6 Clinical Assessment of Voice Disorders The human voice gives us our identity and personality, and it changes throughout our lives from birth through to senescence. It is actually difficult to simply define a normal voice, but it is usually described as having the following characteristics: •It is audible, clear, or stable in a wide range of acoustic settings. •It is appropriate for the gender and age of the speaker. •It is capable of fulfilling its linguistic and paralinguistic functions. •It does not fatigue easily. •It is not associated with discomfort or pain on phonation. Voice quality is an extremely important element in how well a message is communicated with positive and negative effects. A “good” voice can captivate our attention or stir our emotions and is an essential attribute for a performance-level professional voice user such as an entertainer, an actor, a singer, or a broadcaster. However, a “bad” voice, which may sound strained, weak, rough, monotonous, or inappropriate in pitch, can cause the listener to become distracted and bored or lose concentration. Variations in voice quality can provide valuable cues about our current emotions, physical health, and psychological well-being. There is also a continuum between normal and disordered or pathological voice. Individuals, with what an objective listener would consider a pathological voice, may be quite comfortable with their voice quality considering it “their voice”—as long as it fulfills their functional needs. Indeed, abnormal speaking and singing voice qualities can sometimes help determine the personality and character of a professional voice. Patients seek help with their voice problem because they are suffering some form of disability that can take three main forms: (1) impairment, which is a structural problem with the vocal apparatus, for example, a laryngeal tumor causing an alteration in function such as hoarseness; (2) limitation in activity, for example, reduced vocal range in singing or voice tiring with use; and (3) participation restriction, for example, not being able to work or sing in a choir as a result of the voice problem (http://www.who.int/topics/disabilities/en/).1 The consequences of voice problems can be physical, functional, psychosocial, occupational, or financial. To understand the link between impairment, activity limitations, and participation restrictions, it is important to briefly review the normal mechanism of voice production and how this mechanism can be affected by pathological processes. Normal voice production (phonation) is discussed in detail in Chapter 4. Simplistically, voice production requires three processes: (1) an energy source—provided by the lungs; (2) a vibrating structure—usually the two vocal folds in normal voice production; and (3) a resonator—the vocal tract (Table 6.1). The vocal folds are adducted and the free edges of the mucosal surfaces start to vibrate causing compression followed by rarefaction of air molecules, which is the fundamental property of the generation of a periodic sound wave.2
Normal and Disordered Voice
Normal and Disordered Voice Production
Normal Voice Production
Which Essential Element of Voice Production Is Affected? | Which Pathological Processes Are Present? |
1.Energy source: provided by the lungs and causing the vocal folds to vibrate 2.Vibrating structure: the vocal folds—the sound source of the voice 3.Resonator: the vocal tract—modulating the acoustic properties of the sound source (vowels) and adding additional sounds (consonants) to produce recognizable speech and singing voice tones | 1.Structural/neoplastic abnormality •Malignant •Benign 2.Inflammation •Infective •Noninfective 3.Neuromuscular dysfunction •Hyperfunctional •Hypofunctional •Mixed hyper-/hypofunctional •Control/coordination issues 4.Muscle tension imbalance •Primary •Secondary |
The frequency of vibration of the vocal folds (fundamental frequency) is determined by their elastic properties and tensioning.2 The actual sound that a listener hears, however, is determined by the resonance properties of the vocal tract. The resonance properties and the consequent filtering effect can be modulated by the shaping and structure of the vocal tract. The sound emitted from the mouth therefore consists of the fundamental frequency and the nonfiltered multiples of the fundamental frequency (harmonics or overtones). This filtering effect results in concentrations of sound energy at specific frequency bands (formants) that we interpret as individual vowel sounds. Additional sound elements can be added by constricting parts of the vocal tract in production of consonants.3
Pathological Processes Causing Voice Problems
There are four main pathological processes that can contribute to the voice becoming disordered (Table 6.1). It is essential that the presence or absence of these four processes is checked for systematically, particularly as voice disorders tend to be multifactorial (Fig. 6.1). This also reduces the chances of overlooking pathologies, for example, a vocal fold paresis in cases of apparent muscle tension imbalance. Each pathological process can affect any part of the three essential elements of voice production, that is, breath control, vocal fold vibration, and resonance. This is determined by careful history and examination, occasional specialist assessments, and probe therapy or empirical treatment. However, by looking for evidence for each of the four etiologic factors individually, the clinician is able to target the treatment more precisely.
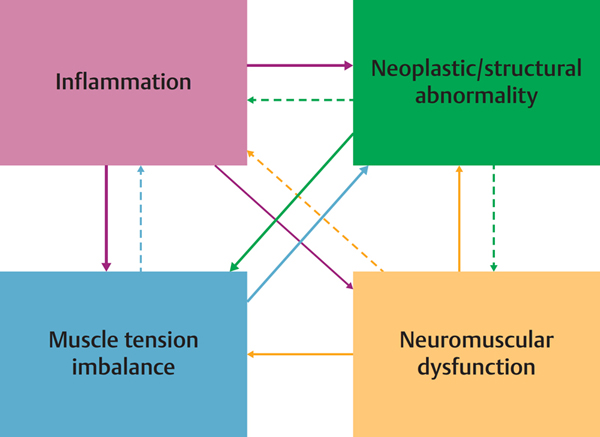
Figure 6.1 Pathological processes and their interactions. Voice disorders are often multifactorial in origin. More than one pathological process may be present or one can lead to another.
It is also important to try and ascertain which is the primary factor and which are secondary or compensatory factors affecting the voice quality. This is not always the same as the patient’s complaint!
Clinical Example of Interaction
A patient with long-standing Reinke edema (structural abnormality) may develop laryngopharyngeal reflux (inflammation), which stiffens the tissues making them more difficult to vibrate. This in turn may require increased muscular effort (muscle tension imbalance) and a more strained voice quality. This increased muscular effort may be compounded by the patient’s concern that he or she might have cancer from smoking. Treating the reflux and muscle tension elements may mean the Reinke edema does not require surgical treatment. In fact surgical treatment can be positively detrimental. In some cases, it can cause stiffened, scarred vocal folds (iatrogenic impairment), making voice production more difficult causing activity limitations and social participation restrictions.
Operating on the Reinke edema usually involves reducing the bulk of the vocal folds with the consequence of increasing the pitch of the voice. This can affect the patient’s self-identity particularly in women, leading to further psychological issues. This is in contrast to the patient with Reinke edema who dislikes the sound of and the negative comments about the voice because it is too deep and who has given up smoking. Surgery, after appropriate counseling, can then have significant positive effects on the quality of life.
Inadequate Energy Input (Breath Support)
To vibrate, healthy vocal folds need an adequate flow of air from the lungs and generation of subglottic pressure to overcome the inertia and viscoelasticity of the apposed vocal folds to induce oscillation. This minimum pressure to initiate phonation is known as the phonation threshold pressure. Values of phonation threshold pressure are in the order of 3 to 5 cm H2O but once oscillating the pressure can be reduced by 1 to 2 cm H2O.4 Structural or inflammatory changes in any part of the lower respiratory tract from alveoli to trachea or chest wall (polymyositis, poliomyelitis, severe chest wall, or diaphragmatic deficiencies) may potentially affect voice production secondary to hypoventilation. Similarly, weakness of the respiratory muscles may result from neuromuscular disorders such as Guillain-Barré syndrome, motor neuron disease, and myasthenia gravis.
Primary abnormal breathing patterns (muscle tension imbalance of respiratory muscles) are a common cause of voice disorders, resulting in inefficient speech-breathing patterns.5,6 By relying on the accessory respiratory muscles (high clavicular breathing pattern) rather than the diaphragm, patients may feel they are running out of air when they talk.7,8 In paradoxical vocal cord dysfunction, when there is adduction of the vocal cords during inspiration causing inspiratory stridor, there may be associated dysphonia.9
Dysfunction of Vibratory Apparatus
To vibrate efficiently and effectively, the vocal cords need to come together and oscillate in a controlled regular manner. A gap between the vocal folds causes breathiness, whereas irregular vibration or involvement of supraglottic structures causes roughness. Hoarseness is the perception of voice abnormality, which can be due to breathiness, roughness, or a combination of the two.
To vibrate effectively, the vocal cords need an adequate driving (subglottic) pressure. This is determined by the airflow and resistance (gap) at the glottis (Pressure = Flow × Resistance). If the gap is too large (low resistance), the flow is too high to maintain the pressure necessary to vibrate the vocal folds. Air escapes giving a breathy voice and the poor vocal fold vibration does not lead to the generation of good-quality sound waves. The patient may not be able to produce a loud voice or be heard above background noise, the patient’s voice may tire with use, or the patient may run out of air while talking and suffer throat dryness or paralaryngeal discomfort.
If the vocal folds are held too tightly together or there is an imbalance in tension or mass or if the layered structure of the vocal folds is abnormal, they will not be able to vibrate effectively, giving a hoarse, rough, or strained voice quality. They may also suffer with some of the above symptoms due to the increased effort in phonation and poor resonance.
In some cases of primary muscle tension dysphonia, there is excessive medial, anteroposterior, or concentric constriction at the glottic or supraglottic level (Table 6.2).5 The vocal folds may be partially or sometimes completely obscured by the false folds during attempted phonation. Several patterns associated with distinct voice profiles have been identified.10–14 The effect on the voice can vary in severity, be intermittent or constant, and be episodic. Muscle tension dysphonia (Type IIb) can also be secondary to a structural, neuromuscular, or inflammatory cause requiring increased laryngeal muscular effort to overcome the underlying defect (Table 6.2). Psychological issues can lead to either excessive vocal or false fold constriction (Type II) preventing air passing through the larynx or the vocal folds being excessively tensed and splinted apart but with little or no air flow (Type IV).
In neuromuscular cases, the degree of vocal fold contact during phonation can vary between being fully abducted, that is, in the “cadaveric” position (e.g. in brainstem injury) to reduced contact that may only be apparent with prolonged voice use (e.g. in myasthenia or a paresis). No contact or reduced contact affects the ability of the lungs to generate sufficient subglottal pressure to lead to sustained vocal fold vibration. The voice is whispery due to turbulent airflow through the glottis and from vocal tract constriction. In unilateral vocal fold palsies, the gap is variable and depends on many factors including the degree of compensation (Table 6.3). To achieve better closure, the larynx may become asymmetrical and the vocal folds may stretch, allowing better closure and loudness but at the expense of a rise in pitch. In unilateral superior laryngeal nerve palsy, the symptoms may be vague but there may be diplophonia and instability of the voice at higher pitches.15 Findings can be subtle but include asymmetry of the posterior glottis and petiole of the epiglottis at higher pitches.16
Although the vocal folds can vibrate irregularly in neuromuscular disorders and muscle tension dysphonia due to tensioning abnormalities, the effects on the voice are often overshadowed by other perceptual features such as breathiness and abnormalities in pitch or loudness. Roughness is more common when there is evidence of inflammation or structural abnormalities of the vocal folds. Inflammation can cause surface exudate (thickened mucus and/or ulceration) or inflammatory changes in the vocal fold mucosa. Structural lesions have variable effects depending on which layer or layers of the lamina propria or vocal fold are affected, the resultant effect on the remaining normal structures, and the compensatory response. For example, an early cancer extending from the epithelium to the deeper underlying muscle on one vocal fold inhibits the mucosal wave so that it cannot vibrate and produce a sound wave. The main effect on the voice is actually the aperiodic vibration of the opposite normal vocal fold caused by the mass effect of the cancer, which is perceived as roughness. This can be seen on stroboscopy or high-speed recordings. An increase in the mass of the vocal folds will lower the pitch of the voice: other mass effects may lead to supraglottic structures vibrating, adding an additional deep rough quality to the sound. If the mass lesion prevents complete glottal closure, air will escape through the glottis causing added breathiness to the voice quality. Analyzing what structures can and cannot vibrate the size of the glottal gap and what can be realistically restored to normal underpins the surgical treatment principles of phonosurgery.
In summary, if air is allowed to escape through the vocal folds from incomplete closure (glottal gap), then a breathy quality will be added to the voice. Abnormalities of the mass, the layered structure, in tensioning, or the elasticity of the vocal folds will cause them to vibrate in a disordered and irregular (aperiodic) manner. This will cause roughness, strain, or pitch abnormalities. Supraglottic structures such as the false folds, aryepiglottic folds, and arytenoid mucosa may also be induced to vibrate. This may be in addition to, or more rarely replace vibration of the vocal folds causing deepening of the pitch and roughness of the voice.
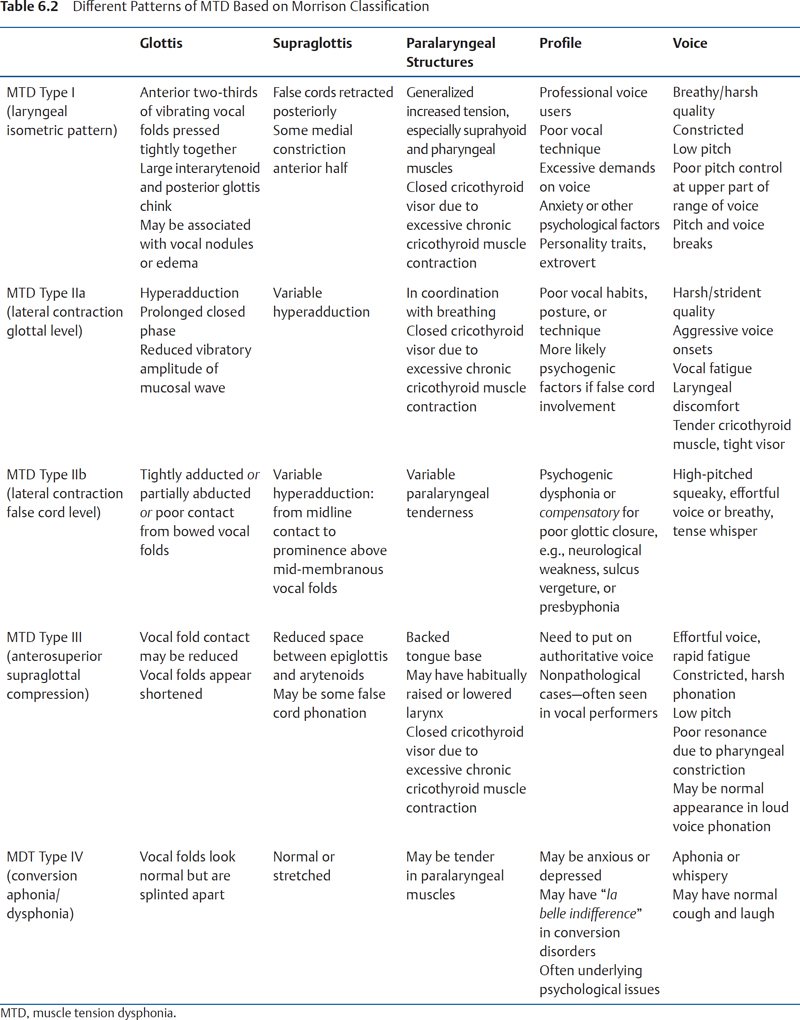
Table 6.3 Factors that Determine the Unpredictable Voice Outcome Following Damage to the Neural Supply to the Larynx
Factor | Comment |
Patient factors: •Individual patient neuroanatomy | •There is considerable variability in the degree of anastomoses between right and left, superior and recurrent, laryngeal nerves. •This complex arrangement helps explain some of the variability in presentation, compensation, reinnervation, and recovery from patient to patient. |
Injury factors: •Level of injury ○Recurrent laryngeal nerve (RLN) ○Superior laryngeal nerve (SLN) ○High vagal (RLN+SLN) •Degree of neural damage ○Complete transection or crush injury ○Partial transection or infiltration ○Segmental demyelination ○Tumor infiltration/scarring | •The degree and severity of the conduction block resulting from the injury also influence recovery. •The severity of the neural injury can vary from segmental demyelination (neuropraxia) to preservation of the neural conduits (axonotmesis) to complete severance (neurotmesis). •A full recovery is usual in neuropraxia as remyelination over the preserved axon restoring conduction and function. In neurotmesis, only a small proportion of fibers bridge the gap between proximal and distal ends being inversely proportional to the size of the gap. •To complicate matters further, the RLN carries mixed adductor and abductor fibers so reinnervation is a random process, which leads to synkinesis. •Other factors influencing recovery and the voice outcome include neurogenic muscle atrophy and vocal fold height disparity. |
Ineffectiveness of the Vocal Tract Resonator
If air is blown through an excised human larynx with the vocal folds adducted, the sound produced has a buzzing quality unlike any recognizable voice quality. This is similar to blowing through an oboe reed that is not attached to the bore of the instrument. The shaping of the vocal tract allows standing waves to develop in the air column. The sound produced by resonance of the air column consists of the fundamental frequency (determined by the frequency of vibration of the vocal folds) and certain harmonics (multiples of the fundamental frequency). Some of these harmonics are effectively filtered out by reducing their intensity, which has the effect of enhancing the energy in certain bands of frequencies (formants). Our brain recognizes these patterns of sound energy concentrated in specific frequency bands as a specific sound character, that is, a vowel. By changing the length and the shape of the resonating chamber (vocal tract), the energy and intensity of sound in specific frequency bands (formants) change. Our brain recognizes the new pattern as a different vowel. It is important to recognize that the fundamental frequency and the harmonics generated by the vibration of the vocal folds may not have changed, rather it is only the effect of the filter of the harmonics that has changed. Consonant sounds in contrast are produced by passing air through constrictions in the vocal tract and can be associated either with vocal fold vibration (voiced) or without (voiceless). For a more in-depth discussion, see Kent et al (1996).3
Individual variations of the vocal tract (supraglottis, piriform fossae, oropharynx, palate, oral cavity, postnasal space, and nasal cavity) are largely responsible for giving us our unique voices. However, structural abnormalities, neuromuscular deficits, inappropriate excessive constriction (muscle tension imbalance), and inflammation of any part of the vocal tract will affect the resonance characteristics of the air column and hence the voice quality. In extreme cases of structural abnormality such as a cleft lip and palate, the resonance patterns and vocal tract constrictions are less precise, making both the vowel and consonant components of the speech sound more difficult to interpret.17 Neuromuscular lesions such as a stroke have variable effects depending on the area and extent of the brain that is affected. The vocal tract can undergo structural changes (due to muscle atrophy or spasticity) and there can be a lack of control of the articulators causing dysarthria. The effect is imprecise consonants, distorted vowels, and hypernasality.18,19
Inflammation, for example, an upper aerodigestive tract infection, affects the resonance characteristics in two ways. The inflammatory process is likely to alter the elasticity of the mucous membranes and therefore the reflective properties of the lining of the vocal tract. Second, there may be changes due to certain resonance chambers, for example, the nasal passages and sinuses being narrowed or occluded. This may be in addition to any inflammatory effects on the vocal folds. The dominant effects on an individual’s voice will vary depending on their anatomy and the nature and severity of the disease process. The voice tonal quality may change and become, for example, “hyponasal,” with a reduction of higher frequency energy due to damping. This has been shown to affect speech intelligibility using automatic speech recognition software.20 Attempts to overcome this effect may result in additional laryngeal effort (increased glottal contact), sometimes risking damage to the vocal fold mucosa.
For the standing waves to be generated efficiently, the lower end of the air column (glottis) needs to be closed. In other words, if there is a glottal gap, energy can escape back into the lungs, which reduces the energy in the transmitted sound from the lips. Muscular constriction of the pharynx, incorrect laryngeal height, too much tightness in the jaw, and tongue narrowing the oral cavity all reduce the effectiveness of the resonating chamber in voice projection, which is often found in cases of muscle tension dysphonia.
Clinical Assessment
A key responsibility as a health professional is to provide an accurate diagnosis to avoid injudicious surgery or prolonged voice therapy that can have detrimental effects on the voice or, at the very least, be a waste of time and resources. Other patient relevant factors that should be taken into consideration during a consultation are listed in Table 6.4.
Clinical Setting
Ideally, all voice disordered patients should be managed by an ENT surgeon and speech pathologist (SP) with a specialized interest in voice disorders. Different models of working exist such as independent working but an integrated team approach, a joint voice clinic (SP + ENT), parallel clinics (SP-led clinic with ENT input available), and SP alone (SP sees triaged referrals). The availability of these services is determined by the enthusiasm and collective experience of the team members, the types of referrals seen in the department, and pragmatism. Other members of a voice disorders service may include a singing teacher, clinical psychologist, osteopath, and physiotherapist. A key element of a voice clinic is the availability of stroboscopy. This is a pragmatic tool for the detailed assessment of the vibrating vocal folds (see Chapter 7). Other imaging techniques such as high-speed digital video recording and videokymography are gaining in popularity and are useful in understanding complex vibratory behavior. Other common methods of assessment include acoustic analysis, electromyography, electrolaryngography, and aerodynamic measurements (see Chapter 7). These can be used to provide supporting evidence for the diagnosis, the objective evaluation of severity, and specific outcome measures.
History
In voice assessment, it is necessary to take a detailed history. It is important to determine the following:
•The nature and chronology of the voice problem.
•Exacerbating and relieving factors.
•Lifestyle, dietary, and hydration issues.
•Contributing medical conditions or the effects of their treatment.
•The patient’s voice use and requirements.
•The impact on their quality of life and social and psychological well-being.
•Their expectations for outcome of the consultation and treatment.
•The patients’ complaints which are most frequently related to changes in voice quality (hoarseness, roughness, and breathiness).
•The diagnosis •Prognosis and the consequences if the condition is not treated •Uncertainties in the diagnosis and possibilities for further investigation •Options for treatment, including the option of not treating •The purpose of proposed investigation or treatment, details of therapies, including subsidiary treatment such as pain relief, and details of what the patient can expect to experience •Details of common side effects •Explanations of the benefits of each option for treatment •Details of serious or frequently occurring risks and lifestyle changes that may be necessary as a result of the treatment •Advice as to whether the treatment is experimental (or evidence for treatment is poor) •How the patient’s condition and possible side effects may be monitored •The name of the health professional in charge of the treatment and names of senior team members if appropriate •Whether students or trainees may be involved •The right to change their mind at any time •The right to seek a second opinion •Details of any costs or charges, if applicable |
Adapted from http://www.gmc-uk.org/static/documents/content/Consent_0510.pdf.
•A pitch that is too high or too low, which is not appropriate for their age and sex.
•An inability to control the voice as required (pitch breaks, voice cutting out).
•An inability to raise the voice or make the voice heard in a noisy environment (reduced loudness).
•An increased effort and/or reduced stamina of the voice, or one that tires with use.
•Difficulties or restrictions in the use of the voice at different times of the day or related to specific daily, social or work-related tasks.
•A reduced ability to communicate effectively.
•Difficulty in singing.
•Throat-related symptoms (soreness, discomfort, aching, dryness, and mucus) particularly related to voice use.
•The consequent emotional and psychological effects caused by the above.
Patients generally use descriptive terms less precisely than clinicians, so a degree of interpretation is required. They will complain or have a voice problem that generally reflects impairment, limitations of activity, and occasionally lack of ability to participate in an activity (http://www.disabilitaincifre.it/documenti/ICF_18.pdf). Self-rating questionnaires such as the Voice Handicap Index,21 Voice-Related Quality of Life,22 and Voice Symptom Scale23 have been developed on the basis of the complaints of patients attending with voice problems (see Chapter 10). The most common impairments relate to the quality of the voice, the pitch, the ability and effort required to produce a loud enough voice, and other throat symptoms. The following is a general guide to the interpretation of vocal complaints and their possible etiology.
Voice Quality
Patients may use the term hoarseness to describe any abnormality of voice quality including roughness, breathiness, weakness (asthenia), and strain. The clinician needs to decide which elements are present and which are most dominant by carefully listening to the voice. This can be quantified using the grade of hoarseness, roughness, breathiness, aesthenia, strain (GRBAS) perceptual rating scale (see Chapter 10).24
Hoarse, Croaky, Rough, Gruff, or “Rusty” Voice
This rough or harsh quality to the voice is usually due to irregular (aperiodic) vibration of the vocal folds. The sound may be coarser if supraglottic structures, for example, the false folds or aryepiglottic folds, are involved. It is one of the most common complaints in patients with structural or inflammatory lesions of the vocal folds and in some forms of muscle tension dysphonia.
Creaky Voice
A creaky voice is characterized by a low-pitched (7 to 78 Hz), “popping quality” voice. The vocal folds are normal but tend to close quickly and peel apart slowly resulting in prolonged vocal fold contact with a sudden short opening burst as part of a long vibratory cycle.25 It is considered to be part of the normal range of voice qualities and appears to be becoming more used in everyday speech, particularly in young women at the end of utterances.26,27 It can become a problem if it becomes habitual and the patient is required to project the voice or vary the pitch as the range is usually reduced. Raising the loudness of the voice is difficult in creaky voice, for example, while singing, without amplification.
Breathy Voice
Breathiness reflects an inability to bring the vocal folds together and there is a consequent leakage of air through the glottis. It most commonly results from neurological problems such as a vocal cord palsy or paresis,28 structural problems such as sulcus vergeture,29 and muscle tension dysphonia such as Morrison Type 4 pattern13,14 and presbylaryngis.30 Myasthenia gravis can rarely present with isolated phonatory and speech symptoms such as breathiness, reduced loudness, hypernasality, and dysarthria.31
Roughness with Breathiness
Breathiness can be associated with a degree of roughness if the vocal folds vibrate irregularly due to a lesion that physically prevents glottal closure such as a polyp or large ventricular cyst. Conversely, lesions such as vocal fold nodules may be secondary due to tensioning of vocal folds such that the shearing forces on the mucosa cause the localized tissue damage of the nodule. In some circumstances, inadequate glottal closure may also result in the false cords vibrating. If the vocal folds are flaccid due to atrophy, presbylaryngis, or a bilateral paresis, they may vibrate irregularly and with large amplitude, which can also add a rough quality to breathy voice.
Whispery Voice
A whispery voice is produced by turbulent airflow through adducted but nonvibrating vocal folds. If the vocal folds are severely inflamed and phonation is painful or difficult, whispering may be easier and more comfortable for the patient. Sometimes this pattern of speaking continues when the original illness has resolved. Splinting of the vocal folds apart can also be the result of a severe primary muscle tension imbalance (whispery dysphonia)13,14 or secondary muscle tension imbalance due to poor coordination of breathing with phonation often due to psychogenic reasons.32 If there is severe structural damage to the vibrating structures of the larynx from trauma and scarring, then there may be no alternative to using a whispery voice if supraglottic structures are not employed as a sound source.
“No Voice” or Aphonia
“No voice” or aphonia may rarely be an extreme form of a breathy voice due to a bilateral adductor vocal fold palsy secondary to a lesion in the brainstem or fixation of cricoarytenoid joints in an abducted position. More commonly, this is due to a psychogenic muscle tension dysphonia.32 The vocal folds can either be held together so tightly than no air can pass through or are splinted apart and the breath is held. In rare cases, there may be a dominant cerebral hemisphere lesion affecting Broca area causing an apraxia of phonation, while other widespread cortical lesions cause mutism.33
Voice Breaks
This can be in the form of pitch breaks where the voice cracks, squeaks, or becomes (usually) high pitched. Pitch breaks can be used with effect in singing when these are known as register transitions34 or mode changes.35 A patient, however, may have no control over what sound is going to come out. Alternatively, the voice may cut out all together. Voice breaks result when some parameter of the vibrating system is changed (e.g., lung pressure, vocal fold tension, or there is an asymmetry of tension or mass between the two vocal folds).2 For example, failure to maintain an adequate subglottic pressure with adequate breath support is one cause. Voice breaks may also be present when the vocal folds are inflamed, there is a primary muscle tension imbalance such as puberphonia or secondary tensioning asymmetries such as a superior laryngeal nerve palsy. Structural abnormalities of the free edge of the vocal folds such as polyps and nodules can lead to vocal fold mass asymmetry or cause voice breaks from the lesion “catching” on the contralateral vocal fold.
Diplophonia
This is when two distinct pitches can be perceived simultaneously during phonation. It can result from tensioning imbalance in primary muscle tension dysphonia, secondary to a subtle neurological weakness such as a paresis,36 or when there is a difference in mass between the two vocal folds due to a structural abnormality such as an intracordal cyst.37 The cyst can act as a vibratory node causing one vocal fold to vibrate at a different phase anterior and posterior to the lesion or at different frequencies. There may also be associated voice breaks.
Tremor
Tremor is a regular wobble or shakiness of the voice (5 to 12 Hz). It is more common in the elderly in isolation or as one of several tremors affecting different parts of the body (essential tremor). It can be present together with other neurological conditions such as cerebellar ataxia (2 or 3 Hz), spasmodic dysphonia (irregular frequency),38 and late-stage Parkinson disease (4 to 7 Hz).39
Fundamental Frequency and Pitch of the Voice
The fundamental frequency of the voice is the measurable vibratory frequency of the sound source, which is in most cases the vocal folds. Pitch is a psychoacoustic phenomenon defined as “that attribute of auditory sensation in terms of which sounds may be ordered on a scale extending from low to high.”40 Pitch depends primarily on the frequency content of the sound stimulus, but it also depends on the sound pressure and the waveform stimulus.41 In other words, although the pitch ascribed by our brains to a certain sound is most usually determined by the fundamental frequency, it is also influenced, and can be derived solely, from the higher harmonics and the loudness of the sound.40 This leaves room for different perceptions of pitch level of the voice by different listeners, which can be at odds with measured fundamental frequency.
In addition to these psychoacoustic difficulties, there are many factors that determine what is perceived as a normal pitch for an individual’s voice. These include anatomical, physiological, social, and cultural influences. As a rough guide, the mean fundamental frequency of adult men during speech ranges between 100 and 150 Hz, between 180 and 250 Hz for adult women, and between 205 and 290 Hz for children.42
Pragmatically, the inappropriateness of the pitch is defined as that judged by the patient and assessor to be outside the normal range based on the age and sex of the individual.
Too High
This is quite a common perceptual finding but is rarely a complaint in women except when the voice has changed or is associated with other vocal complaints. In women, the commonest cause is muscle tension imbalance (lateral compression or Morrison Type 2) resulting from habitual talking at the top of the range of the voice, a common tendency in primary school teachers.13,14 This can result in chronic stretching of the vocal folds and pitch instability. In men, a high-pitched voice can cause negative comments about gender and lead to ridicule and psychological problems. It can result from muscle tension imbalance known as puberphonia or “mutational falsetto.”43 In these cases, the voice commonly never changed at puberty, although the laugh or cough may have a deep tone. Structural abnormalities and neurological problems need to be excluded. Structural problems include sulcus vergeture and an anterior glottis web. In sulcus vergeture, there is a longitudinal groove in the membranous portion of the vocal fold and is frequently bilateral. There is tethering of the epithelium to the underlying ligament or vocalis muscle.44 The thin, stretched free lower edge of the vocal folds make contact, which allows more regular vibration than if the stiffened area is involved. The consequence is a high-pitched voice with reduced pitch range. The voice can also be breathy, lack power, and projection.45 Anterior glottic webs can be congenital or acquired. Both can cause significant high-pitched voices and dysphonia.
In recurrent laryngeal nerves palsies, the compensatory unbalanced pull of the laryngeal muscles leads to asymmetry of the glottis and stretching of the vocal folds. This leads to a high-pitched voice with the breathiness from glottal gap. In advanced Parkinson disease, the mean speaking fundamental is raised compared with age-matched men but not in women and not for early-stage disease.39
Too Low
A low pitch to the voice is a much more common complaint in women who often get comments about sounding like a man, particularly on the phone. The most common cause is Reinke edema in which there is an increased amount of extracellular matrix produced in the superficial lamina propria.46 This is strongly linked to smoking.47 Large polyps, the use of the false folds during phonation, use of androgenic drugs, severe hypothyroidism, and some forms of muscle tension dysphonia will also result in a lower pitched voice.
Altered Pitch Range
The whole pitch range may have shifted, often becoming lowered. This can result from natural changes with age or from the structural effects of increasing the mass of the vocal folds, for example, from smoking. The pitch range may have become narrowed or monopitch, that is, lacks variation in speech. This can be due to personality issues, anxiety, and depression. It can also be a feature of neurological conditions such as Parkinson disease39,48 and in recurrent laryngeal nerve palsy.49 A patient may choose to limit the pitch variation if straying outside that range results in instability of the voice or is more effortful particularly in structural or neurological conditions.
Singers
Singers who are struggling with their pitch range may, for example, need to change key to sing a range of notes in a specific song. Loss of the top end of the range of the voice or difficulty with certain parts of their range may be because of inadequate technique in making transitions between registers or modes of the voice.35
Loudness of the Voice
Not Loud Enough
Reduced loudness of the voice may result from neuromuscular problems such as vocal fold palsies or paresis, Parkinson disease, or myasthenia gravis where there is a physical inability to oppose the vocal folds.39,48 Muscle tension imbalance, structural abnormalities, and inflammation may have variable effects on the ability to produce a loud voice. Sometimes the loudness reduces with voice use. Alternatively, it may only be an issue in noisy environments or when there is a need to project the voice.
Too Loud
Most patients will not complain about this but it may be apparent to the listener. It is common in muscle tension dysphonia when it may be a manifestation of an extrovert personality, a need to be heard when there are other dominant siblings or when the voice cannot be regulated when there is an untreated hearing loss. Occasionally, it may be necessary to increase the subglottic pressure to overcome the inertia of the vocal folds from structural or inflammatory causes. The result can be uncontrolled regulation of loudness and may be associated with voice breaks.
Other Throat Symptoms
Throat symptoms may be present with any of the four etiologic conditions. These include paralaryngeal discomfort or soreness of the throat from the increased effort of phonation (Table 6.5). Dryness of the throat is a common complaint in many types of voice disorder. Specifically, it can be due to medications such as diuretics or antimuscarinics, not drinking enough fluids, too much consumption of sugary or caffeine-containing foods and drinks, a persistent glottic gap or excessive autonomic stimulation secondary to anxiety, throat clearing, and mucus in the throat.50
Endoscopic Laryngeal and Vocal Tract Examination
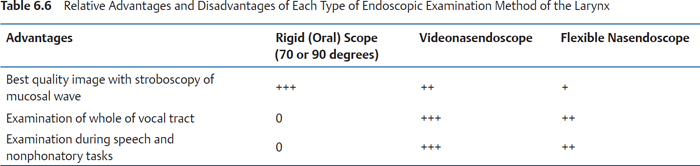
Based on the history, it should be possible to make a preliminary differential diagnosis. It is, however, virtually impossible in most cases to make a confident diagnosis without examining the larynx. Both oral rigid (70 or 90 degrees) endoscopes and flexible or video nasendoscopes should be available and also a continuous (halogen or xenon) and stroboscopic light source and a digital imaging capture system for storage and replay.51 Stroboscopic light used with a rigid endoscope gives the best quality image of the mucosal wave particularly when used with a high-definition camera. Nasendoscopes (diameter 3.2 to 4.8 mm) allow examination of the whole of the vocal tract, including the nasal cavity, and also examination of the patient during speech and nonphonatory tasks such as coughing and swallowing, for example, FEES (functional endoscopic evaluation of swallowing). Video nasendoscopes now allow much improved imaging with stroboscopy, which was previously limited with the fiberoptic nasendoscopes. High-speed digital imaging and videokymography can provide additional useful information when the vibratory patterns are complex, but are not in general use as yet.
Paralaryngeal discomfort or pain Soreness, burning, or tickling in the throat Feeling of a lump or something stuck in the throat (globus) Tightness or feeling of being strangled Throat dryness Mucus or catarrh in throat Needing to clear throat Irritating cough Choking episodes Difficulty swallowing |
The choice of examination technique depends on the quality and availability of the equipment and the specific aim of the assessment (Table 6.6). If a subtle abnormality of the mucosal wave is suspected, then good quality images using stroboscopy should be employed. If a neurological or muscle tension problem is likely, then nasendoscopy with continuous light source is more useful. Inflammation can be assessed with either method. Sometimes both methods need to be employed and patient preference needs to be considered. There are patients who hate anything in their nose and others who have too strong gag reflexes to tolerate a rigid endoscope. Rigid endoscopy can be used in many children from 5 years of age, although views are generally brief. Pediatric nasendoscopes (diameter 2.2 to 2.8 mm) allow neonates upward to be screened for pathology and laryngeal movement abnormalities such as vocal cord palsies and laryngomalacia.
As part of the assessment, it is essential to check each anatomical site and subsite for the presence or absence of the four etiologic factors together with a series of phonatory and nonphonatory tasks (Table 6.7). The phonatory tasks include checking the degree of closure of the vocal folds and supraglottic structures on phonation and the change in the mucosal wave with change in pitch and loudness. Nonphonatory tasks include observing adduction and abduction of the vocal folds on coughing and repeated “i”/sniffing looking for asymmetry and a lag in movement between the two sides.
Further Clinical Evaluation
Palpation of the neck is also another key part of the assessment. This is not only to detect enlarged lymph nodes or other structural abnormalities in the neck but also to detect evidence of muscle tension. In muscle tension dysphonia, the paralaryngeal and other anterior neck muscles are often chronically contracted and tender. The most consistently abnormal muscles are the cricothyroid, thyrohyoid, middle constrictor, and suprahyoid muscles.52,53
Further Evaluation
In spite of a detailed history and examination, it is sometimes still not possible to make an accurate diagnosis. In these cases, further investigations may be required including acoustic and electrolaryngographic analysis of the voice, laryngeal electromyography, a diagnostic microlaryngoscopy, and high-definition computed tomography scan of the larynx. Trials of medication and probe voice therapy are also useful and are covered in other chapters of the book.
Summary
Once the main types of etiologic factor have been identified by detailed history, careful voice assessment, neck palpation, and laryngostroboscopic examination, it is then possible to be more precise in the diagnosis. Fig. 6.2 summarizes the steps in clinical assessment and Table 6.8A–D describes the more common conditions encountered in patients presenting with hoarseness.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


