Careful evaluation of the lens is an essential part of a complete eye examination. Cataracts (Figs. 1, 2, 3, 4), in particular age-related or senile cataracts, are among the most common ocular finding in older patients and accounts for up to 50% of blindness worldwide.1,2,3 In the United States, among Medicare beneficiaries, cataract is the most common condition for which eye care services are sought, accounting for 45% of visits to eye doctors.4 In addition, cataract surgery is the most frequently performed surgical procedure among 30 million Medicare beneficiaries.4 With the prolongation of human life by advances in medicine, increasing numbers of patients with age-related disorders, especially cataracts, are to be expected.
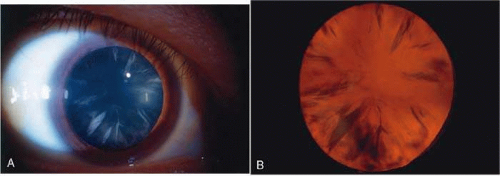 Fig. 1. Cortical cataract using (A) direct illumination (B) retroillumination. Cortical cataracts usually start in the lens periphery and encroach into the visual axis (and interfere with central vision) only in later stages. |
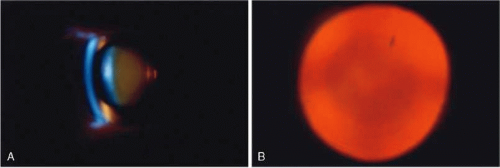 Fig. 2. Brunescent (brown) nuclear cataract using (A) narrow beam slit illumination and (B) retroillumination. The cataract is best seen by direct slit illumination. In retroillumination, as seen in this image, the outline of the nuclear cataract may be seen due to its increased refractive index, although the cataract does not cast any shadows. Because of its central location, this cataract may cause distortion of images early in their development. |
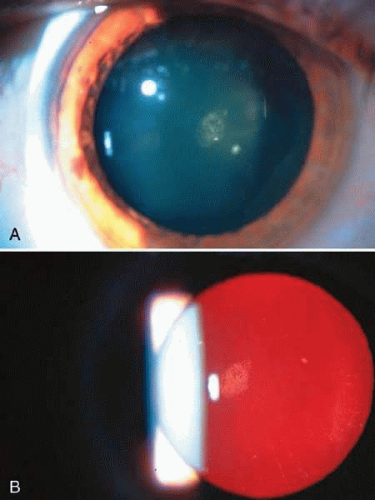 Fig. 3. Posterior subcapsular cataract (PSC) using (A) direct illumination and (B) retroillumination. PSCs usually start centrally and extend toward the periphery. For this reason, they interfere with visual function, causing glare disability early. |
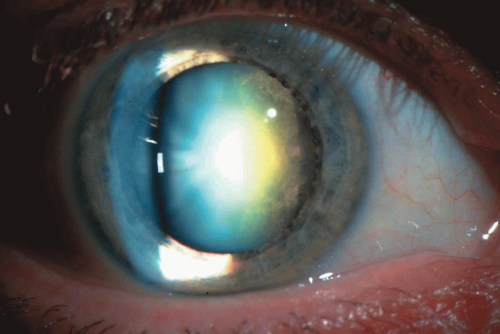 Fig. 4. Mixed cortical-nuclear-posterior subcapsular cataract. |
The primary purpose in managing a patient with cataract, as stated in the American Academy of Ophthalmology’s, Preferred Practice Pattern for Cataract in the Adult Eye,5 is to improve functional vision and the quality of life. Currently, the only effective treatment of cataract is surgical removal with, in most cases, insertion of an intraocular lens. The indications for surgery are: when the cataract-impaired vision no longer meets the patient’s needs, and the anticipated benefits of surgery outweigh the risks. No single test adequately describes the effect of cataract on a patient’s visual status or functional ability.5 It is important then, that each clinician be well versed in the current techniques of cataract assessment (such as cataract detection, documentation, and monitoring methods), and the assessment of the total effect of the cataract on the patient’s daily needs and quality of life (such as visual function and functional impairment tests).
Noncataractous lens changes occur with normal aging6,7 and the clinical difference between early cataract and age-related change is often not clear-cut. The difference becomes more obvious as the cataract progresses, hence the need for regular follow-up examinations in the elderly. Most clinicians tend to vary in their subjective grading of cataractous changes. For this purpose, newly developed clinical cataract grading systems (see below) using standard cataract photographs help clinicians to document the progress of cataracts better and to compare their assessment with that of other clinicians. These grading systems are especially useful in clinical research studies as well as for publication of clinical reports.
Once a cataract is diagnosed, the clinician should determine its overall effect on visual function and the well-being of the patient. These assessments will serve as the basis for a decision whether to recommend any treatment such as cataract surgery. A careful inquiry should be made into the patient’s daily, occupational, leisure, and social activities and document any cataract-related impairment. The recent introduction of functional disability measures, such as the NEI VFQ-25 and VFQ-14 tests (see below), allow more objective and accurate measures of the functional disability caused by a cataract on a particular patient.
This chapter aims to summarize currently available methods for the evaluation of cataracts for clinicians and to describe new promising methods being developed and tested. Tremendous technological advances in the field of computers, photography, and imaging in the last 10 years have revolutionized ophthalmology, especially in the diagnosis and treatment of eye disorders including cataracts. Developments in recent years have helped standardize various methods used for the documentation and monitoring of cataracts as well as the documenting the effect of cataracts on a patient’s visual function and quality of life. Table 1 gives a list of these methods, which are then discussed in detail in the text.
Table 1. Methods used in Cataract Evaluation: Documentation of Cataract and Its Effects on Vision | |
|---|---|
|
METHODS USED FOR CATARACT EVALUATION: DOCUMENTATION OF CATARACT AND ITS EFFECT ON VISION
VISUAL ACUITY TESTING
Snellen Charts and Projectors
Since its introduction in 1862, the Snellen test chart has been the clinically preferred standard used to measure visual acuity, and thus also used initially to assess the effect of cataracts on visual function. It remains the gold standard used to measure minimum separable and legible acuity,8 to measure the effect of any abnormal state of the eye, as well as for measurement of the effectiveness of medical and surgical intervention in diseased states of the eye.
Recently, the need to be able to obtain measurements of visual acuity values that can be used for statistical analysis for research studies has led to further standardization and modifications of the Snellen chart. One such modification for such purposes is the Early Treatment Diabetic Retinopathy Study or ETDRS version.9 It was designed to have a geometric progression of the letter size of test letters and standardized lighting of the chart. Visual acuity scores are expressed as the logarithm of the minimal angle of resolution (LogMar), which is linear, meaning, it decreases by 0.1 unit for each lower line on the chart. Most current clinical eye research studies use the ETDRS visual acuity chart measurements as a major end point.
As recently as four decades ago, as a result of high complication rates, cataract surgery was deferred until a patient did not have much to lose in terms of visual acuity, should intraoperative or postoperative surgical complications occur. Patients were advised to wait until their cataract was “ripe” and their Snellen visual acuity dropped down to 20/80 or worse before contemplating surgery. With the development of safer techniques such as the intracapsular cataract extraction (ICCE) technique using the Cryoprobe, and later the extracapsular cataract extraction (ECCE) technique using automated irrigation-aspiration (I/A) devices and implantation of an intraocular lens (IOL), the indication for cataract surgery was lowered to a Snellen acuity of 20/40 or worse coupled with anticipated improvement of vision. In most states, a minimum requirement for an unrestricted license to drive a vehicle was a visual acuity of 20/40 and a patient could potentially lose his/her driver’s license should his/her Snellen acuity drop below this level. Hence, the cataract needed to be removed to allow the patient to continue driving.
Currently, with the development of even safer techniques such as phacoemulsification followed by implantation of an IOL (resulting in lower complication rates and superb postoperative vision), the indications for surgery have further changed. The American Academy of Ophthalmology (AAO)’s Preferred Practice Pattern for Cataract in the Adult Eye states that there is no single test that adequately describes the effect of cataract on visual status and functional ability. Cataract/IOL surgery is therefore indicated when the vision no longer meets the requirements of the patient, and when the expected surgical benefits outweigh the risks. Hence, not only the level of visual acuity but other considerations such as the ability to perform daily tasks of living, ability to perform work or avocations, and good quality of life in general are equally important in deciding when cataract extraction should be performed.
Snellen-type visual acuity tests measure the eye’s ability to resolve fine detail at high contrast but do not adequately describe the ability to see large but low contrast patterns such as faces or nearby objects. A cataract may affect the results of the Snellen acuity test minimally, and yet a patient may already experience difficulties in daily activities such as driving or walking especially in bright sunlight or at night, or have difficulty in their line of work, such as lawyers or accountants who need to read fine print accurately or architects who need to see fine lines in a line drawing.
Recently, a number of tests have been proposed to document changes in visual function that are not detected by the Snellen visual acuity test. Among the important ones are contrast sensitivity testing and glare testing.10 A number of glare and contrast sensitivity tests have been devised and continue to be further refined, especially with the use of computer monitors. Potential acuity tests such as the Guyton-Minkowsky Potential Acuity Meter (PAM) and clinical interferometers are used mainly to determine macular function independent of media opacities such as corneal, lens, and vitreous opacities. The Resolution Test Target Projection Ophthalmoscope was developed to document distortions in vision that are not adequately determined by the Snellen acuity test. The following are discussions of each of these.
Clinical Contrast Sensitivity Tests
Contrast sensitivity is a measure of the amount of contrast required to detect or recognize the target. Cataracts increase intraocular light scatter causing a reduction in retinal image contrast, and a subsequent decrease in contrast sensitivity. In general there are two types of devices used for contrast sensitivity testing.10 The traditional devices consist of sine wave gratings, which are patterns of alternating light and dark bars produced and controlled by computers, wherein the spatial frequency, contrast luminance, field size, and attenuation at the edge of the field are either modifiable or fixed.11 Examples of this are, among others, Optec 3500 Vision Tester (Stereo Optical Co., Inc., Chicago, IL), B-VAT PC system (Medtronic Solan Co., Inc., Jacksonville, FL), Smart System 20/20 (M & S Technologies, Inc., Chicago, IL), and CSV-1000E Contrast Sensitivity Instrument (VectorVision, Inc., Arcanum, OH). The second type of devices are based on photographically reproduced sine wave gratings (such as the Arden plates and the Vistech vision contrast test system) or variable contrast optic types (such as the Regan letter chart, the Vistest picture test, the Pelli-Robson letter chart, and the Melbourne edge test),12
Hess and Woo13 first reported contrast sensitivity function loss in patients with cataracts. They suggested that early cataracts cause high-spatial frequency loss, whereas more advanced cataracts produce both high- and low-spatial frequency losses. Drews-Bankiewicz et al.14 documented correlations between early nuclear cataracts with loss of contrast sensitivity in the intermediate and high spatial frequencies (4 to 16 cycles per degree). Lasa et al.15 found significant contrast sensitivity loss only in advanced cortical and posterior subcapsular cataracts. This loss was also correlated with decreased Snellen visual acuity. Adamsons et al.16 however, found that contrast sensitivity scores were lower for all patients with lens opacities than for clear lenses at high frequencies only, and all lens opacity groups scored similarly with each other. Recently, Kuroda et al.17 found a significant correlation between increasing lens density (using the Scheimpflug camera to measure lens density) and loss of contrast sensitivity in nuclear and cortical cataracts at 12 cycles per degree.
Glare Testing
Glare sensitivity refers to the change in visual function caused by the presence of a glare (light) source in another part of the visual field. In general, glare can be divided into either discomfort or disability glare. Discomfort glare causes a photophobic sensation without measurable effects on visual function, whereas disability glare causes reduction in visual function because of the presence of a bright light source.18 Disability glare is a specific type of glare caused by light scattered by the ocular media and is the type of glare that is commonly tested by the devices that have been developed to document glare.
Glare testing is helpful in documenting glare disability especially for those patients who complain of glare when driving at night and having difficulty with oncoming headlights, or having difficulty reading road signs when there is bright sunlight.19 Examples of these devices include the Brightness Acuity Tester or BAT (Marco Ophthalmics, Jacksonville, FL), the CSV 1000HGT (VectorVision Inc., Arcanum, OH), and the Optec 3500 Vision tester (Stereo Optical Co., Inc, Chicago, IL).
Potential Acuity Tests
Pinhole acuity8 is easy and quick to perform and is often used when visual acuity is less than 20/20. It can give useful information, especially if one obtains a good reading. However, a poor pinhole acuity result does not necessarily mean poor macular function because the decrease in retinal illumination produced by use of the small aperture degrades the image as it reaches the macula. Recently, Melki et al.20 studied a standardized method of pinhole testing and found it relatively reliable in estimating the visual outcome after uncomplicated cataract surgery without coexisting disease. Another version of the pinhole test described by Hofeldt and Weiss21 uses a specially illuminated near card (Mini-Illuminated Near Card, Gulden Ophthalmics, Elkins Park, PA). They found that it was useful in predicting postoperative acuity in cataractous eyes with comorbid disease.
Various tests of visual discrimination such as the ability to perceive light coming from various quadrants of the visual field (light projection), to perceive the orientation of the streak from a Maddox rod, and to discriminate between two light sources versus one source of light do not depend on macular function. Even color perception is not a valid measure of macular function, since cone receptors are present in the peripheral retina. The electroretinogram and visual evoked potential are not specific for macular function. These tests do not correlate well with visual acuity in the presence of amblyopia or macular degeneration.
The entoptic phenomenon test is traditionally used in mature cataracts to test for gross retinal function. This phenomenon is created by sweeping a small light source such as a hand-held light from side to side against the eye, usually shining the light through the lower or upper eyelid pointing toward the macular area. The strips of photoreceptors beneath the retinal blood vessels do not have time to adapt when the shadows of the blood vessels move rapidly from side to side, and the shadows become visible as a branching pattern embracing the macula. Perception of the vascular shadows described as seeing veins or vines is a time-honored test for visual function in mature cataracts, but it is not specific for macular function and therefore does not correlate well with postoperative visual acuity in the presence of localized macular disease.
Entoptic phenomena are poorly quantifiable and it is difficult to assign a numeric level of expected visual acuity based on the response of a patient. Using the bluefield entoptoscope, Sinclair and coworkers22 tested 136 eyes prior to uncomplicated cataract surgery. They obtained up to 94% correct prediction of good foveal function and at least 75% correct prediction of poor foveal function. However, Murphy,23 showed less success with bluefield entoptoscopy, especially in dense cataracts. False-positive predictions of potential acuity have also been reported in the presence of macular disorders.
In the presence of dense mature cataracts, if there is serious doubt as to the status of the retina or optic nerve, and thus the outcome of cataract surgery, it may be necessary to perform additional tests such as ultrasonography and computed tomography (CT) scanning.
The following two devices were designed as macular function test devices independent of media opacities in the cornea, aqueous, lens, or vitreous: the potential acuity meter and the clinical interferometer. In actual practice, however, both are effective only in mild to moderate cataracts where there is no macular dysfunction or disease state. However, they have proven to be very useful within these limits, esp. in predicting surgical outcomes in questionable cases, as discussed below.
The Guyton Minkowski PAM (Marco Ophthalmic, Jacksonville, FL)24 projects a standard Snellen chart through a 0.1-mm diameter aperture. This projected chart is directed through small windows in the cataract onto the macula and the patient reads the chart from 20/400 to 20/20. It uses a low-cost incandescent lamp and has a field of vision of 6 degrees.
In the clinical interferometer, beams of coherent light from two point sources are directed to the clearest area of the lens into the retina. Interference fringes in the macula are formed wherever the two beams overlap and by varying the width of the interference fringe pattern, visual acuity can be determined with the Snellen equivalent from 20/660 to 20/20, independent of the optics of the eye. Clinical interferometers use either red helium neon laser light or white light from an incandescent source such as a Xenon Halogen lamp, with a field size ranging from 1.5 degrees to 8 degrees. An example of this is the Heine Lambda 100 hand-held Retinometer (Lombart Co., Norfolk, VA).
In actual use, both the PAM and clinical interferometers underestimate as well as overestimate the potential vision in certain conditions.25 The PAM tends to underestimate the potential acuity in advanced, dense cataracts without any clear zones or openings through which to project the Snellen chart. This is not necessarily a disadvantage in such cases, because the actual postoperative acuity may be much better than predicted, to the pleasant surprise of both patient and surgeon.
On the other hand, clinical interferometers tend to overestimate potential vision in patients with macular disease, such as macular degeneration and amblyopia. In this device the retina has to distinguish the two overlapping coherent light beam fringes as two distinct lines. There may happen to be a few good cones that are situated at just the right position to distinguish these two lines as separate and give a good potential acuity reading. However, there may not be enough cones to recognize a Snellen letter of the equivalent level of acuity. This may result in an overestimation of the potential vision resulting in an unexpectedly poor postoperative vision.
Both the PAM and clinical interferometers are therefore useful to determine the potential acuity and possible outcome of surgery in patients with mild to moderate cataracts. However, they perform poorly in dense opacities, which they cannot penetrate, so that the patient cannot perceive the test objects. Caution should be used when interpreting results from patients with macular disease and amblyopia.26,27,28
Tests for Refractive Distortions in the Lens
RESOLUTION TEST TARGET PROJECTION OPHTHALMOSCOPE.
Localized refractive distortions may occur during the development of a cataract, which may distort vision to such an extent that the patient is incapacitated. This may be of major importance to patients with special visual needs, such as surgeons, accountants, bookkeepers, and architects. A device to document these distortions by projecting a series of parallel lines into the retina, which decrease in size to correspond to a Snellen equivalent numerical unit of measure, was developed by the U.S. Air Force29 and modified by Lobo and Weale.30 The Oqual (Zeiss Meditec, Dublin, CA) is mounted on an ophthalmoscope and the examiner views the projected lines in the fundus, grades the degradation of the projected chart image, and documents the degradation of the image using the Snellen equivalent unit.
FUNCTIONAL IMPAIRMENT/QUALITY-OF-LIFE TESTS
During careful history taking, the patient usually volunteers typical complaints associated with cataracts, such as painless, progressive loss of vision, difficulty seeing in bright sunlight or at dawn and dusk, increased glare from incoming headlights when driving at night, and difficulty reading road signs. As a result of the vast improvement of cataract and intraocular lens surgical techniques, with the resultant decrease in the complication rate of cataract surgery, criteria for cataract surgery have changed in recent years. These changes allow for earlier surgery if the cataract interferes with the patient’s occupation and other activities, combined with the determination (using the potential vision tests described above) that the patient would indeed benefit from cataract surgery. Hence, any visual difficulty with daily activities, as well as the patient’s occupational, leisure and social activities, should be inquired about and noted down. A brief statement should be entered into a patient’s chart to summarize these discussions, such as: “The patient’s visual function has decreased to a level that interferes with the patient’s ability to carry out normal daily activities. In addition, given the mental status and physical abilities of the patient, there is reason to expect some surgical benefit in function and personal comfort and/or activity.” This can be added to the consent form also, with the statement that possible complications with eye surgery were discussed with the patient. These discussions with the patient and their proper documentation in the chart play a crucial role in the decision making in cataract surgery as well as in litigation when there is a problem as to the outcome of cataract surgery.
Recent research has also revealed the interesting observation that in older patients, cataracts may play an important role in the causation of car accidents,31 falling accidents resulting in fractures,32 and mortality and functional decline.33 Hence, earlier visual rehabilitation through cataract/IOL surgery is becoming not only an option but a necessity.
Recently, more detailed and standardized methods of documenting these visual and functional disabilities have been developed, especially for clinical research purposes.
National Eye Institute Visual Function Questionnaire: 25 Items (VFQ-25)
The National Eye Institute Visual Function Questionnaire: 25 Items (VFQ-25) was developed under the sponsorship of the National Eye Institute with the goal of creating a survey that would measure the dimensions of self-reported, vision-targeted health status that are most important for persons with chronic eye problems.34 The survey measures the influence of visual disability and visual symptoms on patients’ daily visual functions as well as other health domains such as emotional well-being and social functioning. It consists of a base set of 25 vision-targeted questions representing 11 vision-related constructs, plus 1 general health rating question. It takes approximately 10 minutes for an interviewer to administer. There is also a self-administered format. The VFQ-25 forms (revised 2000), as well as additional information, can be obtained from the website of the National Eye Institute (http://www.nih.gov.easyaccess1.lib.cuhk.edu.hk).
Visual Function Questionnaire—14 Items (VF-14)
The Visual Function Questionnaire—14 Items (VF-14) was developed by a team from the Johns Hopkins University Hospital and Georgetown University Hospital as a measure of functional impairment caused by cataract and provides information not conveyed by visual acuity or a general measure of health status. It has also been shown to be sensitive and reproducible.35,36
OPHTHALMOLOGIC CLINICAL EXAMINATION
Hand-Held Light Examination
Field eye examinations, such as done in epidemiologic studies and surveys, can be facilitated by the use of a hand-held light in conjunction with a head-mounted or spectacle-mounted magnifying loupe, ideally inside a darkened room (to promote mydriasis). Because one is looking mainly for visually significant cataract, information obtained with this method, together with a Snellen visual acuity measurement, is the usual end point for these studies. More sophisticated equipment such as an ophthalmoscope and a hand-held slit lamp biomicroscope will be needed if a more precise classification and grading of the cataract is needed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


