluoroethylene sheet was cut to a rectangular piece 50 mm long and 5 mm wide. The polytetrafluoroethylene surgical method was based on the technique used for direct tarsal and frontalis muscle fixation ( Figure 2 ). Three lines were marked on the upper eyelid and eyebrow: a horizontal eyelid incision line to create a palpebral crease, a central vertical line just above the pupil to the eyebrow, and a small horizontal incision line above the eyebrow. A wide eyelid crease incision was made with a no. 15 scalpel to expose the tarsal plate and the orbital septum. A tunnel was made deep to the orbital septum from the eyelid incision to above the eyebrow along the marked central line. A small incision was made above the eyebrow to the tunnel. The polytetrafluoroethylene sheet was passed through the tunnel. The lower part of the polytetrafluoroethylene sheet was divided into 2 branches to form an inverted Y. The 2 limbs of the Y were fixed with 6-0 suture to the upper tarsus. The upper limb was pulled up and adjusted to ensure that the eyelid had a natural contour. To achieve satisfactory lid contour, the 2 branches of the sheet were moved medially or laterally before securing the sheet to the tarsus. The pretarsal tissue was repaired and the lower polytetrafluoroethylene sheet was covered. The eyelid crease was created by internal fixation to prevent eyelash ptosis. The eyelid crease incision was closed with 7-0 suture. The upper limb of the polytetrafluoroethylene sheet was adjusted for the desired eyelid elevation. The upper polytetrafluoroethylene end was fixed with 5-0 suture to the frontalis muscle and the subcutaneous tissue under the eyebrow. Excess polytetrafluoroethylene material of the upper limb was trimmed off and buried in the tunnel. The small incision above the eyebrow was closed with 7-0 suture.
Statistical Analyses
The significance of the differences in the age at the time of surgery and the postoperative follow-up period between the nylon suture group and the polytetrafluoroethylene sheet group was determined by Mann–Whitney U tests. Comparisons of the frequency of ptosis recurrences and complications between the 2 groups were made by Fisher exact probability tests. Kaplan-Meier analysis was used to calculate the cumulative occurrence of events defined as recurrences or complications. The difference in the event-free survival between the 2 groups was analyzed by log-rank test. A P value less than .05 was accepted as being statistically significant. The statistical analyses were performed using JMP software version 8.0.1 (SAS Institute Inc, Cary, North Carolina, USA).
Results
Sixty-six patients with congenital ptosis underwent frontalis suspension surgery using either a nylon suture or a polytetrafluoroethylene sheet between April 2004 and March 2011. Among these, 9 patients were excluded because the follow-up period was less than 1 year, and 8 patients were excluded because they were older than 16 years. In the end, 70 eyelids of 49 patients with congenital ptosis who had undergone frontalis suspension surgery and were followed up for at least 1 year were studied. There were 29 boys and 20 girls and 21 bilateral and 28 unilateral cases. Simple congenital ptosis was the initial diagnosis in 44 patients, and blepharophimosis syndrome was the initial diagnosis in 5 patients.
We analyzed 37 eyelids of 25 patients who had undergone nylon suture primary or secondary surgeries and 42 eyelids of 31 patients who had undergone polytetrafluoroethylene sheet primary or secondary surgeries ( Table 1 ). Among these, 9 eyelids of 7 patients were included in both groups, that is, they underwent nylon suture surgery first and were followed up more than 1 year and then demonstrated a recurrence of the ptosis and underwent secondary surgery with a polytetrafluoroethylene sheet and were followed up for more than 1 year ( Figure 3 ).
| Nylon Suture | Polytetrafluoroethylene Sheet | P Value | |
|---|---|---|---|
| No. of patients (eyelids) | 25 (37) | 31 (42) | |
| Mean age ± SD (median), y | 4.2 ± 4.9 (2) | 5.8 ± 3.3 (5) | <.001 |
| Mean postoperative follow-up ± SD (median), mos | 38.3 ± 21.5 (32) | 33.2 ± 17.7 (32) | NS |
| Bilateral or unilateral surgery, no. of patients | |||
| Bilateral | 12 | 11 | |
| Unilateral | 13 | 20 | |
| Previous treatments, no. of eyelids | |||
| Levator resection | 1 | 6 | |
| Frontalis suspension using a nylon suture | 0 | 9 | |
| Ptosis recurrence, no. of eyelids (%) | 23 (62.2) | 0 (0) | <.001 |
| Complications, no. of eyelids (%) | 0 (0) | 3 (7.1) | NS |
In the nylon suture group, 12 patients underwent bilateral surgery and 13 patients underwent unilateral surgery. In the polytetrafluoroethylene sheet group, 11 patients underwent bilateral surgery and 20 patients underwent unilateral surgery. In the nylon suture group, 1 eyelid had undergone a previous levator resection surgery for ptosis. In the polytetrafluoroethylene sheet group, 15 eyelids had undergone previous ptosis surgery, including 6 eyelids with levator resection and 9 eyelids with frontalis suspension using a nylon suture.
The mean age at the time of surgery was 4.2 ± 4.9 years (median, 2 years), with a range of 6 months to 15 years, in the nylon suture group, and 5.8 ± 3.3 years (median, 5 years), with a range of 3 to 14 years, in the polytetrafluoroethylene sheet group. The nylon suture group was significantly younger than the polytetrafluoroethylene sheet group ( P < .001, Mann–Whitney U test).
The mean postoperative follow-up period was 38.3 ± 21.5 months (median, 32 months), with a range of 12 to 76 months, in the nylon suture group and 33.2 ± 17.7 months (median, 32 months), with a range of 13 to 70 months, in the polytetrafluoroethylene sheet group. The difference in the postoperative follow-up period between the 2 groups was not significant.
A recurrence of the ptosis was found in 23 of 37 (62.2%) eyelids in the nylon suture group, which was significantly more frequent than the 0 of 42 (0%) eyelids in the polytetrafluoroethylene sheet group ( P < .001, Fisher exact probability test). The recurrences in the nylon suture group appeared after a mean of 25.7 ± 9.6 months (median, 24 months), with a range 10 to 50 months. Other than the recurrences in the 14 eyelids, there were no other postoperative complications in the nylon suture group.
In the polytetrafluoroethylene group, there were no recurrences; however, complications developed after the surgery in 3 eyelids (7.1%; P = .15, Fisher exact probability tests). Infections and granuloma developed in 2 eyelids (4.8%) in the polytetrafluoroethylene sheet group. The 2 infections occurred within 3 months after the surgery and required reoperations ( Figure 4 ). One case of infection was resolved by incision and drainage. The other case required removal of the polytetrafluoroethylene sheet, which was removed easily. Even after removal of the polytetrafluoroethylene sheet, the upper eyelid height was maintained.
An undercorrection of the ptosis was found in 1 eyelid (2.4%) in the polytetrafluoroethylene group, and this eyelid required a reoperation 1 year after the primary surgery to adjust the polytetrafluoroethylene sheet. This child had bilateral ptosis and a downward slant of the palpebral fissures associated with partial trisomy 22. He had undergone bilateral suspension surgery using polytetrafluoroethylene sheets. In this case, the ptosis of the left eyelid was not corrected sufficiently during the first postoperative week, and it was not classified as a recurrence. The reoperation to adjust the amount of elevation to the eyebrow incision at a later stage was relatively easy.
Both groups had cases in which the surgery was a secondary ptosis surgery, that is, 1 eyelid (previous surgery: levator resection) in the nylon suture group and 15 eyelids (previous surgery: levator resection in 6 eyelids and frontalis suspension using a nylon suture in 9 eyelids) in the polytetrafluoroethylene sheet group ( Table 1 ). We then compared only primary surgery cases, excluding secondary surgery cases in both groups. A recurrence of the ptosis after the primary ptosis surgery was found in 22 (61.1%) of 36 eyelids in the nylon suture group and in 0 (0%) of 27 eyelids in the polytetrafluoroethylene sheet group ( P < .001). Other postoperative complications were found in none of the eyelids in the nylon suture group and in 2 (7.4%) of 27 eyelids in the polytetrafluoroethylene sheet group ( P = .18).
An event for the survival graph was defined as a recurrence of the ptosis or the development of other complications ( Figure 5 ). Although an event-free survival rate at 36 months after the surgery in the nylon suture group decreased to approximately 30%, the success rate with the polytetrafluoroethylene sheet was maintained at approximately 90% throughout the experimental period. The difference in the survival rate between the 2 groups was significant ( P < .001, log-rank test).



