Cleft Lip & Palate: Introduction
In large series, the distribution of clefts is about 50% cleft lip and palate, 30% cleft palate only, and 20% cleft lip only. Cleft lip occurs most often on the left side; the distribution of left to right to bilateral cleft lip is approximately 6:3:1. Right-sided clefts are more commonly associated with syndromes. There is a slightly higher incidence in males.
Modern ultrasound can identify cleft lip by the absence of muscle fibers crossing the lip. Specific efforts must be made to obtain a frontal view to make a prenatal diagnosis. Newer ultrasounds have increasing accuracy. Although fetal surgery for clefts is not yet feasible in humans, prenatal diagnosis makes it possible to counsel parents earlier and prepare them for the care that their new child will require (Figure 20–1).

Embryology
It is important to remember the embryology of clefting; the primary palate includes the lip and premaxilla, whereas the secondary palate extends from the incisive foramen back. The lip and alveolus are formed by the fusion of the frontonasal process and the lateral maxillary processes; this fusion is reinforced by the migration of mesenchymal tissue derived from neuroectoderm (Figure 20–2). The stabilization of neuroectoderm by folate during the first trimester of pregnancy has been shown to reduce the incidence of clefting as well as that of other neural crest defects such as myelomeningocele.

Anatomy
An understanding of the anatomic derangements is critical to proper repair. In the cleft lip, the orbicularis oris muscle is interrupted, and the remnants of the muscle adjacent to the cleft flow toward the upper portion of the cleft, at the base of the columella medially and at the alar base laterally. Incomplete clefts have variable amounts of muscle intact across the upper portion of the lip. In bilateral complete clefts, there is no muscle in the central portion (the prolabium).
Normally, the levator palatini muscle forms a sling that elevates the soft palate and excludes the nasopharynx from the oropharynx during speech and swallowing. In the cleft palate, the levator muscle is oriented longitudinally, parallel with the cleft margin. This abnormal orientation of the muscle is even seen in submucous cleft palate, when the mucosa is intact (Figure 20–3). The most recent techniques of cleft palate repair incorporate reorientation of the levator muscle as part of the repair, which contributes to the improved speech results seen today.

The tensor palatini muscle is also abnormally oriented, more longitudinally than normal; this results in inadequate opening of the eustachian tube in children with cleft palate. It also explains the high incidence of serous otitis media seen in these children; almost all children with clefts require myringotomy and tube placement in early development. As they grow, the eustachian tube develops stronger cartilaginous support and the need for ventilating tubes is generally outgrown.
Classification
Clefts are generally classified as complete or incomplete. Complete cleft lip implies a separation of the lip that extends through the nasal sill and the alveolus into the palate. Incomplete cleft lip may present as a cleft of variable width with an intact bridge of skin below the nasal sill, known as a Simonart’s band. At the other end of the spectrum is the forme fruste or microform cleft lip, which may be as little as a small notch in the vermilion (Figure 20–4).


Clefts may also be unilateral or bilateral. As with unilateral clefts, bilateral clefts may be complete or incomplete, and these variants may be different on the two sides. In a complete bilateral cleft, the central portion of the alveolus, the premaxilla, is attached only to the nasal septum and the central lip or prolabium is attached only to the premaxilla and the columella. These cases pose a particular problem because the premaxilla migrates anteriorly and can be virtually horizontal in orientation. The premaxilla must be brought down into a closer relationship with the lateral segments in order to achieve a bilateral cleft lip repair (Figure 20–5).
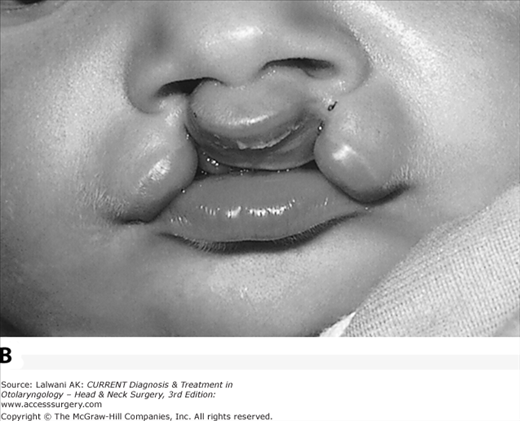
Figure 20–5.

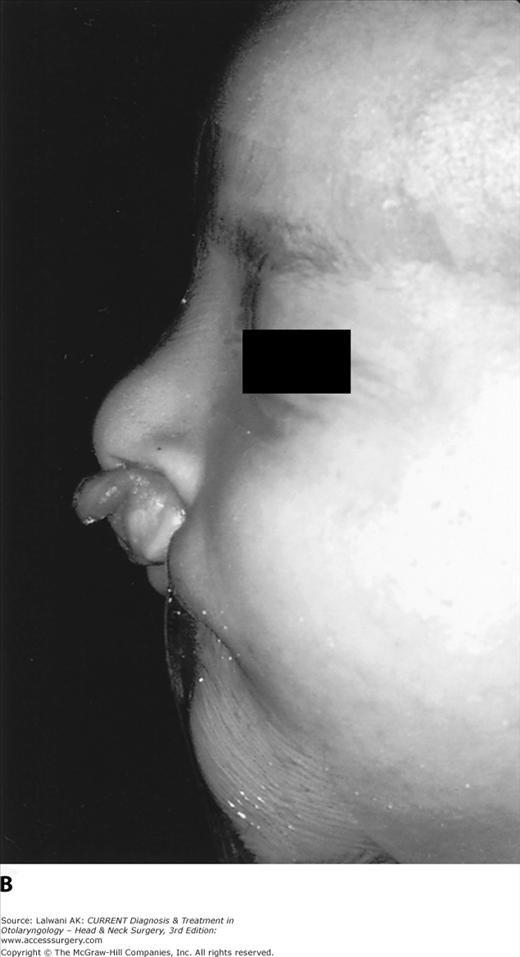
Bilateral complete cleft lip. (A) Anteroposterior view. The central portion, the prolabium, is of fairly good size in this example. (B) Lateral view. Note the short columella and the anterior displacement of the prolabium and premaxilla due to the interruption of the orbicularis oris muscle.
Complete cleft palate occurs in association with complete cleft lip, whereas incomplete cleft palate refers to a cleft of the secondary palate only. As with the lip, the presentation of incomplete clefts has a great deal of variability, from a wide cleft of the palate extending all the way forward to the incisive foramen, to a narrow cleft of the posterior portion of the soft palate. The submucous cleft palate represents a specific entity with separation of the levator palatini muscles but intact mucosa.
Syndromes
Literally hundreds of congenital syndromes include clefting as one manifestation of a genetic abnormality. Together, these make up <20% of all clefts; those not associated with a syndrome are generally referred to as “isolated” clefts.
Velocardiofacial syndrome, or Shprintzen syndrome, is associated with a deletion at the 22q locus. This is the same locus involved in the DiGeorge syndrome, and there may be overlap with this syndrome of B-cell dysfunction. As the name implies, affected children have clefts (usually of the palate only), cardiac anomalies, and characteristic facial appearance. There may be velopharyngeal insufficiency in the absence of any cleft. Children with velocardiofacial syndrome have a developmental delay that may contribute to problems with speech. It is possible to test for the genetic deletion with fluorescent in situ hybridization (ie, FISH testing).
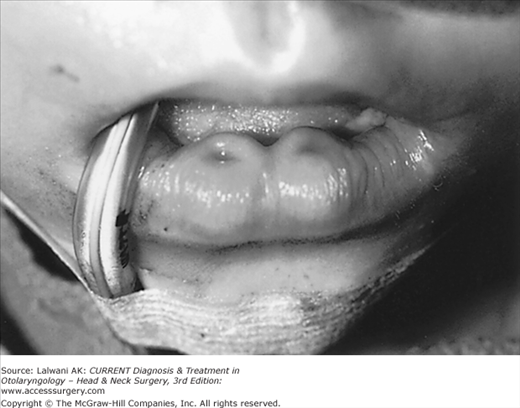
Van der Woude syndrome is an association of clefting with lower lip sinus tracts, known as lip pits. This syndrome is notable for autosomal dominant inheritance and for variable penetrance; even within a single family, affected children may have different presentations (Figure 20–6).
Stickler syndrome is an association between clefts and ocular abnormalities, including fairly severe myopia presenting at an early age, as well as retinal abnormalities. Generally, an examination by a pediatric ophthalmologist is recommended for children with clefts to make or rule out the diagnosis in the first year of life.
Pierre Robin Sequence
Pierre Robin syndrome is characterized by a triad of retrogenia, retrodisplacement of the tongue, and respiratory insufficiency. Most children with this syndrome also have clefts of the secondary palate, which are characteristically U-shaped clefts that are quite wide. The breathing difficulties seen in Pierre Robin sequence arise from posterior positioning of the tongue and upper posterior pharyngeal obstruction (Figure 20–7).

In most cases, the respiratory obstruction is seen immediately in the neonatal period. Turning the infant to the prone position may move the tongue forward and alleviate the obstruction. The placement of a nasogastric feeding tube permits better nutrition and also breaks the seal of the tongue against the posterior pharyngeal wall. Various types of oral airways have been used as temporizing measures to keep the tongue down and forward. Over time, the mandible grows forward in most cases and the problem improves.
If conservative measures fail in the neonatal period, surgical intervention is warranted. The goal of surgery is to avoid infant tracheostomy, which remains the final resort in these cases. In all cases bronchoscopy should be performed to rule out laryngomalacia or tracheomalacia, which would mandate tracheotomy. Tongue-lip plication, or glossopexy, is a simple procedure that requires an incision in the tongue just below the tip and in the wet vermilion of the lower lip; the two mucosal incisions are closed along with a retention suture that is tied over two buttons on the tongue and in the lower chin. This technique has been successful in avoiding tracheotomy in about 80% of cases in several large series. Recently, mandibular distraction has been used in infants to elongate the ramus and bring the tongue forward with the mandible. This is the preferred technique for treatment of PRS at a number of centers in the United States and elsewhere. The purported advantages are the high success rate, elimination of GERD, and the ability to repair the palate at an early age without airway problems. The long-term effects on mandibular growth are not known at this time.
Submucous Cleft Palate
Submucous cleft palate represents a special subset of clefts that remains confusing in both diagnosis and treatment. The diagnosis is made by the findings of the classic triad of a bifid uvula, central thinning of the soft palate, and a palpable notch in the posterior border of the hard palate (normally the location of the posterior nasal spine). Anatomically, there is the same separation of the levator palatini muscle that is seen in overt clefts.
In large prospective studies, most patients with submucous cleft palate do not have speech problems (ie, nasal air loss). However, it is not uncommon to see patients with nasal speech who have an unrecognized submucous cleft. Patients with submucous clefts should be observed as speech develops; if nasal air loss occurs, surgical intervention should be considered. The Furlow double-opposing Z-plasty is an excellent method for repair in these cases (see Treatment section below).
The care of children with a cleft lip and palate requires a comprehensive treatment plan from the initial diagnosis through the completion of reconstruction in adolescence. A child with a complete cleft lip and palate requires several operations as he or she develops. In general, the goal of treatment is to have as few operations as possible with the best possible outcome. Naturally, there are a variety of approaches, any of which may produce the same final result. A comparison of outcomes has been difficult because of treatment differences, as well as the fact that the experience and ability of the individual surgeon may also influence the outcome.
It is important to emphasize the team approach to cleft care, which has developed gradually over the past 50 years. Although surgeons, speech therapists, and orthodontists, among others, may offer specific treatment, a dedicated cleft team offers the best possibility of coordinating the care among various specialists. This approach can both minimize the number and length of the various interventions as well as ensure that they are done at optimal times. The American Cleft Palate-Craniofacial Association has developed an outline of the standards for team care of cleft patients.
Before any surgery, it is important for the patient to have a thorough team evaluation, including genetic and pediatric examinations, which can lead to other studies to diagnose or rule out specific syndromes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


