77 Classifications • Healed COM: healed perforation, tympanosclerosis • Inactive mucosal COM: dry TM perforation, uninflamed ME mucosa • Inactive squamous COM: TM retraction, not retaining debris or infected • Active mucosal COM: TM perforation with mucopus, inflamed ME mucosa • Active squamous COM: cholesteatoma • TOS classification: pars flaccida/attic retractions • SADE classification: pars tensa retractions • Moffett–Smith classification • Fisch – C1: limited involvement of vertical portion of carotid canal – C2: invasion of vertical portion of carotid canal – C3: invasion of horizontal carotid canal • House–Brackmann • Class I (Chevallet): fronto/frontolateral blow with vertical fracture septum + depressed/displaced nasal bone • Class II (Jarjavay): lateral blow with horizontal C-shaped fracture septum + perpendicular plate of ethmoid and frontal process maxilla • Class III: fracture extends to ethmoid labyrinth, septum collapses into face, nasal bones pushed under frontal bone leading to telecanthus • Kadisch staging • Type 1: from molar extraction and healthy maxillary sinus (1–5 mm) • Type 2: from molar extraction and maxillary sinus acute/chronic disease (6–19 mm) • Type 3: secondary to surgical removal (>20 mm) • Draf I—frontal recess is defined + opened + agger nasi cell roof is “uncapped” • Draf IIA—frontal sinus opened between lamina papyracea and insertion of middle turbinate • Draf IIB—frontal sinus opened medial to middle turbinate by removal of most of anterior attachment of middle turbinate to skull base • Draf III • Andrews staging – A: without intracranial involvement – B: intracranial/extradural involvement – A: no cavernous sinus, pituitary fossa, or optic chiasm involvement – B: all areas above involved • Scores – 0 (not occluded) – 2 (occluded) • Areas scored • Score range • Anterior ethmoidal cells impinging on frontal recess or frontal sinus • Lindholt • (Alternative = grade I–IV where III is to nasal floor and IV is to anterior nares) • Type I: limited to the frontal sinus only with or without orbital extension • Type II: frontal and ethmoidal sinuses with or without orbital extension • Type IIIa: erosion of the posterior wall frontal sinus with minimal or no intracranial involvement • Type IIIb: erosion of the posterior wall with major intracranial extension • Type IV: erosion of the anterior wall of the frontal sinus • Type Va: erosion of both anterior and posterior walls of frontal sinus without or minimal intracranial extension • Type Vb: erosion of both anterior and posterior walls of frontal sinus a major intracranial extension • Tardy • Chandler • Keros • Krouse – Tumour with extranasal and extrasinus extension – Tumours associated with malignancy • Modified Krouse – Involvement of any maxillary wall (other than medial wall), or – Frontal sinus or sphenoid sinus • Krespi Table 77.2 Grading system for sinus cavities in post-op AFRS patients
77.1 Otology
77.1.1 Chronic Otitis Media
77.1.2 Retraction Pockets
 Type I: dimple/visible air space
Type I: dimple/visible air space
 Type II: retraction to neck of malleus + no visible air space
Type II: retraction to neck of malleus + no visible air space
 Type III: bony erosion (scutum); retraction beyond osseous malleus with full extent seen
Type III: bony erosion (scutum); retraction beyond osseous malleus with full extent seen
 Type IV: keratin accumulation/cholesteatoma
Type IV: keratin accumulation/cholesteatoma
 Type I: annular retraction
Type I: annular retraction
 Type II: retraction onto long process of incus/ISJ
Type II: retraction onto long process of incus/ISJ
 Type III: retraction onto promontory (nonadhesive)
Type III: retraction onto promontory (nonadhesive)
 Type IV: adhesion onto medial wall
Type IV: adhesion onto medial wall
77.1.3 Petrous Apex Cholesteatoma
 Supralabyrinthine: above the labyrinth
Supralabyrinthine: above the labyrinth
 Supralabyrinthine–apical: above the labyrinth extending to petrous apex
Supralabyrinthine–apical: above the labyrinth extending to petrous apex
 Infralabyrinthine: below the labyrinth
Infralabyrinthine: below the labyrinth
 Infralabyrinthine–apical: below labyrinth extending to petrous apex
Infralabyrinthine–apical: below labyrinth extending to petrous apex
 Massive labyrinthine: extensive destruction of inner ear
Massive labyrinthine: extensive destruction of inner ear
 Massive labyrinthine apical: extensive destruction of inner ear extending to petrous apex
Massive labyrinthine apical: extensive destruction of inner ear extending to petrous apex
 Apical: confined to petrous apex
Apical: confined to petrous apex
77.1.4 Glomus Tumours
 Type A: limited to middle ear
Type A: limited to middle ear
 Type B: limited to tympanomastoid area with no infralabyrinthine extension
Type B: limited to tympanomastoid area with no infralabyrinthine extension
 Type C: infralabyrinthine involvement to petrous apex
Type C: infralabyrinthine involvement to petrous apex
 Type D1: intracranial ext <2 cm
Type D1: intracranial ext <2 cm
 Type D2: intracranial ext >2 cm
Type D2: intracranial ext >2 cm
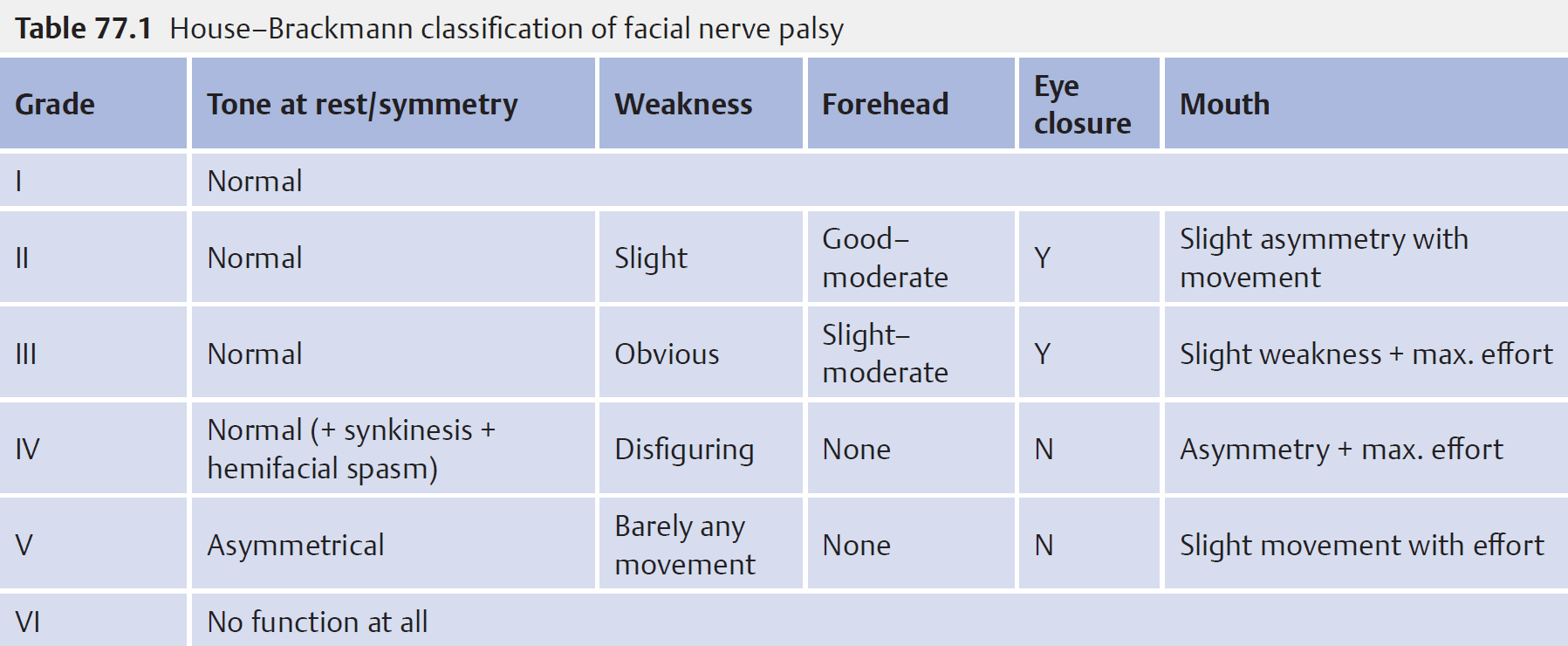
77.1.5 Facial Nerve Palsy
 See Table 77.1
See Table 77.1
 Clinically important to differentiate grade III from IV as this relates to patients’ ability to be able to fully close and therefore protect their eye
Clinically important to differentiate grade III from IV as this relates to patients’ ability to be able to fully close and therefore protect their eye
77.2 Rhinology
77.2.1 Nasal Fracture
77.2.2 Olfactory Neuroblastoma
 Type A: limited to nasal cavity
Type A: limited to nasal cavity
 Type B: + paranasal sinuses
Type B: + paranasal sinuses
 Type C: extension beyond
Type C: extension beyond
77.2.3 Oroantral Fistulas
77.2.4 Frontal Sinus Surgery
 Aka endoscopic Lothrop
Aka endoscopic Lothrop
 Transseptal frontal sinusotomy with superior part of nasal septum and floor of frontal sinuses and intersinus septum removed to create one large cavity
Transseptal frontal sinusotomy with superior part of nasal septum and floor of frontal sinuses and intersinus septum removed to create one large cavity
77.2.5 Juvenile Angiofibroma
 Stage I: limited to nasopharynx/sphenopalatine foramen with minimal bone destruction
Stage I: limited to nasopharynx/sphenopalatine foramen with minimal bone destruction
 Stage II: invading pterygopalatine fossa or maxillary, ethmoid, sphenoid sinus, and bone destruction
Stage II: invading pterygopalatine fossa or maxillary, ethmoid, sphenoid sinus, and bone destruction
 Stage III: invading infratemporal fossa or orbit
Stage III: invading infratemporal fossa or orbit
 Stage IV: intracranial intradural involvement
Stage IV: intracranial intradural involvement
77.2.6 Lund–Mackay Staging Sinus Disease on CT Scans
 0 (normal)
0 (normal)
 1 (partial opacification)
1 (partial opacification)
 2 (complete opacification)
2 (complete opacification)
 Osteomeatal complex:
Osteomeatal complex:
 Maxillary
Maxillary
 Frontal
Frontal
 Anterior ethmoid
Anterior ethmoid
 Posterior ethmoid
Posterior ethmoid
 Sphenoid
Sphenoid
 Osteomeatal complex
Osteomeatal complex
 0 to 24 (max. 12 each side)
0 to 24 (max. 12 each side)
 Score ≥4 for FESS or 2 with unilateral disease
Score ≥4 for FESS or 2 with unilateral disease
77.2.7 Kuhn Cells
 Type 1: single frontal recess cell above agger nasi
Type 1: single frontal recess cell above agger nasi
 Type 2: tier of cells in frontal recess above the agger nasi
Type 2: tier of cells in frontal recess above the agger nasi
 Type 3: single large cell extending beyond frontal os
Type 3: single large cell extending beyond frontal os
 Type 4: isolated cell within frontal recess—probably an artifact of older imaging protocols
Type 4: isolated cell within frontal recess—probably an artifact of older imaging protocols
77.2.8 Nasal Polyp Grading
 0: no visible polyps
0: no visible polyps
 1: polyps confined to middle meatus
1: polyps confined to middle meatus
 2: polyps below the middle turbinate
2: polyps below the middle turbinate
 3: massive polyps completely obstructing the nasal cavity
3: massive polyps completely obstructing the nasal cavity
77.2.9 Frontal Sinus Mucocele
77.2.10 Saddle Nose Deformity
 Minimal: supratip depression greater than the ideal 1–2 mm tip–supratip differential
Minimal: supratip depression greater than the ideal 1–2 mm tip–supratip differential
 Moderate: moderate degrees of saddling due to loss of height of the quadrangular cartilage, usually with septal damage
Moderate: moderate degrees of saddling due to loss of height of the quadrangular cartilage, usually with septal damage
 Major: more severe degree of saddling with major cartilage loss and major stigmata of a saddlenose deformity
Major: more severe degree of saddling with major cartilage loss and major stigmata of a saddlenose deformity
77.2.11 Orbital Cellulitis Complicating Sinusitis
 Group 1: preseptal cellulitis
Group 1: preseptal cellulitis
 Group 2: orbital cellulitis
Group 2: orbital cellulitis
 Group 3: subperiosteal abscess
Group 3: subperiosteal abscess
 Group 4: orbital abscess
Group 4: orbital abscess
 Group 5: cavernous sinus thrombosis
Group 5: cavernous sinus thrombosis
77.2.12 Olfactory Fossa Depth
 Type I: 1 to 3 mm
Type I: 1 to 3 mm
 Type II: 4 to 7 mm
Type II: 4 to 7 mm
 Type III: 8 to 16 mm
Type III: 8 to 16 mm
 Type IV: asymmetrical
Type IV: asymmetrical
77.2.13 Inverting Papilloma
 Type I: tumour confined to nasal cavity
Type I: tumour confined to nasal cavity
 Type II: tumour involving osteomeatal complex and ethmoids and/medial wall of maxillary sinus (with or without nasal cavity involvement)
Type II: tumour involving osteomeatal complex and ethmoids and/medial wall of maxillary sinus (with or without nasal cavity involvement)
 Type III: tumour involving any wall of maxillary sinus (but medial wall), sphenoid or frontal sinus, with or without stage II criteria
Type III: tumour involving any wall of maxillary sinus (but medial wall), sphenoid or frontal sinus, with or without stage II criteria
 Type IV:
Type IV:
 Type A: limited to within the nasal cavity, ethmoid sinus, or medial maxillary wall
Type A: limited to within the nasal cavity, ethmoid sinus, or medial maxillary wall
 Type B
Type B
 Type C: extension beyond the paranasal sinus
Type C: extension beyond the paranasal sinus
77.2.14 Sinonasal Sarcoidosis
 Stage 1: limited reversible involvement
Stage 1: limited reversible involvement
 Stage 2: moderate disease involvement or limited single sinus involvement
Stage 2: moderate disease involvement or limited single sinus involvement
 Stage 3: irreversible disease causing synechiae, stenosis, and cartilage destruction
Stage 3: irreversible disease causing synechiae, stenosis, and cartilage destruction
| Grading | State of mucosa |
| 0 | No oedema |
| 1–3 | Mucosal oedema (mild/moderate/severe) |
| 4–6 | Polypoid oedema (mild/moderate/severe) |
| 7–9 | Frank polyps (mild/moderate/severe) |
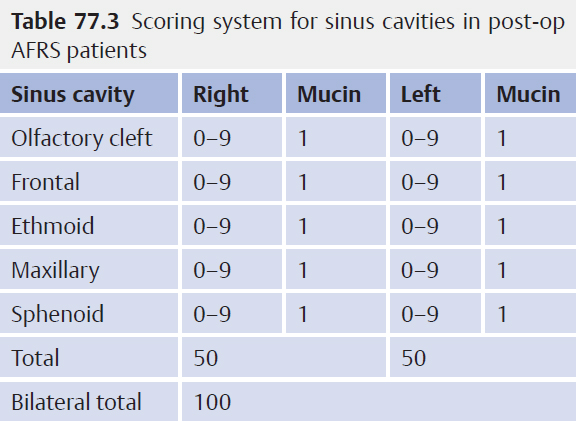
77.2.15 Staging System for Sinus Cavities in Post-op AFRS Patients
• See Tables 77.2 and 77.3
77.3 Head and Neck
77.3.1 Neck Trauma
• Zone I: superior cricoid to inferior thoracic inlet
• Zone II: superior angle of mandible to inferior cricoid
• Zone III: superior skull base to inferior angle of mandible
77.3.2 Apnoea/Hypopnea Index
• 5 to 20: mild
• 20 to 40: moderate
• >40: severe
77.3.3 Posterior Glottic Stenosis
• Type I: interarytenoid adhesion
• Type II: posterior commissure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


