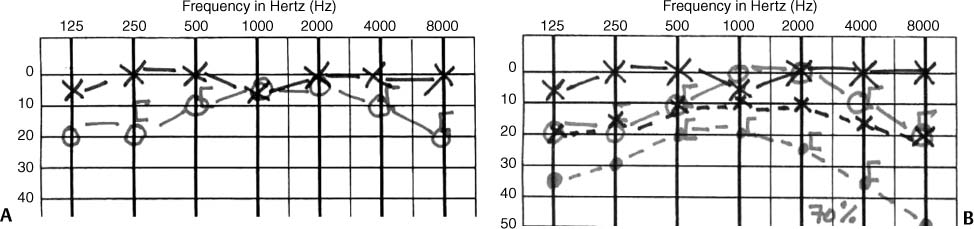
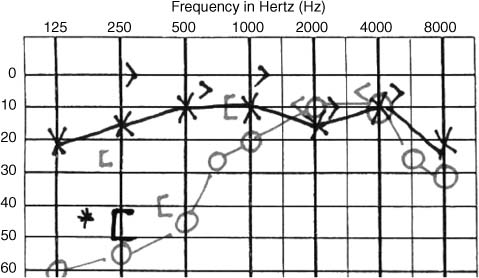
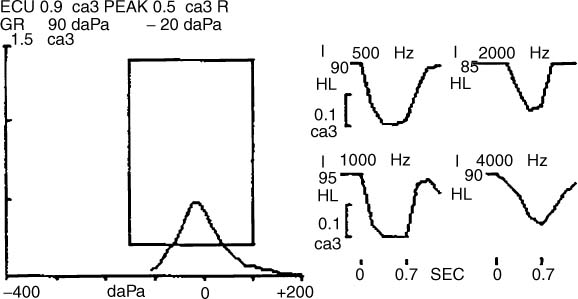
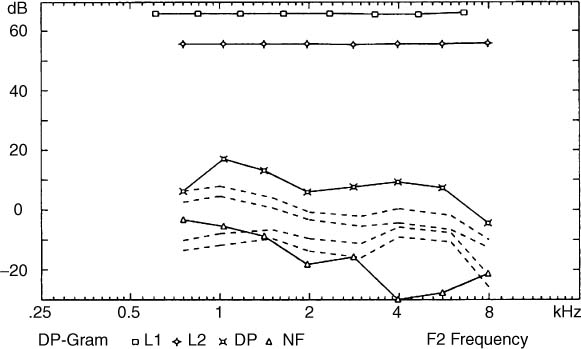
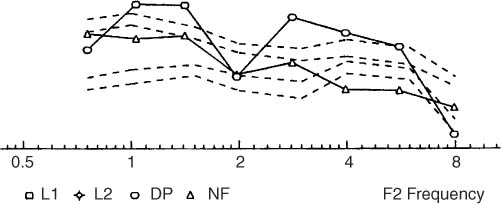
5 Clinical Approach to Patients with Auditory and Vestibular Disorders This chapter focuses on the practical clinical approach to patients with hearing and vestibular dysfunctions, and it discusses history taking, physical exam, diagnostic tests, and management. As with other fields of medicine, the history and physical examination are critical in helping the physician decide on the most effective evaluation protocol. That said, it is important to realize that the history alone is insufficient to make a final working diagnosis and that a traditional ear, nose, and throat (ENT) physical examination may not uncover vestibular deficits. Supplementary tests especially for the vestibular system are critical in this process. In medicine, history taking is an art that the practitioner develops with time and practice. Although standard questionnaires are very helpful and time saving in today’s environment, the physician should use them as a guideline. In this section, we discuss our approach to history taking, and readers are encouraged to develop their own. The basic components of a medical history include onset of symptoms, severity, fluctuation, progression, triggering and alleviating factors, and residual dysfunction or disability. Past medical history, review of systems, social history, allergies, and medications are also important components of a complete medical history. In eliciting a hearing loss history, determining the onset is important for differentiating congenital from acquired forms of hearing loss. Congenital hearing loss is usually discovered at birth with universal newborn hearing screening. The mother’s pre- and perinatal history of infection, drug abuse, and ototoxic medication are important to document. Adult-onset hearing loss is usually acquired and discovered by the patient or the family. Additionally, a history of unilateral and bilateral disease, aural fullness, tinnitus, and current subjective hearing deficit are important to determine. A family history of hearing loss and its pattern among family members is critical to determine hereditary forms of hearing loss. A detailed history of the nature and duration of noise exposure is important for both medical and legal purposes. A history of use of ototoxic medications and extended hospitalization is critical in cases of suspected ototoxicity. A past medical history of childhood or adult ear disease, ear surgery, trauma, and hearing screening tests is also important to determine. In eliciting a history of vertigo, dizziness, or imbalance, physicians should ask patients to use their own words to describe their symptoms. Patients can be guided when necessary so that, clinically, symptoms are classified into two main categories: vertigo and nonvertigo. Vertigo is the sense of rotational movement of the self or the surroundings. Nonvertigo includes light-headedness, unsteadiness, motion intolerance, imbalance, and floating or tilting sensations. This dichotomy is helpful because rotational vertigo is often due to inner ear disease, whereas nonvertigo symptoms may be due to central nervous system (CNS), cardiovascular, or systemic diseases. Sudden onset and vivid memory of vertigo episodes are often due to inner ear disease, especially if hearing loss, ear pressure, and tinnitus are present. Gradual and ill-defined symptoms are more common in CNS, cardiac, and systemic diseases. The duration and time course of vertigo are key components of the history. Are the symptoms episodic or constant? How long does each episode last? Is the patient normal between episodes? Episodic true vertigo that lasts for seconds and is associated with position changes is likely due to benign positional vertigo. Vertigo that lasts for hours or days is likely due to Meniere’s disease or vestibular neuronitis. Vertigo lasting for minutes can be due to vascular disease, especially if cardiovascular risk factors are present. Episodic motion sensitivity especially with physical exertion raises the question of perilymphatic fistula, especially if there is associated head or ear trauma. Continuous dizziness or motion sensitivity can be due to uncompensated peripheral vestibular disease, vestibular migraine, dehiscence of the superior semi-circular canal, or hyperventilation/stress. Falling and “drop attacks” are less common but important to evaluate for the safety of patients and others. Drop attacks that happen suddenly without syncope or prior warning signs can be due to “otolith crisis–Tumarkin” in late Meniere’s disease. Falling is a more gradual symptom and is usually due to sudden perturbation of posture. A history of prior viral illness, cold sores, sensory changes at the C2 to C3 levels, or cranial nerve V distributions usually point to vestibular neuronitis or exacerbation of a well-controlled Meniere’s disease. History of headaches, especially migraine headaches, is usually associated with migraine-related dizziness. Headaches with dizziness and pulsatile tinnitus, in an obese female patient, raise the question of benign intracranial hypertension. Postural imbalance, memory changes, and incontinence raise the question of the rare entity of benign intracranial hypertension. The presence of visual and autonomic symptoms or brainstem symptoms are important to rule out CNS disease. Incoordination and inability to walk during vertigo episodes can be due to cerebellar diseases, especially in the elderly. Sensory and motor symptoms and signs are usually associated with CNS diseases. The history should include a review of systems (especially head trauma and ear diseases) and screening for anxiety and depression. A history of prescription medications, over-the-counter medications, herbal medications, and recreational drugs (including smoking and alcohol) is helpful to identify pharmacologically induced dizziness and light-headedness. Traditional medical, neurologic, and ENT examinations of vertigo patients are often “normal”. Hearing loss and vestibular patients in particular need additional/complementary neurotologic examinations, such as auditory, vestibular, and neurologic examinations. It is also important to check the vital signs, including postural blood pressure changes. The ears are examined for obvious external or middle ear infection or inflammation. Examination of the ear with an operative microscope should be performed whenever there is a question about traumatic hearing loss, middle ear infection, or conductive hearing loss, or if the ear cannot be adequately examined with a handheld otoscope. Hearing is tested clinically using tuning forks and whisper tests. The vestibular examination starts with evaluating the neck for range of motion, rigidity, or increased muscle tone. Saccadic, pursuit, and optokinetic (OKN) nystagmus eye movements are examined in all cardinal directions. Post-OKN self-induced motion (circularvection) is usually correlated with visual-induced dizziness. It is also important to search for spontaneous and gaze-evoked nystagmus and to differentiate peripheral and central nystagmus. Generally, central nystagmus is purely horizontal or vertical and is evident when visual fixation. Peripheral nystagmus is usually rotatory and is present when removing visual fixation (e.g., under closed eyelids, use of Frenzel’s glasses, or video monitoring). A fairly reliable clinical impression of the horizontal and vertical vestibuloculomotor reflex (VOR) can be ascertained by observing (or video recording) the presence, intensity, and symmetry of per-rotatory nystagmus during passive and active head movements in the horizontal and vertical directions. For example, unilateral and bilateral reduced nystagmus responses can be observed during this test. The head-shake exam is critical because the presence of robust doll’s-eye movements and intact visual acuity with active head movements reflect adequate vestibular function or reserve. Poorly formed or absent doll’s-eye movements or a decrease in visual acuity with active head movements reflect decreased vestibular function, especially in patients suspected of ototoxicity (gentamicin or other ototoxic medications). Nystagmus, slow eye drift, and symptoms after rapid head shaking reflect asymmetric vestibular input usually secondary to uncompensated vestibular neuronitis or active Meniere’s disease. Post-head-shake nystagmus or ocular drift (slow phase drift) are very helpful in assessing symmetry and the status of vestibular compensation. For example, post-head-shake right beating nystagmus reflects underactive left vestibular dysfunction, whereas post-head-shake left ocular drift reflects decreased left function with incomplete central compensation. No post-head-shake nystagmus reflects either normal bilateral function or unilateral hypofunction with “complete” central compensation. Non paroxysmal positional nystagmus can be evaluated with the patient in the supine position and the head in the center, right and left positions. If nystagmus is present, it is usually direction fixed or, less commonly, direction changing. Nystagmus is usually of low velocity (5–10 deg/sec) and is suppressed with visual fixation. During this exam, we usually examine the effects of tragel compression, valsalva, noise or mastoid vibration with a handheld mechanical vibrator. Symptoms and nystagmus are observed and recorded as they may be associated with active hydrop (more common) perilymph fistula or dehiscence of the superior canal (less common). Nystagmus and vertigo during the Dix-Hallpike exam are typical findings in benign paroxysmal positional vertigo (BPPV) of the posterior canal or the horizontal canal. Details of interpreting the Dix-Hallpike exam are discussed in Chapter 6, but it is important to note here that while the exam is simple, the resulting symptoms and eye movements are not that simple. It is also important to ensure that there are no neck or spinal problems before conducting this exam, especially in the elderly patient. Also, the patient’s head does not need to be hyper-extended beyond the edge of the exam table. The stimulus is the acceleration motion from the sitting to the lying down position. Most of us do not lie down to sleep hyper-extending our necks, and patients complain of symptoms with such activities as lying down to sleep or looking up at bookshelves without neck “hyperextension.” This point is elaborated to avoid potential harm to elderly patients who usually do not have flexible neck movements. Focused neurologic examination of the cranial nerves, motor and sensory modalities, gait, and stance is important at the initial visit. Cerebellar tests, especially failure of fixation suppression of vestibular eye movements, are important for checking the vestibulocerebellum. Failure of fixation suppression can be tested by asking patients to stretch their arms and look at their thumbs while being passively rotated (manual rotation of examination chair). A visible nystagmus (left or right) indicates failure of fixation suppression that is always central in origin. Stance and gait are evaluated for qualitative ability to stand up without assistance, gait speed, and stride length. The traditional Romberg test is usually not challenging to the posture system and does not evaluate the limits of stability and strategy. The use of a high-compliance foam pad to examine posture control is very helpful in “stressing” the vestibular system to evaluate postural sway, the limits of stability, and postural strategies (hip versus ankle sway). These parameters are helpful in addressing the pathophysiology of falling and in tailoring appropriate vestibular rehabilitation programs. This is very critical in elderly patients who are evaluated for the primary complaint of falling. When the above exams are normal and the history is not specific for a primary ear or brain disease, having the patient hyperventilate for 2 minutes is helpful in identifying the hyperventilation syndrome, particularly if it reproduces the patient’s symptoms. Posthyperventilation nystagmus is an objective sign of vestibular disease. In the course of evaluating patients for hearing and balance disorders, additional tests that are commonly considered include audiometry, vestibular tests, blood tests, computed tomography (CT) and magnetic resonance imaging (MRI). These tests need to be tailored according to the history and physical findings. This section describes the different tests commonly used in the course of evaluating the neurotologic patients. Audiologic and vestibular tests are composed of several behavioral and electrophysiologic tests. They are often conducted by qualified audiologists, who also provide electrophysiologic interpretations of these tests. It is important to realize that these tests are not diagnostic in the medical sense. For example, conductive hearing loss can be due to external, middle, or inner ear disease. A unilateral vestibular loss can be due to vestibular neuronitis or an acoustic tumor. It is therefore critical to avoid the temptation to interpret these tests as indicative of pathologic entities. Physicians who are responsible for the medical interpretations of these tests should also have the proper training and background in neurophysiology and electrophysiology to be able to utilize these results effectively. They also must be aware of the limitations and variability inherent in such tests. The specialty of auditory and vestibular medicine is evolving. A team approach based on mutual understanding and appreciation between scientists and physicians is optimal for the management of patients with hearing and balance disorders. Basic and advanced audiologic evaluations include air and bone conduction thresholds, speech discrimination scores, tympanometry with stapedial reflexes, and distortion product otoacoustic emissions (DPOAEs). Patients with tinnitus are tested for tinnitus matching and residual inhibition parameters. A typical audiogram is shown in Fig. 5–1. Although traditional teaching implies that thresholds above 20 dB are normal, it is clear in this audiogram that there is asymmetric hearing loss within the normal range. This is emphasized because a repeat audiogram in this case 3 months later clearly shows definite hearing loss. Audiometric air thresholds should be tested between 125 Hz and 8 kHz to identify a low-frequency rising pattern, a peak pattern, and a high-frequency sloping pattern. Certain audiometric profiles correlate with different inner ear diseases; for example, low-frequency rising and peak patterns are usually seen in Meniere’s disease, whereas high-frequency sloping patterns are usually seen in age-related and noise-induced hearing loss. Bone conduction thresholds should be measured at 250 Hz to 4 kHz. It is important to determine bone conduction thresholds below the 0-dB level to identify bone conduction hypersensitivity, commonly seen in patients with dehiscence of the superior canal. The audiogram is interpreted to reflect normal hearing, conductive hearing loss, or mixed hearing loss. It is clinically important to double check pure tone thresholds with tuning forks, especially in cases with conductive hearing loss, to avoid the potential of undermasking (Fig. 5–2). Masking is very important to ensure accurate determination of the thresholds of the tested ear and to avoid a false air–bone conduction gap. Masking of the nontest ear with narrow band noise should be applied if the air conduction thresholds difference between the two ears exceeds 40 dB or when the bone conduction of the better ear is 40 dB higher than the air threshold of the test ear. The 40-dB level represents the interaural attenuation when headphones are used. Masking is applied during bone conduction testing whenever there is a 10-dB difference between the two ears. Figure 5–1 Pure tone audiograms. (A) Normal left thresholds. The right ear thresholds, although in the “normal range” are clearly lower than the right ear. (B) The patient had mild right ear symptoms and repeat test in 3 months reveals moderated loss in the right ear and mild loss in the left ear. Note that the right speech discrimination dropped to 70%. This is a typical presentation of patients suspected to have immune-mediated hearing loss. Figures 5–2 The audiogram bone conduction of the left ear is at “0” and can be also recorded at “–5 dB” in cases of bone conduction hypersensitivity. The right ear shows mixed hearing loss despite adequate masking. This is a “false” conductive loss because the 256-Hz tuning fork did not show conductive loss and the tympanogram (Fig. 5–3) is normal. The speech in noise (white or conversational noise) test1 should be routinely performed to determine speech discrimination, especially in patients who have difficulty hearing in background noise and in patients undergoing hearing aid fitting. In our opinion, audiograms with no speech discrimination scores are incomplete. Furthermore, current speech tests using spondees and phonetically balanced words may not be sufficient to evaluate the true ability of speech discrimination. We have encountered patients with speech discrimination scores of less than 50% who were able, with appropriate amplifications, to accurately answer open-ended questions with no lip reading. Although not frequently utilized, the threshold equalizing noise (TEN) test2,3 is becoming an important part of audiometry to determine cochlear dead regions, especially in understanding cochlear physiology and in optimizing hearing aid fitting. Tympanometry is the common term used for immittance audiometry, which provides an objective evaluation of the middle ear compliance by measuring tympanic membrane (TM) movement to applied air pressure (300 to +300 mm H2O) in the external canal. A negative middle ear pressure or a noncompliant middle ear is consistent with eustachian tube dysfunction or middle ear effusion. The normal tympanogram (type A) and ipsilateral stapedial reflexes are shown in Fig. 5–3. Abnormal shapes of the tympanogram are classified as type C (normal with negative middle ear pressure), type As (normal with low peak amplitude; increased middle ear stiffness), type Ad (normal with high peak amplitude; flaccid TM or ossicular discontinuity), type B (flat, non-compliant middle ear), or type D (flaccid with disarticulation). Ipsi- and contralateral acoustic reflex thresholds are also measured during tympanometry. Typically acoustic reflex thresholds are in the range of 85 dB for the middle frequency range (200–500 Hz). Elevated thresholds are seen in sensorineural hearing loss and recruitment. Absent thresholds are consistent with conductive hearing loss (more common), sensorineural hearing loss without recruitment, or central etiology (less common). A clinically important use of tympanometry and acoustic reflex is with conductive hearing loss as shown in Fig. 5–3. The conductive hearing loss in the low frequency could be due to either fixed ossicles or cochlear conductive loss due to secondary hydrops of the saccule. The presence of an acoustic reflex eliminates the possibility of a stapes fixation and points to cochlear conductive loss. This distinction is clinically important because the treatment is very different for the two conditions. Figure 5–3 Normal tympanogram and ipsilateral stapedial reflexes. Figure 5–4 Normal distortion product otoacoustic emission (DPOAE). The solid lines represent the signal (echo, DP) and the noise floor (NF). The dotted lines are the normal range for DPOAE. L1, L2 are the signal levels of the f1 and f2. Note that the NF is higher at the low frequency. Otoacoustic emissions (OAEs) have become a routine part of the full audiologic evaluation of patients presenting with hearing disorders.1,2 OAEs are sounds generated by the normal healthy cochlea, specifically the outer hair cells, and recorded from the external canal. The most clinically used OAEs are the evoked OAEs (EOAEs) because of their higher sensitivity and specificity. EOAEs are present in almost all normal hearing ears with thresholds better than 40 dB and are further divided into transient (TOAEs) and distortion product (DPOAEs) types. The TOAEs are evoked by sound clicks (sound pulses with energy in the 500- to 5000-Hz range) and the response, therefore, is generated by all outer hair cells on the basilar membrane. TOAEs have the advantage of being recorded in a relatively short time and thus are useful for screening neonates and difficult-to-test children. The DPOAE, on the other hand, is generated by using two stimulus frequencies staggered in pitch and loudness to stimulate specific areas on the basilar membrane to produce a frequency-specific response. DPOAEs take a bit longer to test and currently are the most utilized OAEs protocol. A normal DPOAE is shown in Fig. 5–4. OAEs are clinically useful in differentiating the level of auditory dysfunction. In general, absent OAE is associated with end-organ hearing loss. For example, asymmetric hearing loss and absent DPOAEs (Fig. 5–5) probably reflect end-organ loss, and an MRI may not be needed, especially if the auditory brainstem response (ABR) is normal and stapedial reflexes are present. A less utilized aspect of OAE is its suppression with contralateral noise stimulation via the medial olivocochlear bundle.3 This test may be useful in patients with hyperacusis and intractable tinnitus as well as those with possible inferior vestibular nerve dysfunction. Figure 5–5 Abnormal DPOAE showing no echo at the 2-kHz mean frequency. This patient had a 30-dB notch on the audiogram. Note that the low and high ends do not show echo because of a higher noise floor (NF) signal. The dip, however, is not affected by the NF.
History
Physical Examination
Diagnostic Tests
Audiologic Tests
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


