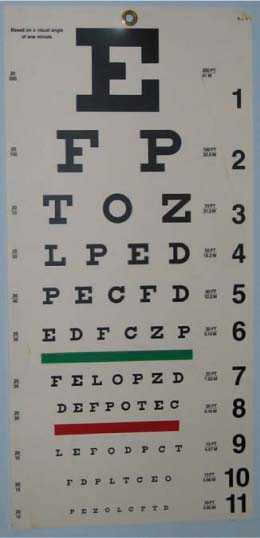
Chapter 1 Clinical testing of visual function measures visual acuity, color vision, and visual fields. Testing of the pupillary response to direct light stimulation may also be considered an indicator of visual function but is not a pure test of visual function. Testing of these parameters of visual function involves a variety of subjective and objective techniques. Selecting which tests to use for which patient and for which clinical problem is part of the art of assessing visual function and neuro-ophthalmology. Visual acuity is the optical resolving power of the eye or simply how well patients can see using their central visual field. Measuring visual acuity must be tailored to the patient’s age, cooperation, medical and neurologic condition, and literacy. Visual acuity is tested for distance and near vision with the patient wearing glasses or contact lenses. Each eye is tested independently. The right eye is tested first and then the left. As a routine, we do not check visual acuity with both eyes open unless the patient has nystagmus. We use a Snellen chart (Fig. 1–1) to check distance visual acuity. The chart should be 20 feet from the patient and well illuminated. The patient should be comfortably seated and at the same level as the chart. We try to eliminate glare from the windows and doors because these lighting conditions can affect vision. In our offices, we use a mirror-projection system so that not as large an area is required. Observe how the patient reads the chart. The manner in which the patient reads the chart may provide some clues to the diagnosis. For example, while the right eye is being tested, if the patient ignores the letters on the right side of the chart of each line he may have a right homonymous hemianopia or bitemporal hemianopia. The smallest line that a patient reads is the visual acuity. Normal vision is 20/20. If the patient reads less than 20/20, visual acuity is checked using a pinhole over the patient’s glasses. The pinhole should be no more than 2.4 mm in diameter. If the visual acuity improves to the 20/25 range, the decrease is caused by a refractive error, probably in the range of 3 to 4 diopters. If the visual acuity does not improve or improves only slightly, then it is likely to be due to a large refractive error or to some other pathology. If the visual acuity worsens with the pinhole, then it is likely due to retinal disease. If the patient reads 20/25 with the pinhole, the vision is recorded as 20/25 PH. If the patient does not read the 20/400 line, we ask the patient to move closer to the chart. If the patient reads the 20/400 line at 6 feet, the visual acuity is recorded as 6/400. The numerator is the distance in feet between the patient and the chart, and the denominator the line that is read. If the patient does not read any line standing close to the chart, the patient’s visual acuity may be poor. We now ask the patient to count our fingers by showing one, two, or five fingers close to his face. If he is able to count fingers correctly, we then move away from the patient until he cannot see to count the fingers. The visual acuity is recorded as CF @ the distance seen. Suspect nonphysiologic visual loss if the patient vision does not improve on moving close to the chart. FIGURE 1–1 Snellen acuity chart, used in measuring visual acuity. These charts vary in design, but all include letters, numbers, or symbols of decreasing size, corresponding to better visual acuity. If the patient cannot count fingers close to the face, we move a hand in front of the eye to be tested. If the patient sees the hand moving, we record as hand motion (HM). This test should be performed in all four quadrants of the visual field: superotemporal, superonasal, inferotemporal, inferonasal. If the patient cannot see hand motions, we then check the ability to see light [light perception (LP)]. This test is done in a darkened room. The eye that is not tested is covered with the palm of the patient so that light does not reach this eye, preventing a false response from the opposite eye. A bright light source such as the indirect ophthalmoscope or the muscle light should be used. The source of light should be documented in the chart. Shine the light and ask the patient if it is dark or bright rather than “Do you see the light?” Depending on the patient’s response, you can record visual acuity as NLP (no light perception) or LP. If LP, you can refine this by shining the light from the four quadrants as described before for HM. (See Table 1–1 for a list of common abbreviations used in vision records.) Here are some examples of Red Flags:
CLINICAL TESTING OF VISUAL FUNCTION
VISUAL ACUITY
ADULTS
Distance Visual Acuity
Red Flags
 “I do not see any letter” Make sure that the letters are projected on the mirrors.
“I do not see any letter” Make sure that the letters are projected on the mirrors.
 “I can see better without glasses” This may be due to a change in the refractive error, or the patient may be wearing nearvision glasses or someone else’s glasses.
“I can see better without glasses” This may be due to a change in the refractive error, or the patient may be wearing nearvision glasses or someone else’s glasses.
 “I can see the letters but they are blurry” This could be due to scratches or dirty lenses or to ocular causes.
“I can see the letters but they are blurry” This could be due to scratches or dirty lenses or to ocular causes.
 In the presence of a droopy lid, visual acuity may be improved by manually elevating the lid.
In the presence of a droopy lid, visual acuity may be improved by manually elevating the lid.
 Patient reads better when single letters are shown This may be normal in some children; suspect amblyopia or lazy eye.
Patient reads better when single letters are shown This may be normal in some children; suspect amblyopia or lazy eye.
 Vision improves after a few blinks This most probably is due to an ocular surface problem such as dry eyes or an improper contact lens fit.
Vision improves after a few blinks This most probably is due to an ocular surface problem such as dry eyes or an improper contact lens fit.
 Patient feels that the letters are distorted in one eye Suspect unilateral ocular causes.
Patient feels that the letters are distorted in one eye Suspect unilateral ocular causes.
 Patient feels that the letters are distorted in both eyes Suspect bilateral ocular causes or occipital cause.
Patient feels that the letters are distorted in both eyes Suspect bilateral ocular causes or occipital cause.
 If the patient’s vision does not improve with pinhole or by moving closer to the chart, suspect nonphysiologic visual loss.
If the patient’s vision does not improve with pinhole or by moving closer to the chart, suspect nonphysiologic visual loss.
 If the patient denies LP Suspect nonphysiologic visual loss in the presence of a brisk pupillary light reflex.
If the patient denies LP Suspect nonphysiologic visual loss in the presence of a brisk pupillary light reflex.
OD | Right eye |
OS | Left eye |
OU | Both eyes |
BCVA | Best corrected visual acuity |
SC | Without correction |
CC | With correction |
PH | Improvement with pinhole |
W | With glasses |
NPH | No improvement with pinhole |
HM | Hand motion |
CF | Counting fingers |
LP | Light perception |
NLP | No light perception |
20/20−2 | Missed two letters in the 20/20 line |
20/20+2 | Read two more letters in the next line |
CSM | Central, steady, and maintained |
FF | Fixes and follows |
 If the patient sees the letters double (monocular diplopia) with the other eye covered, it is most likely due to an ocular cause. This suspicion can be confirmed by an improvement with pinhole. In the absence of an ocular cause, suspect cerebral polyopia/diplopia due to parietal or parieto-occipital stroke (see Chapter 9).
If the patient sees the letters double (monocular diplopia) with the other eye covered, it is most likely due to an ocular cause. This suspicion can be confirmed by an improvement with pinhole. In the absence of an ocular cause, suspect cerebral polyopia/diplopia due to parietal or parieto-occipital stroke (see Chapter 9).
 Letters appear smaller in one eye Likely to be refractive error or ocular cause, especially macular edema.
Letters appear smaller in one eye Likely to be refractive error or ocular cause, especially macular edema.
 Letters appear dimmer in one eye This is likely to be an optic neuropathy or chiasmal disorder.
Letters appear dimmer in one eye This is likely to be an optic neuropathy or chiasmal disorder.
 “Vision is better if I manipulate my glasses” This is due to a refractive error.
“Vision is better if I manipulate my glasses” This is due to a refractive error.
 Patient does not read the letters in right or left half of each line Suspect visual field defect.
Patient does not read the letters in right or left half of each line Suspect visual field defect.
 Letters come and go This could be due to fluctuation in refraction, ocular surface disease, cataract, or paracentral scotomas directly adjacent to fixation.
Letters come and go This could be due to fluctuation in refraction, ocular surface disease, cataract, or paracentral scotomas directly adjacent to fixation.
 Patient misses some letters on a line, or reads an “E” as “F” This could be due to small central scotomas or astigmatism.
Patient misses some letters on a line, or reads an “E” as “F” This could be due to small central scotomas or astigmatism.
 If the patient cannot read the letters but can write them: “alexia without agraphia.” This syndrome is caused by disconnection of the right occipital cortex due to a lesion of the corpus callosum and left calcarine cortex, as well as associated areas of higher cortical function (see Chapter 29).
If the patient cannot read the letters but can write them: “alexia without agraphia.” This syndrome is caused by disconnection of the right occipital cortex due to a lesion of the corpus callosum and left calcarine cortex, as well as associated areas of higher cortical function (see Chapter 29).
Near Visual Acuity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


