Fig. 255 Intact soft meatal wall (Dagget 1949) in the conservative radical operation, using a retroauricular approach with removal of the bridge but preservation of the intact soft meatal wall in continuity with the drum, in a case of an attic cholesteatoma and intact ossicular chain. The cholesteatoma membrane is removed and the neck of the cholesteatoma is pushed through Shrapnell’s membrane into the ear canal (arrow) in the hope that it will grow together and close the perforation
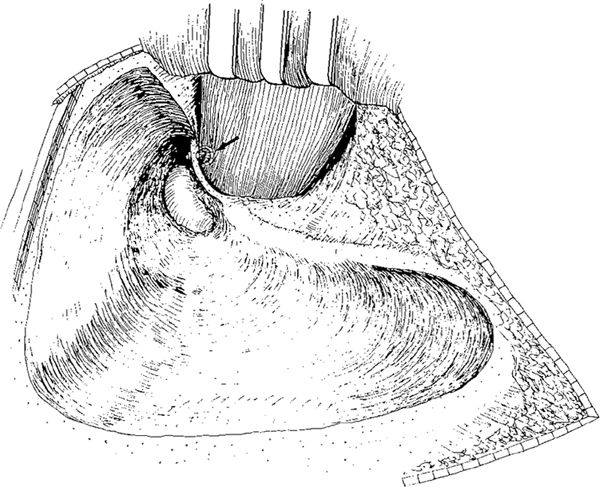
Fig. 256 Conservative radical operation with removal of the posterior bony ear canal wall, but with preservation of an intact bridge in a case of attic cholesteatoma. The incus is removed, the malleus head resected, and the cholesteatoma membrane removed. The neck of the cholesteatoma is pushed through the perforation into the ear canal (arrow). The soft meatal wall is intact
The intact ear canal is filled with gauze, pushing the remaining drum gently onto the medial wall of the tympanic cavity (Dagget 1949). A strip of rubber glove or oiled silk is then placed behind the drum perforation up into the attic region, temporarily closing the ear canal from the cavity (Fig. 257). Blood is allowed to fill the cavity behind the rubber strip, which is brought out of the wound, and the postantral wound is primary closed. The rubber strip is removed after 36 hours, and the ear canal package is removed after six days. For the first ten days, the meatus appears to be somewhat narrowed, but then organization of the blood clot is followed by contraction, and the ear canal opens up as “though it was pulled back from behind.” Within three months, this pulling back of the meatal soft tissue is so obvious that it is often difficult at first glance to be sure that a meatal flap was not cut and laid back into the cavity during the original operation (Dagget 1949).
These attempts to preserve the intact soft ear canal wall and to reconstruct its defect, including the drum perforation, before the tympanoplasty era, are extremely interesting, as is the obliteration of the cavity with blood clot and recognition of the retraction of the soft ear canal wall with the gradual formation of a cavity.
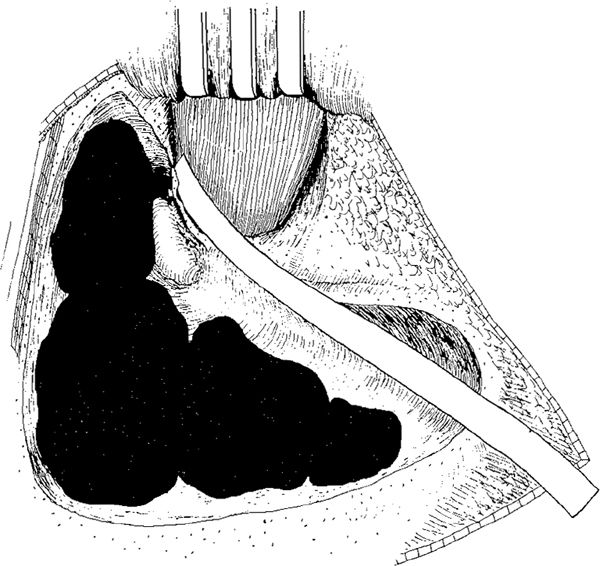
Fig. 257 After removal of the cholesteatoma, a strip of rubber glove is placed behind Shrapnell’s membrane, and the cavity is filled with blood. The rubber glove strip is brought out of the wound, which is given a primary closure before the strip removed after 36 hours (Dagget 1949)
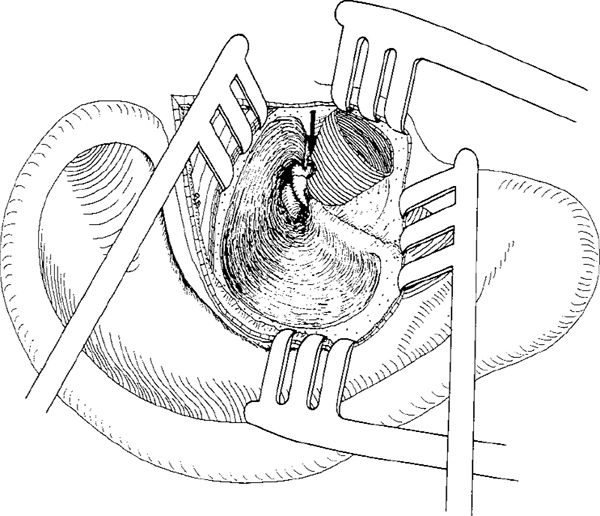
Fig. 258 Preservation of the intact ear canal skin in the endaural approach (Andrew 1956). An endaural conservative radical operation, with removal of the bridge and preservation of the intact ear canal skin tube. A Shambaugh incision is performed, and the lateral circular incision of the ear canal skin is continued all the way around the meatus. The ear canal skin is elevated as a tube together with the ear drum. A conservative radical operation is performed, the cholesteatoma membrane removed, and the neck of the cholesteatoma is pushed through the perforation in the Shrapnell’s membrane into the ear canal (arrow).
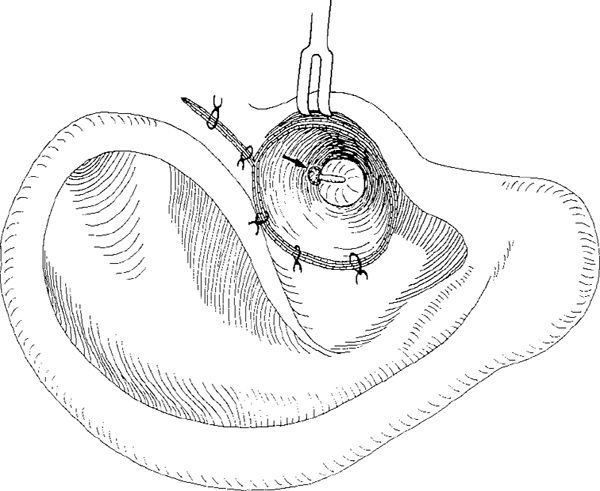
Fig. 259 After the cavity has been filled with blood, the ear canal is closed with sutures. The inverted neck of the cholesteatoma membrane is seen in the ear canal (arrow). The Shrapnell’s membrane perforation is intended to close spontaneously.
Preservation of the soft ear canal was also performed in the endaural Shambaugh incision by Andrew (1956). After the Shambaugh incision (Volume 1, Figs. 50, 52) and a lateral circumferential incision all the way around the ear canal (Fig. 258), an endaural conservative radical operation is performed, with removal of the posterior bony ear canal and the bridge. The intact ear canal skin is carefully elevated and maintained intact. The attic cholesteatoma is debulked, and the matrix is elevated from the intact ossicular chain. The neck of the cholesteatoma at Shrapnell’s membrane is inverted into the ear canal (Fig. 258). The ear canal skin is closed with sutures, and the cavity behind the ear canal is fills with blood (Fig. 259). The cholesteatoma perforation in the Shrapnell’s membrane region is supposed to close spontaneously. Andrew selected cases with attic cholesteatoma and an intact ossicular chain for this type of operation, with preservation of good hearing. Andrew (1956) followed nine patients for more than one year, achieving good results.
During the tympanoplasty era, Pou (1960) and Collins (1964) performed an identical operation to Andrews, but the perforation was closed with a skin, vein, or fascial graft, and the possibly defective soft ear canal wall was reconstructed.
After the introduction of tympanoplasty techniques by Wullstein and Zöllner in the mid-1950s, improvement of hearing and control of cholesteatoma was possible (Wullstein 1956, Zöllner 1957, 1959). In the late 1950s, Rambo (1957) and Guilford (1960) introduced obliteration techniques to avoid a cavity and improve hearing.
Preservation of the Bony Ear Canal Wall
In 1931, Morrisset Smith published his “new radical operation,” which was probably the first attempt to preserve the intact bony ear canal wall in surgery for chronic otitis media (Smith 1931). The idea was to create a mastoid cavity that would be filled with granulation tissue and a tympanic cavity, also filled with granulation tissue and covered with the ear canal epithelium. Using the retroauricular approach, a complete cortical mastoidectomy is performed, with preservation of a thin, but intact, bony ear canal wall. The posterior ear canal wall skin is then elevated and pushed anteriorly. Through the ear canal, using a combined approach, the ear drum with the fibrous annulus, and the malleus and incus are removed. All the middle ear mucosa and the Eustachian tube mucosa are removed with a curette. This is accomplished without removing the bony posterior ear canal wall (Fig. 260) that separates the middle ear from the mastoid cavity, allowing the mastoid cavity to fill with healthy granulation tissue, as in simple mastoidectomy after acute mastoiditis. The tympanic cavity should also fill with healthy granulation tissue, and epithelialization of the granulations should take place from the ear canal skin. Smith (1931) never published any results of this operation.
An intact canal wall mastoidectomy with an enlarged ear canal was described and used by Brunar in 1957 (Brunar 1958, 1959). Through a retroauricular approach, the posterior ear canal skin is elevated, and the bony ear canal is widened by about 2 mm by transmeatal drilling of the posterior bony wall. An intact canal wall atticoantrotomy and mastoidectomy is performed, leaving an intact bony ear canal wall that is 1 mm thick and posteriorly displaced by about 2 mm, because of the initial widening of the ear canal (Fig. 261). In this technique, Brunar used Wullstein’s inspection hole through the facial recess in order to inspect the stapes. Wullstein (1956) called this lower inspection opening (Fig. 262) “Untere Paukenkontrolle,” the term originally used in fenestration operations. Later, this hole was used to inspect the incudostapedial joint and the stapes in myringostapediopexy. Brunar reconstructed the defect in the ear canal with full-thickness skin grafts, and hoped for repneumatization of the cavity.
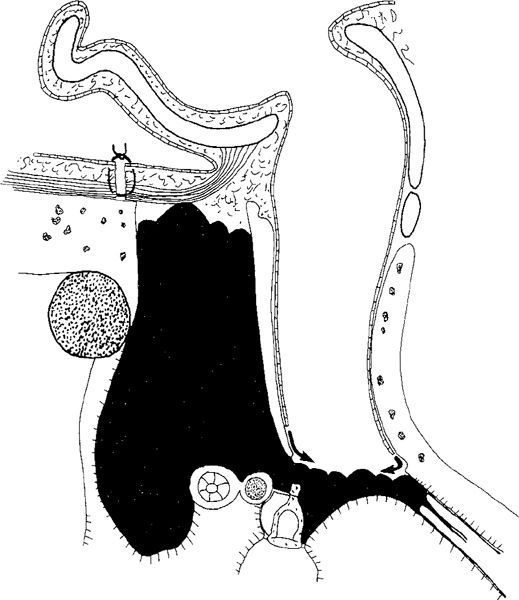
Fig. 260 Preservation of the intact bony ear canal wall (Smith 1931). Side view of the “new radical operation” with preservation of an intact bony ear canal wall. The ear drum and the fibrous annulus, malleus, and incus are removed. The mastoid cavity and the tympanic cavity are filled with blood, and the intention is that healthy granulation tissue should fill the mastoid cavity and the tympanic cavity. The granulation tissue in the mastoid cavity will be epithelialized from the ear canal (arrows). The Eustachian tube is intended to remain closed.
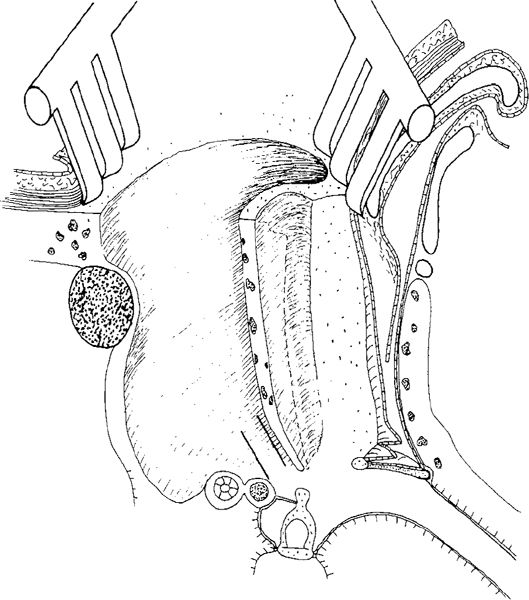
Fig. 261 Preservation of a posteriorly displaced intact bony ear canal wall (Brunar 1959). Perspective side view of Brunar’s intact canal wall mastoidectomy. After elevation of the posterior canal wall skin, the ear canal is enlarged by intrameatal drilling for about 2 mm. The dotted line indicates the original position of the bony ear canal wall. An intact wall mastoidectomy is performed. The bony ear canal wall is thinned to 1 mm thickness. The Wullstein lower inspection opening is carried out, indicated here by the two solid lines in the facial recess.
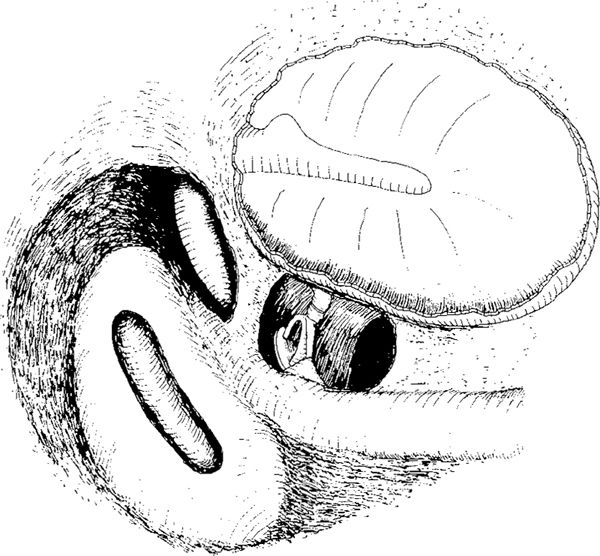
Fig. 262 The original Wullstein lower inspection opening through the facial recess, in a situation with fenestration of the lateral semicircular canal. The stapes and the incudostapedial joint as well as the round window, are visible through the hole. The facial nerve is skeletonized, and a broad posterior buttress has been left in place, partly hiding the inferior edge of the short process of the incus. Fenestration is performed on the lateral semicircular canal.
Further Development of the Posterior Atticoantrotomy
In the facialchorda angle, i. e., the facial recess, new surgical techniques for facial nerve decompression were developed during the 1950s (Lewis 1956, Wullstein 1958, Kettel 1959). These authors all described techniques in which the facial nerve is exposed by a simple mastoidectomy, with removal of the bone within the facial recess.
Applying the posterior atticotympanotomy, Jansen was the first, in 1957, to preserve the posterior bony ear canal wall in cholesteatoma surgery (Jansen 1958, Jansen 1962). In his first English publication, Jansen (1963) reported that, in the majority of surgical cases with chronic middle ear disease, using meticulous drilling and thinning it was possible to preserve the posterior bony ear canal wall. The thinning of its medial part around the ossicles was reported to achieve exposure of the lateral attic. To expose the posterior tympanum, Jansen elaborated and widened the original Wullstein lower inspection opening, especially towards the hypotympanum. He originally called this procedure posterior hypotympanotomy. The bone to be removed was termed by Jako (1966) the antrum threshold. The term facial recess, defining the space between the facial nerve canal and the chorda tympani, was popularized by Sheehy (1965, 1970), and this surgical term became widely accepted in the classic intact canal wall mastoidectomy technique.
In the USA, the Otological Medical Group (Los Angeles) started performing intact canal wall technique in 1958, and published their methods (House and Sheehy 1963, Sheehy 1965) and their first results (Sheehy and Patterson 1967). Myers and Schlosser (1960), Austin and Shea (1961), and Corgill and Martinez (1963) have also independently performed intact canal wall mastoidectomy operations.
During the 1960s and early 1970s, the intact canal wall mastoidectomy became a very popular method and was used in many centers, but the late results soon showed some disadvantages of the technique. There was a high percentage of residual cholesteatoma in the tympanic sinus, which could not be properly removed through the extended posterior atticotympanotomy. Also, a high frequency of residual cholesteatoma in the anterior attic was found, demonstrating that exposure of the anterior attic is often not sufficient. In addition, there was a high frequency of recurrent cholesteatoma, manifesting initially as retraction into the posterior tympanum, around the intact bony wall and into the attic and aditus ad antrum (Smyth et al. 1967, 1971, Smyth 1976). Many surgeons abandoned the intact canal wall technique and went back to canal wall– down techniques, while others performed canal wall– up mastoidectomy in two stages, thus allowing a “second-look” procedure to check that no cholesteatoma remained behind the intact ear drum or intact posterior ear canal wall.
Surgical Technique
Incision
Any retroauricular skin incision can be used, and these are described in Volume 1, Chapter 4. The retroauricular fold incision or posterosuperior incision (Portmann 1979) (Volume 1, Figs. 123, 124) is placed at the most anterior point in the postauricular fold. If these incisions are used, then the subcutis–periosteum incision is placed along the entrance of the bony ear canal; but then an additional subcutis–periosteum incision has to be performed along the lower edge of the temporalis muscle. The subcutis and periosteum are elevated and held with selfretaining retractors. In Portmann’s (1979) skin incision, as well as the subcutis–periosteum incision around the entire bony canal entrance, two additional, posteriorly directed incisions are performed, one superiorly and one inferiorly, allowing further elevation of a posterior-based flap (Volume 1, Fig. 32), thus exposing the cortex of the mastoid process.
Using the retroauricular flap incision 1–5 cm behind the retroauricular fold (Volume 1, pp. 55– 59), the subcutis–periosteum incision is performed at the same level as the skin incision, and the flap is elevated anteriorly, including either subcutaneous tissue and periosteum together with the skin, or separately, creating an anteriorly-based subcutis–muscle–periosteum flap. This flap can be useful in obliteration and reconstruction of the ear canal if it becomes clear that a canal wall–up procedure cannot be performed. The present author therefore prefers the retroauricular flap incision, with creation of an anteriorly based subcutis–muscle–periosteum flap.
Ear Canal Skin Elevation
The goals of ear canal skin elevation are to expose only as much bone as necessary, to preserve all attached skin as intact flaps, and to protect the flaps during the surgery. This can be achieved in several ways, as described in Volume 1, Chapter 4, i. e., performing a medially-placed circumferential incision between the 12-o’clock and 6-o’clock positions, and two radial incisions at the 12-o’clock and 6-o’clock positions, running laterally. In this way, a large laterally based skin flap is pushed anteriorly toward the anterior wall, and held in place and protected with a special House–Sheehy retractor (Volume 1, Fig. 107). The circumferential incision can be placed more laterally in the ear canal, with the result that the medial tympanomeatal flap is larger and the lateral flap shorter. The lateral flap can be turned posteriorly outward, retracted, and held in place with a protective selfretaining retractor (Fig. 263) or a strip of gauze (Portmann 1979) (Volume 1, Figs. 130, 131).
Sheehy (1970b) used his own “posterior vascular strip technique” (Volume 1, Figs. 148–157), with elevation and removal of the ear canal skin together with the drum remnant epithelium (Volume 1, Figs. 148–156). The elevated posterior canal skin (the vascular strip) is turned outward and held in place with a protecting retractor.
The posterior canal skin flap can be turned around the posterior surface of the auricle and fixed there with a surgical stay (Volume 1, Fig. 155).
The present author does not feel that ear canal skin removal is necessary, except in a few cases with very pronounced protrusion of the anterior ear canal wall.
Mastoidectomy
The principles of mastoidectomy are basically the same as those described in Chapter 4, but in the intact canal wall technique, attention is focused from the very beginning on thinning the posterior ear canal wall. In the present Chapter, therefore, the work around the ear canal is described in detail; the other phases of mastoidectomy are described in Chapter 4.
After exposure of the entire mastoid plane, drilling commences behind the posterior edge of the ear canal, using a large cutting burr (Fig. 263). Drilling of the cortical bone is continued along the terminal line (Fig. 264). Bone removal and exenteration of the air cells is gradually extended in an inferior and medial direction toward Körner’s septum, depending on the pneumatization and pathology of the mastoid process (Fig. 265).
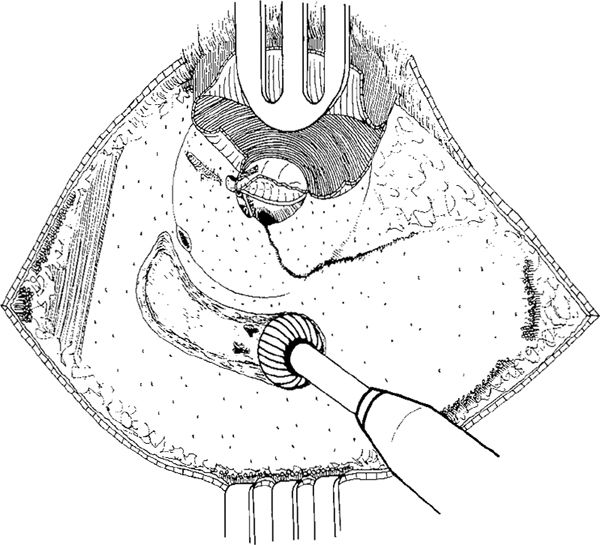
Fig. 263 Intact canal wall mastoidectomy. After the retroauricular incision and elevation of a subcutis–periosteum flap, a lateral circumferential canal skin incision and two radial skin incisions, at the 12-o’clock and 6-o’clock positions are performed. The posterior ear canal skin flap is elevated outward and protected by a selfretaining retractor. A large area of the mastoid cortex is exposed, up to the temporalis muscle. Drilling is started with a large cutting burr, initially making a groove along the posterior edge of the bony ear canal
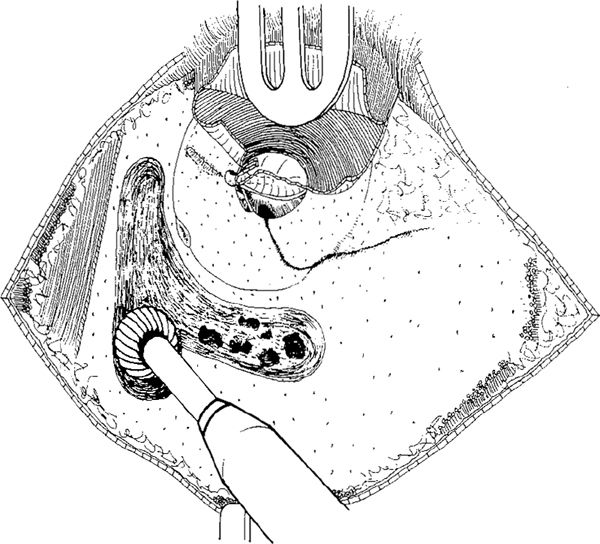
Fig. 264 The drilling is continued along the middle fossa dura plate, and the mastoid cortex is gradually removed
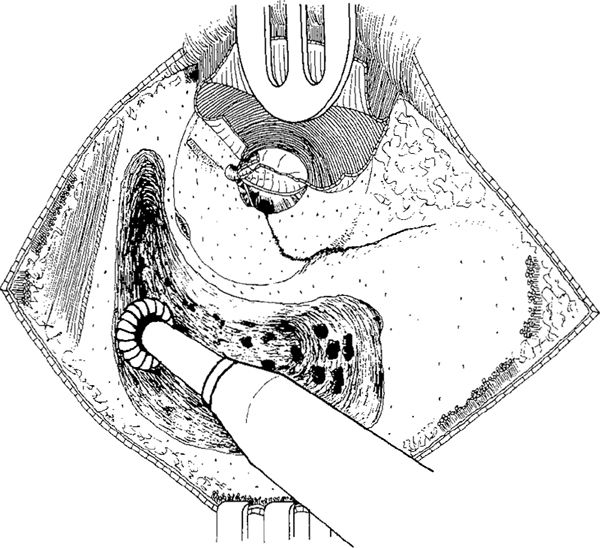
Fig. 265 The cavity is enlarged along the middle fossa dura plate, and the sigmoid sinus and lateral mastoid air cells are exenterated
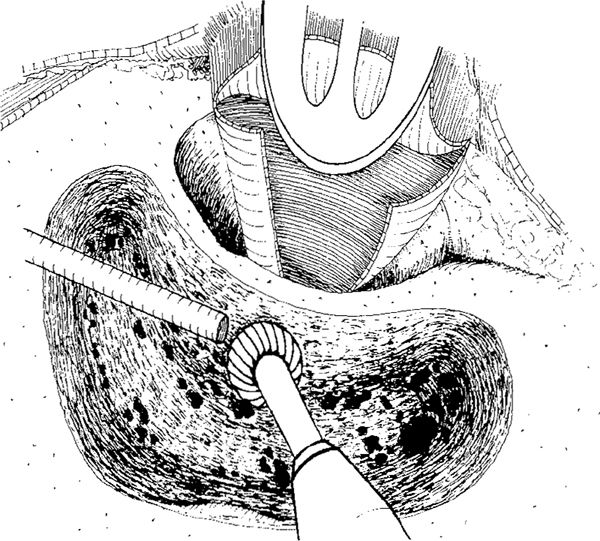
Fig. 266 The posterior side of the ear canal is thinned with a cutting burr. Körner’s septum has not yet been opened
Thinning the Posterior Ear Canal Wall
After exenterating the lateral mastoid air cells down to Körner’s septum, the posterior ear canal wall is thinned. The patient is tilted away from the surgeon, allowing better visualization of the posterior side of the ear canal wall, which is gradually thinned with a cutting burr (Fig. 266).
The cavity is enlarged, the sigmoid sinus is skeletonized, and the antrum is entered after removal of Körner’s septum (Fig. 267) (as illustrated in Chapter 4, Figs. 189–192). The posterior ear canal wall is still too thick for the incus body and the prominence of the lateral semicircular canal anteromedially in the antrum to be identified, and the posterior ear canal wall is therefore further thinned (Fig. 268). The thinning of the ear canal is continued until the prominence of the lateral semicircular canal becomes visible (Figs. 269, 270a). Further drilling of the lateral attic wall and thinning of the ear canal exposes more of the lateral semicircular canal, but the incus body is still not visible (Figs. 271, 270b).
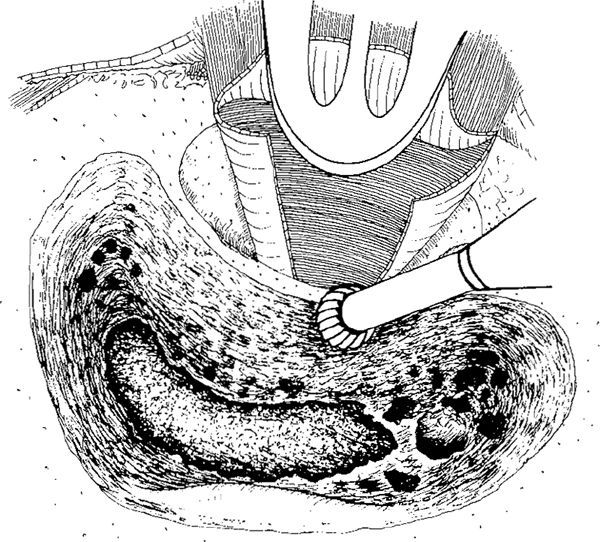
Fig. 267 Körner’s septum has been removed and the antrum has been opened, as has the aditus ad antrum. Posteriorly, the cavity is enlarged and the sigmoid sinus skeletonized
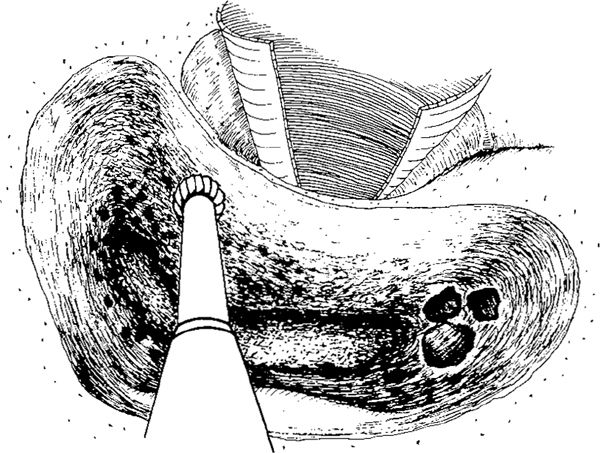
Fig. 268 Further thinning of the posterior ear canal wal is taking place
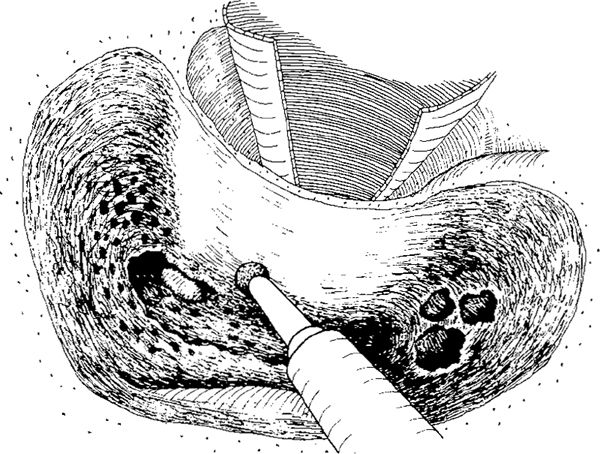
Fig. 269 Using a diamond burr, the inner ear canal is thinned medially, exposing the lateral semicircular canal. The malleus head and incus body are still covered with a bony overhang
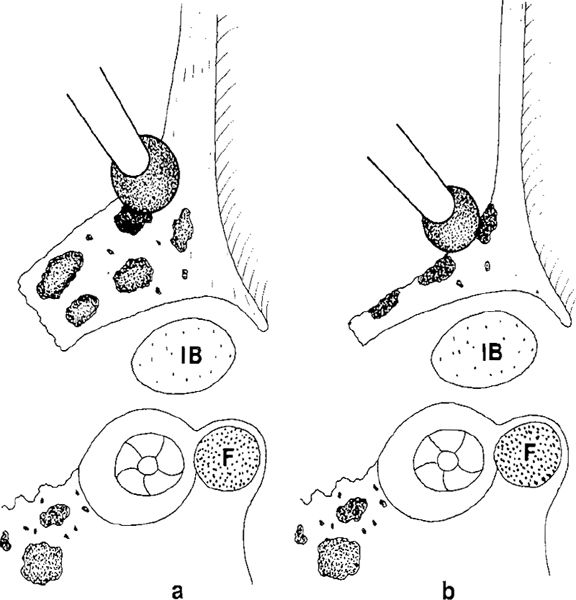
Fig. 270 Side view of the posterior ear canal wall with its bony overhang. F: facial nerve.
a There is still a thick bony overhang covering the incus body (IB) and part of the lateral semicircular canal.
b The bony ear canal wall is maximally thinned, as is the bony overhang covering the incus body
Lateral Atticotympanotomy
Further careful drilling with a small diamond burr and further thinning of the ear canal is required to expose the lateral aspect of the incus body (Fig. 272). This procedure has been called superior tympanotomy (Smyth 1980); the present author prefers the term lateral atticotympanotomy, which is more precise, firstly to avoid confusion with a similar term for elevation of the superior tympanomeatal flap, earlier called superior tympanotomy by Wullstein (1968). The procedure itself involves the thinning of the lateral attic wall in order to enter the tympanic cavity through the lateral attic, so that it is best described as lateral atticotympanotomy. The last overhang of the lateral attic wall covering the incus body can be carefully fractured out using a House curette (Fig. 273a). Finally, the posterior and lateral aspects of the malleus and incus body become visible (Figs. 273b, and 274).
To complete the lateral atticotympanotomy, some drilling of the lateral attic wall is required in order to make it thinner so as to survey the lateral attic and enter the tympanic cavity through it. This is performed using a small diamond burr (Figs. 275, 276). Finally, the ear canal is maximally thinned, the lateral attic is exposed (Fig. 277), and the instruments can pass into the tympanic cavity (Fig. 276b). The lateral atticotympanotomy is thus complete. The thinning of the posterior ear canal has to be performed carefully, without perforation of the attic wall. If an intact ossicular chain is found, care must be taken to avoid touching the incus body and the malleus head with the burr. Thinning is therefore a difficult procedure, and requires much practice on temporal bones. Thinning of the ear canal wall has to be extended to the anterior attic and the posterior attic along the short process of the incus, at which point a small bony bridge between the ear canal wall and the horizontal semicircular canal—the posterior buttress—is left intact. Inferior to the buttress, the posterior atticotympanotomy is performed.
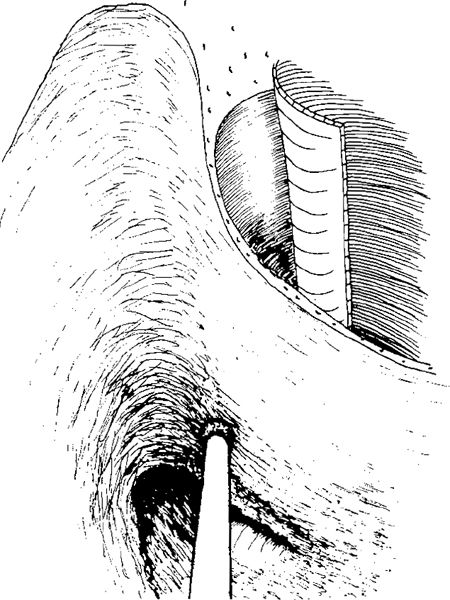
Fig. 271 Further drilling of the bony overhang covering the malleus head
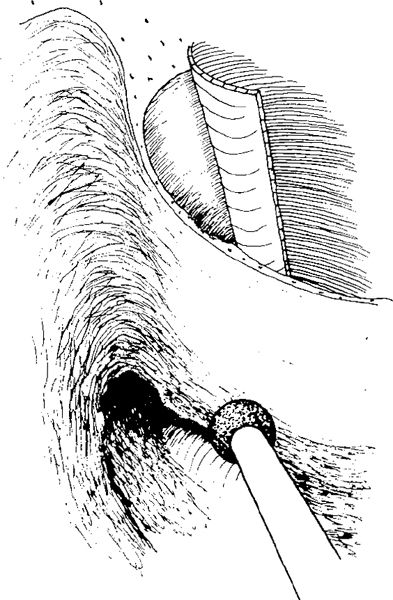
Fig. 272 Lateral atticotympanotomy, defined as drilling of the lateral attic wall and the bony overhang covering the incus body
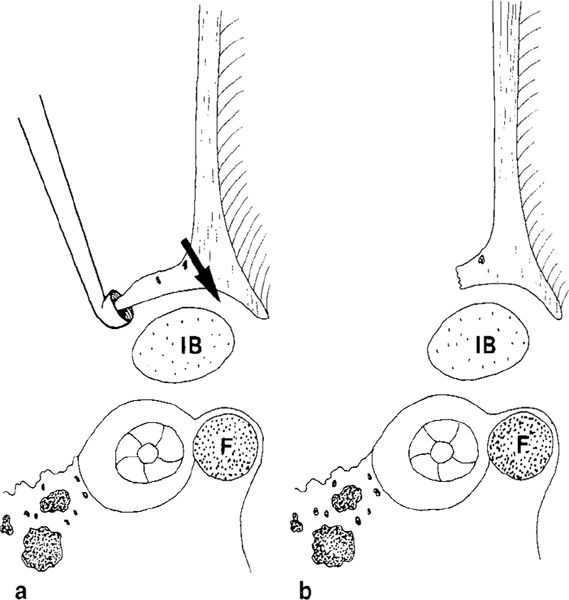
Fig. 273 The lateral atticotympanotomy seen in a side view, with the thinned ear canal wall and the bony overhang blocking the view of the incus. F: facial nerve; IB: incus body.
a The direction of drilling is shown by the arrow. The overhang is removed with a curette.
b There is still a small overhang covering the incus
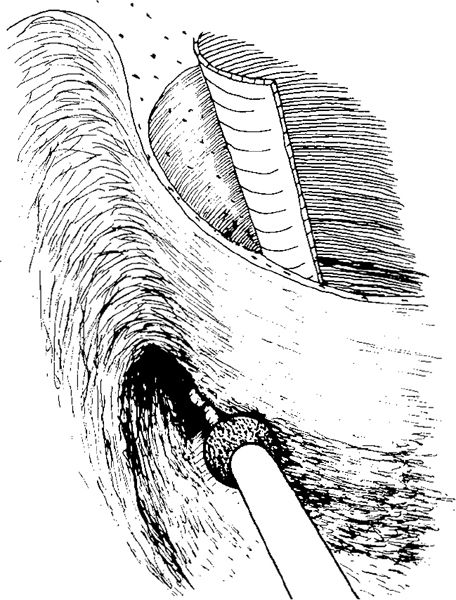
Fig. 274 With further drilling of the ear canal, the incus body and the malleus head are further exposed
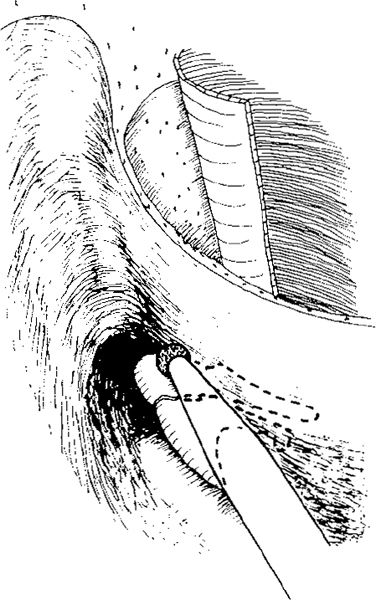
Fig. 275 Careful drilling of the bone with a small diamond burr, resulting in extreme thinning of the lateral attic wall, completing the lateral atticotympanotomy
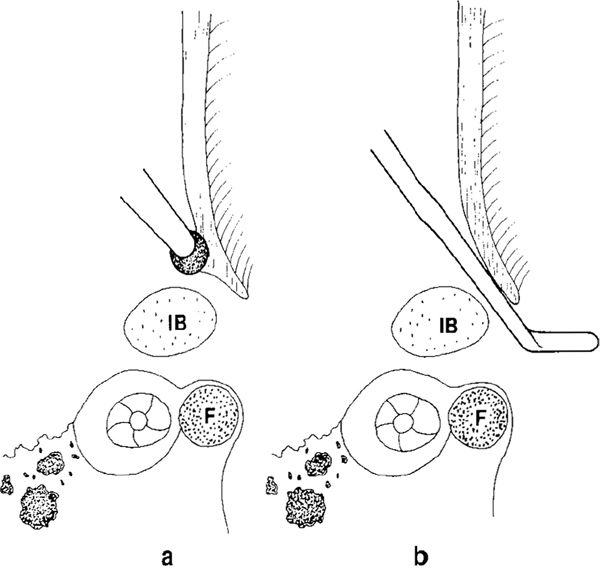
Fig. 276 Side view of the lateral attic wall. F: facial nerve; IB: incus body.
a The last overhang of the lateral attic wall is drilled away with a diamond burr.
b A good communication is produced between the lateral attic and the tympanic cavity by extreme thinning of the lateral wall
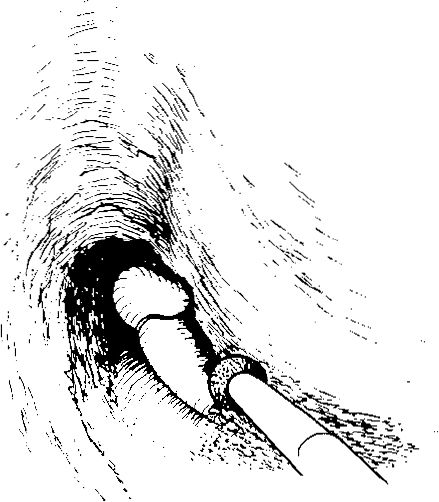
Fig. 277 Final thinning of the posterior aspect of the lateral attic wall and the posterior buttress, defined as the bony connection between the posterior ear canal wall and the lateral semicircular canal at the level of the incudal fossa
Posterior Atticotympanotomy
The author prefers the term atticotympanotomy instead of Jansen’s term posterior tympanotomy, since this avoids confusion with posterior tympanotomy when referring to elevation of a posterior tympanomeatal flap. The term posterior (transmastoid) atticotympanotomy, already used by Farrior (1968, 1969), is also more logical, since the procedure describes the establishment of a connection between the posterior attic and the posterior tympanum. Farrior (1968) uses a similar term, anterior atticotympanotomy, to describe the procedure in intact canal wall mastoidectomy of connecting the anterior attic with the anterior tympanum, including the tympanic orifice of the Eustachian tube.
The drilling technique in posterior atticotympanotomy can be performed along two routes: 1) the lateral route, with initial thinning of the bony ear canal wall lateroinferior to the buttress and the short process of the incus (Fig. 278); and 2) the medial route, with initial drilling of the bone medial to the incudal fossa at the same level as the lateral semicircular canal. In this way, the facial recess is approached medially close to the facial nerve (Fig. 278).
Morimitsu (1991) distinguished between two types of posterior atticotympanotomy: the classic posterior tympanotomy with drilling lateral to the incus, corresponding to the lateral route and the “posterior” posterior tympanotomy, with drilling posterior to the incus corresponding to the medial route.
1. The lateral route. This is safer with regard to the facial nerve, and the drilling is in fact a continuation of the thinning of the bony ear canal wall (Fig. 279), already performed in the lateral attic wall By drilling laterally in the facial recess just inferior to the incudal fossa, no damage to the chorda will occur, because the chorda at this level is located outside the chordal canal, and runs from the chordal canal toward the long process of the incus (Fig. 280a). By continued thinning of the ear canal in the same direction, an opening to the posterior tympanum lateral to the pyramidal eminence is achieved (Fig. 280b), providing a view of the lateral part of the stapes and its tendon (Fig. 281). With further inferior extension of the drilling at the level of the chordal eminence, the chorda tympani is exposed, demarcating the lateral limit of the facial recess (Fig. 282). With further drilling toward the hypotympanum along the course of the chorda tympani, the inferior part of the facial recess is opened (Fig. 283). The lateral extension of the inferior part of the facial recess is limited by the chorda, which runs obliquely down toward the facial nerve, making the chordafacial angle smaller (Fig. 284). With gradual drilling of the bone along the facial nerve, the atticotympanotomy opening gradually extends medially. It can now be extended along the facial nerve down to the hypotympanum (Fig. 285) as far as possible, depending on the course of the chorda tympani (Fig. 286).
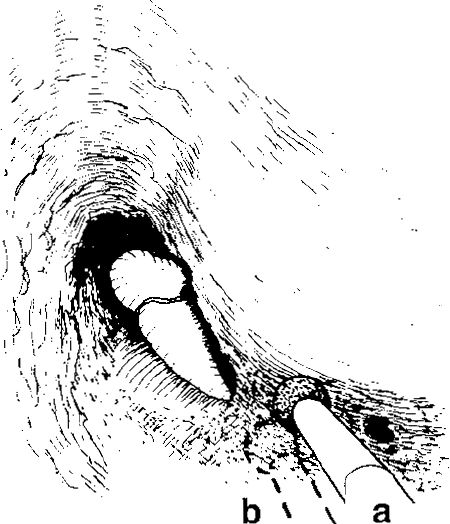
Fig. 278 Posterior atticotympanotomy. Initial drilling with a diamond drill behind the posterior buttress.
a Lateral route to the facial recess, starting the drilling laterally to the incudal fossa and just inferior to the posterior buttress (solid burr).
b Medial route, starting the drilling medially in the facial recess, initially exposing the facial nerve (dashed burr)
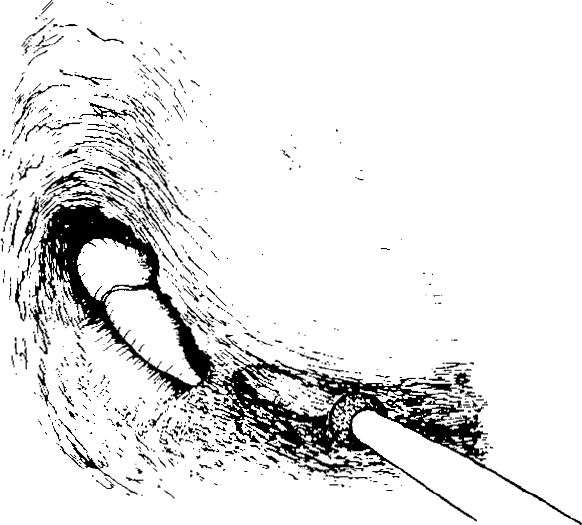
Fig. 279 The lateral route through the facial recess. Behind the broad posterior buttress, a small hole is drilled laterally in the facial recess
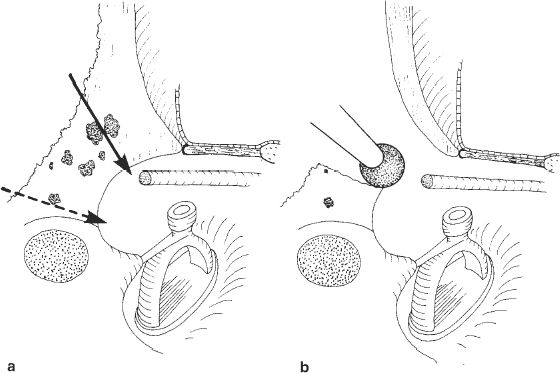
Fig. 280 Side view of the facial recess, illustrating the lateral and medial routes superior to the chordal eminence.
a The lateral route through the facial recess starts with thinning of the posterior ear canal wall (solid arrow) inferior to the buttress. The direction of the medial route through the facial recess is shown by the dashed (dashed arrow).
b The lateral route through the facial recess. A hole is drilled laterally into the facial recess making the posterior ear canal wall thin
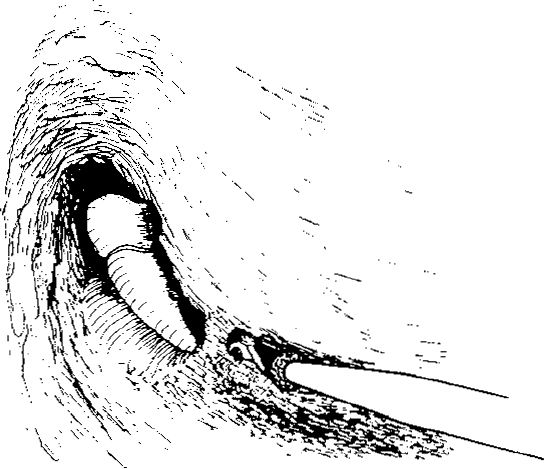
Fig. 281 The lateral route. The facial recess is enlarged by careful drilling along the posterior ear canal in a search for the tympanic chorda. The lateral part of the stapes and the stapedius muscle tendon are visible
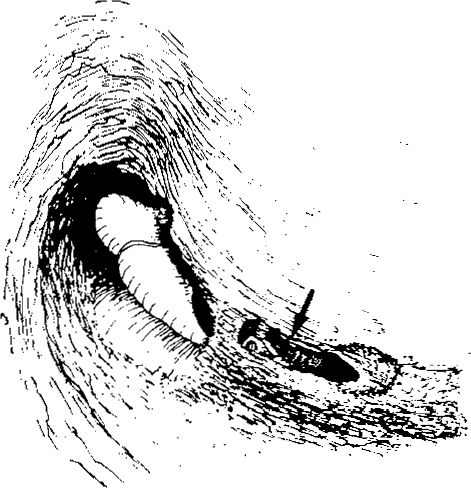
Fig. 282 The chorda tympani is exposed inferior to the incudostapedial joint (arrow)

Fig. 283 Further drilling inferiorly along the course of the chorda tympani enlarges the facial recess and exposes the posterior tympanum, especially the round window niche
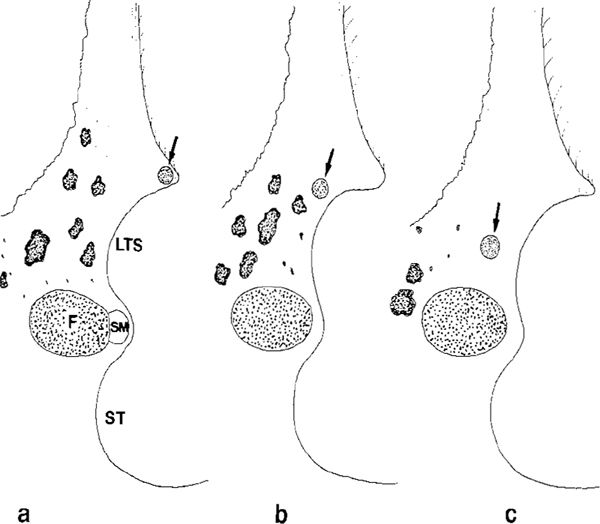
Fig. 284 Side view of the facial recess, illustrating the position of the chorda tympani within the facial recess.
a At the level of the chordal eminence, the chorda is located exactly at the level of the bony annulus. The facial nerve (F) and the stapedius muscle (SM) make the medial border of the facial recess somewhat inferior to the pyramidal eminence. LTS: lateral tympanic sinus; ST: sinus tympani.
b At the level of the round window, the distance from the facial nerve to the chorda tympani is smaller.
c In the hypotympanic region, before its entrance into the facial nerve, the space between the chorda and the lateral surface of the facial nerve is very small. There are usually no air cells at this level
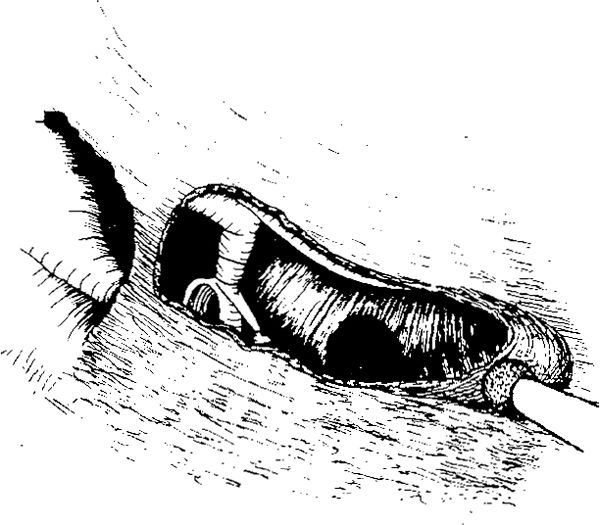
Fig. 285 Further extension of the facial recess inferior to the level of the round window
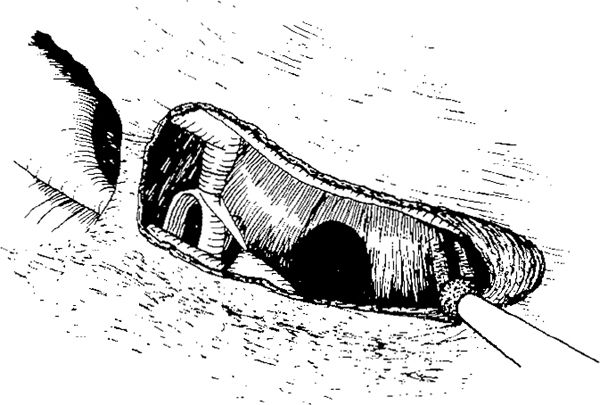
Fig. 286 The inferior limit of the facial recess at the level of the entrance of the chorda tympani into the facial nerve
The facial recess can be further widened by drilling the bone from the lateral aspect of the facial nerve (Fig. 286). If necessary, complete skeletonization of the facial nerve or even decompression of its lateral and anterior aspects can be performed (Fig. 287) at the level of the external genu and along its vertical segment until the junction of the chorda tympani with the facial nerve. Sometimes “barber-poling” of the facial nerve (Nelson 1982) is necessary to gain maximal exposure without damaging any surrounding structures. This term describes the thinning of the bone covering the facial nerve in a barber-pole fashion: 1) the vertical portion of the mastoid segment at the junction of the chorda with the facial nerve is skeletonized and unroofed on its posterior aspect. In this way, the chorda tympani is saved (Fig. 288). 2) At the external genu, the facial nerve is unroofed on its lateral and anterior aspects. Drilling on the posterior aspect of the facial nerve at this level results in fenestration of the posterior or lateral semicircular canal, or both. 3) The horizontal segment is unroofed on its lateral and inferior aspects, but this latter part of the procedure is applied only in decompression of the facial nerve.
Barber-poling the facial nerve is sometimes necessary to enlarge the facial recess in cases of cholesteatoma. In decompression of the facial nerve, the procedure is very useful (Nelson 1983). It is also useful in cases in which there is difficulty in recognizing the extent of the facial recess, and in variations of the course of the facial nerve.
The facial recess is very variable. The bone can be sclerotic without any cells (Fig. 289a) (Sheehy 1970b), and in such cases the drilling is difficult and troublesome. The bone covering the facial nerve can include several air cells, some of them relatively large, and in such cases, by exenterating these air cells, the posterior atticotympanotomy is relatively easy (Fig. 289b). Sometimes the bone within the facial recess is thin because the depth of the lateral tympanic sinus and the facial sinus is large, and a posterior atticotympanotomy can again be relatively easy to perform in such cases (Fig. 289c).
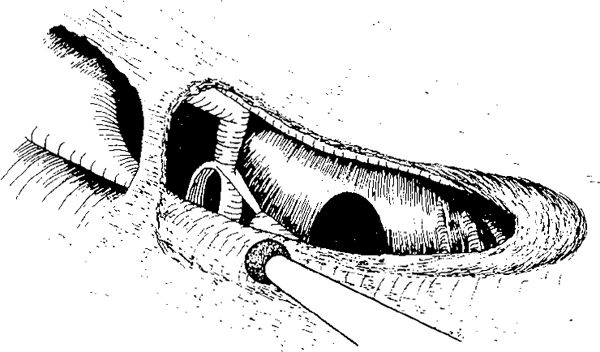
Fig. 287 Further enlargement of the facial recess by removal of the bone along the facial nerve, starting the drilling at the horizontal part of the facial nerve, and continuing toward the external genu and further inferiorly, along the vertical part of the facial nerve
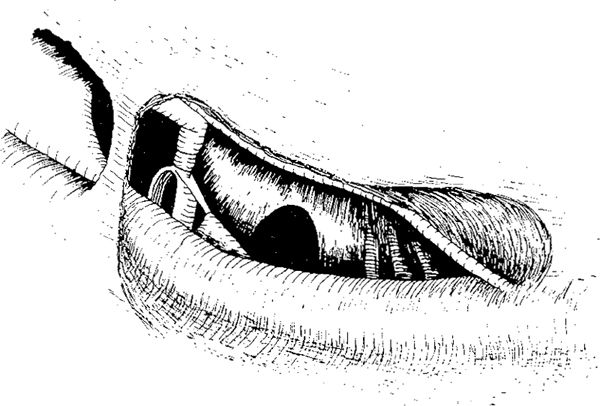
Fig. 288 Barber-poling of the facial nerve in order to decompress the nerve and enlarge the facial recess. At the level of the vertical segment, inferior to the posterior semicircular canal and the level of the entrance of the chorda into the facial nerve, the nerve is skeletonized and decompressed on its posterior aspect
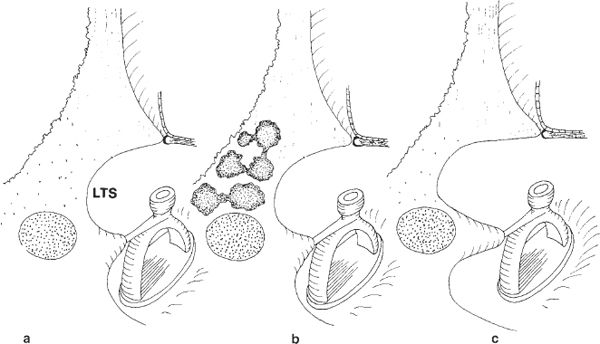
Fig. 289 The variability of the compact bone and air cells within the facial recess.
a The facial recess consists of thick compact bone, without cells.
b The bone forming the facial recess contains relatively large air cells which are easy to follow in order to enter the lateral tympanic sinus (LTS)
c The lateral tympanic sinus is large, and the bone covering the entrance to the facial recess is relatively thin, but compact. Here, too, the drilling through the facial recess is relatively easy
2. The medial route. Skeletonizing the facial nerve (and sometimes even decompressing it) at the external genu is necessary when the facial recess is entered medially close to the facial nerve (Fig. 280). If the medial route to the facial recess is used, then the level of the short process of the incus is initially established. Inferior and medial to the short process of the incus, a small posterior buttress is left, and drilling is continued inferior to this buttress. The facial nerve is located. Through the opening into the facial recess, the stapedial arch is visualized (Figs. 290, 291). With further drilling along the facial nerve, the nerve is skeletonized down to the hypotympanum, and at the same time the facial recess is extended laterally, with the chorda tympani being identified and followed toward its entrance into the facial nerve. Finally, the small residual triangle of bone between the facial nerve and the chorda tympani is drilled away (Fig. 292), completing the posterior atticotympanotomy through the medial route (Fig. 290b).
Removing the Posterior Buttress
Removal of the buttress in cases with an intact ossicular chain is sometimes necessary in order to gain a better view of the horizontal portion of the facial nerve and the posterior tympanic sinus (Fig. 293). Removing the buttress allows more complete and safer removal of the cholesteatoma, and the ossicular chain can still remain intact. A disadvantage of removing the buttress can be the lack of suspension of the short process of the incus, but it has not been demonstrated that this has any major effect on hearing.
Posterior Atticotympanotomy with Absent Incus
If the long process of the incus is defective or missing, or if the incus has been extracted before the posterior tympanotomy, then the thinning of the lateral attic wall starts at the level of the malleus head and continues toward the posterior buttress, which is removed, and the facial recess is then opened, with constant visualization of the horizontal part of the facial nerve being maintained (Fig. 294). The thinning of the lateral attic wall is continued, allowing good enlargement of the tympanic isthmus (Fig. 295). With further drilling in an inferior direction, the stapes is visualized (Fig. 296), and the external genu of the facial nerve eventually becomes visible (Fig. 297). The facial recess is now extended laterally toward the chorda tympani, which is exposed. The access to the tympanic cavity is larger here than in cases with an intact ossicular chain (Fig. 298).
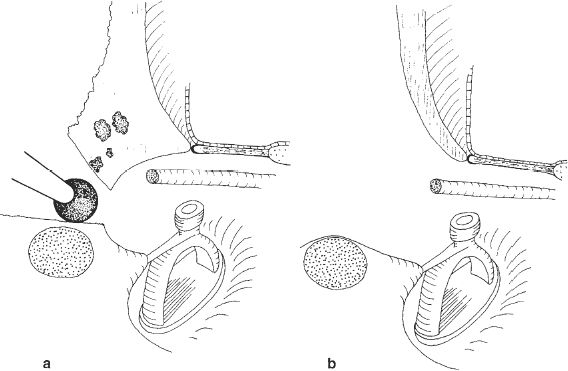
Fig. 290 The medial route through the facial recess
a The drilling is starting close to the posterior buttress and along the facial nerve, skeletonizing it at its external genu, and continuing drilling in inferior direction.
b Final status after completing the medial route, skeletonizing all bone covering the facial nerve and maximal thinning of the posterior ear canal wall
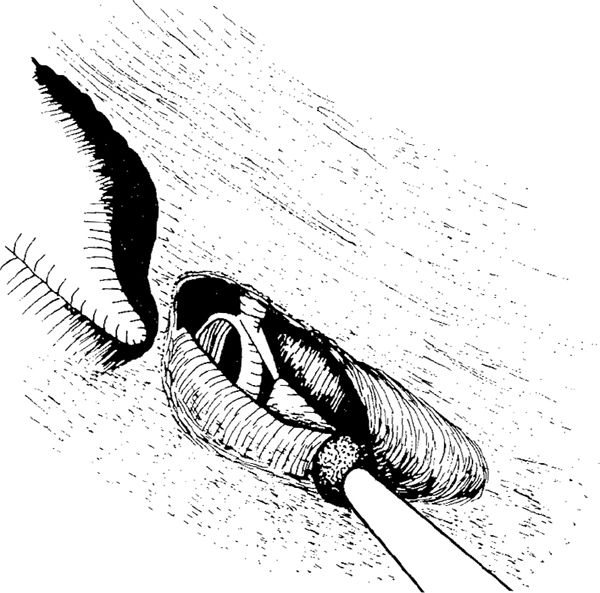
Fig. 291 The medial route through the facial recess. The short process of the incus and fossa incudis are exposed along the small posterior buttress. The drilling is started medially and inferiorly to the short process of the incus, removing the bone localized on the lateral semicircular canal and continuing medially, skeletonizing the external genu of the facial nerve with the pyramidal process. The drilling continues along the nerve in the inferior direction, toward the entrance of the chorda into the facial nerve
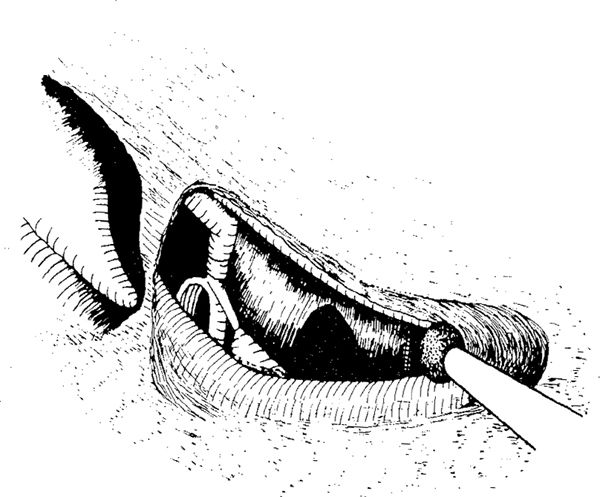
Fig. 292 The drilling along the facial nerve is nearly completed, and the lateral part of the bone has been removed up to the tympanic chorda, which is intact
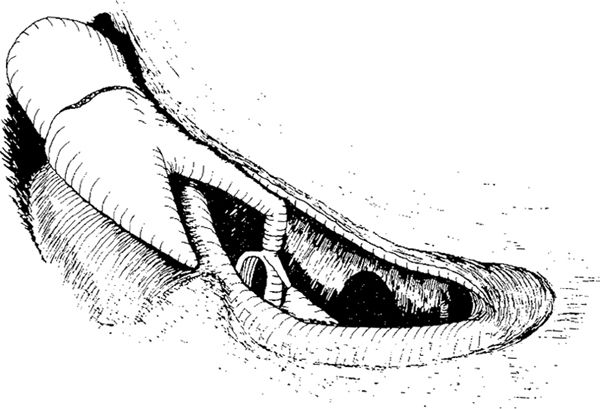
Fig. 293 Removal of the posterior buttress in an intact ossicular chain allows better visualization of the posterior tympanum, especially the horizontal segment of the facial nerve, incus, and stapes
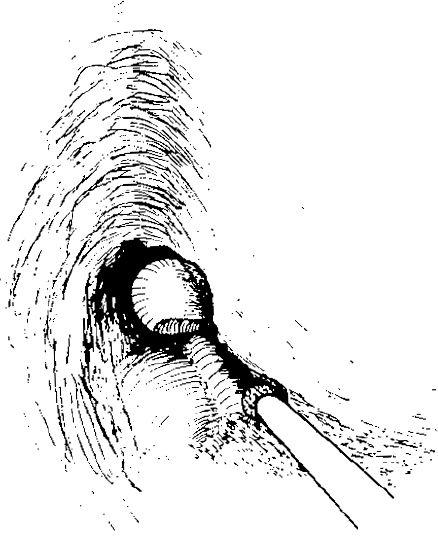
Fig. 294 Posterior atticotympanotomy with an absent incus. The thinning of the lateral attic wall starts at the malleus head and continues toward the posterior buttress
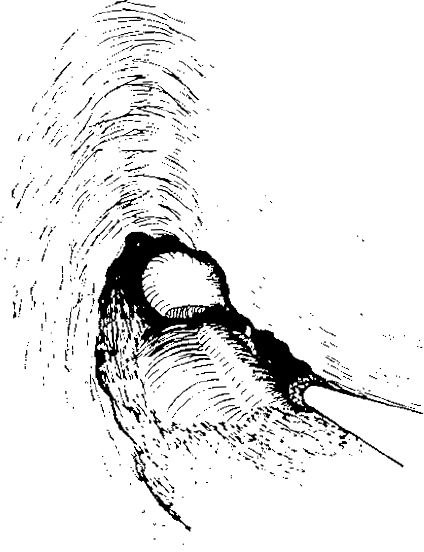
Fig. 295 The isthmus tympani is wide open, and the posterior buttress has been removed
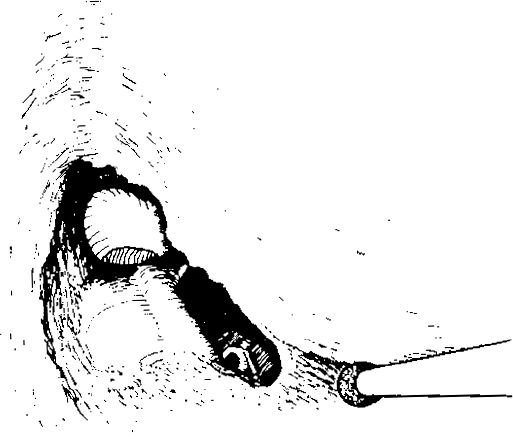
Fig. 296 The posterior atticotympanotomy is extended inferiorly. The stapes is visualized
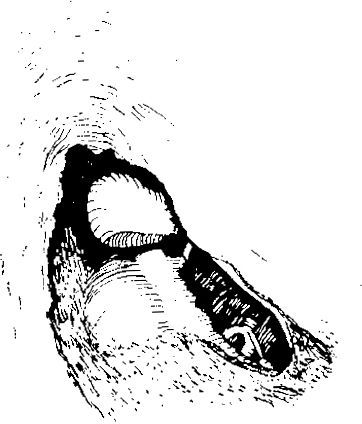
Fig. 297 Further enlargement of the posterior atticotympanotomy exposing the chorda
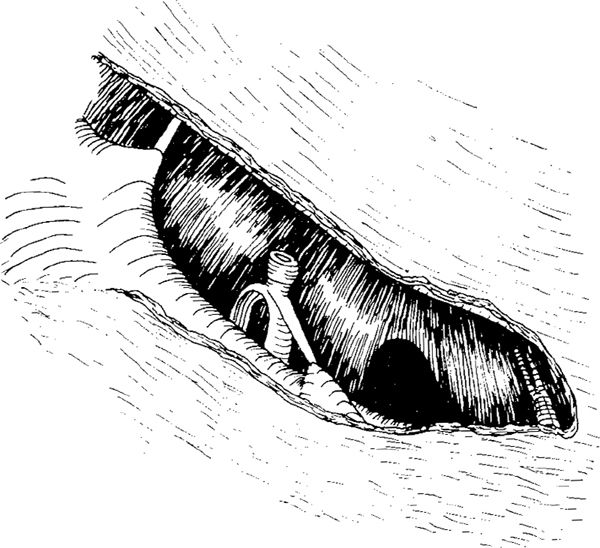
Fig. 298 The posterior atticotympanotomy is nearly complete. The chorda tympani is exposed. Part of hypotympanum and the posterior tympanum are visible
Complications of Posterior Atticotomy
In cases with an intact ossicular chain, drilling in the lateral attic to achieve a thin ear canal wall can be troublesome and dangerous if the burr comes into contact with the intact chain. In order to prevent a high-tone sensorineural hearing loss, a diamond burr is always used in this region, and it is moved gently along the posterior circumference of the lateral attic wall.
During drilling of the facial recess with an intact ossicular chain, the short process of the incus and the fossa incudis needs to be located. The posterior buttress prevents contact between the burr and the incus, but it hampers the view of the tympanic sinus.
The risk of damage to the chorda tympani in the lateral route through the facial recess, or damage to the facial nerve in the medial route, always exists. Practice on many temporal bones is required in order to perform posterior atticotympanotomy properly and quickly. Even the experienced ear surgeon performing posterior atticotympanotomy may occasionally have problems drilling within the facial recess and avoiding exposure of the facial nerve. A dehiscent facial nerve canal in its horizontal course was found in 22% of cases with cholesteatoma, and these dehiscences were either due to bone resorption by the disease or were congenital in origin (Jansen 1963). Even an experienced surgeon who performs posterior atticotympanotomy may injure the facial nerve in a small percentage of cases, but the risk to the facial nerve is much higher when surgery is performed by an inexperienced surgeon.
During lateral drilling, the chorda is relatively frequently damaged, and the drill can touch the incudostapedial joint, causing sensorineural hearing loss.
In order to avoid sensorineural hearing loss and to provide better access to the facial nerve, several surgeons recommend disruption of an intact ossicular chain before drilling (Smyth et al. 1971). The present author (Tos and Lau 1991) has documented that the long-term hearing results in cases with cholesteatoma and a disrupted ossicular chain are poorer than in cases with an intact ossicular chain (Volume 1, Fig. 711), and such disruption is therefore not recommended only in order to perform a posterior atticotympanotomy. In such cases, it is preferable to perform a canal wall–down mastoidectomy and keep the ossicular chain intact.
Extended Posterior Atticotympanotomy, Transmastoid Hypotympanotomy
In cases requiring extensive access to the tympanic cavity, such as glomus tympanicum tumors, glomus jugulare tumors, facial nerve neurinomas, or even cholesteatomas involving the hypotympanum, the chorda tympani is sacrificed and the posterior atticotympanotomy is extended inferiorly and anteriorly. This procedure is called hypotympanotomy by Jansen (1972), but the present author suggests the term transmastoid hypotympanotomy to differentiate it from transmeatal hypotympanotomy (Volume 1, Figs. 192–204).
When a large atticotympanotomy is desired, the chorda can be sacrificed at the chordal eminence (Fig. 299). With the chorda tympani as the guide, the drilling through the facial recess is faster, and a large atticotympanotomy is performed before further removal of the bone along the inferior bony annuhis. The exit of the chorda from the facial nerve is located, and the facial nerve is skeletonized. The drilling can then continue far anteriorly, while the lower prominence of the promontory at the hypotympanic sinus is inspected. The drilling is continued into the tympanic bone (Fig. 300). With further drilling anteriorly, the anterior part of the hypotympanum is reached (Fig. 301), and finally the inferior transmastoid hypotympanotomy is completed (Fig. 302).
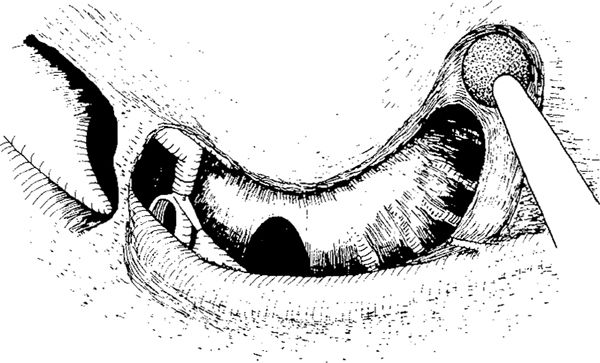
Fig. 299 Transmastoid hypotympanotomy. The chorda is sacrificed, and the posterior atticotympanotomy is extended toward the hypotympanum by drilling the tympanic bone. Posteriorly, the facial nerve is exposed
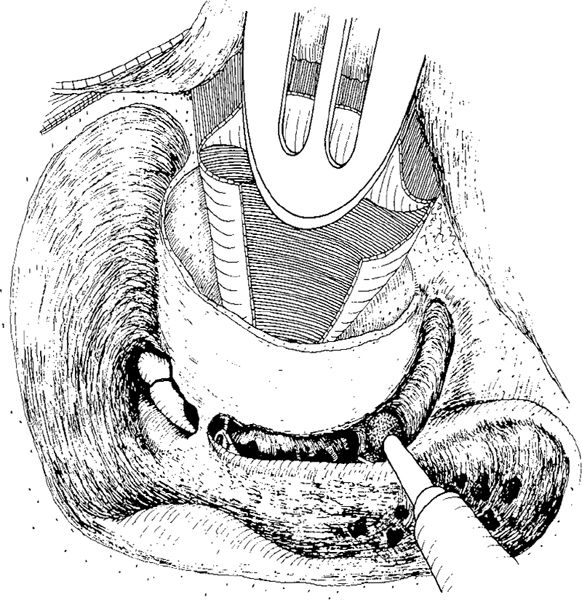
Fig. 300 The inferior bony ear canal wall is preserved and the hypotympanum exposed
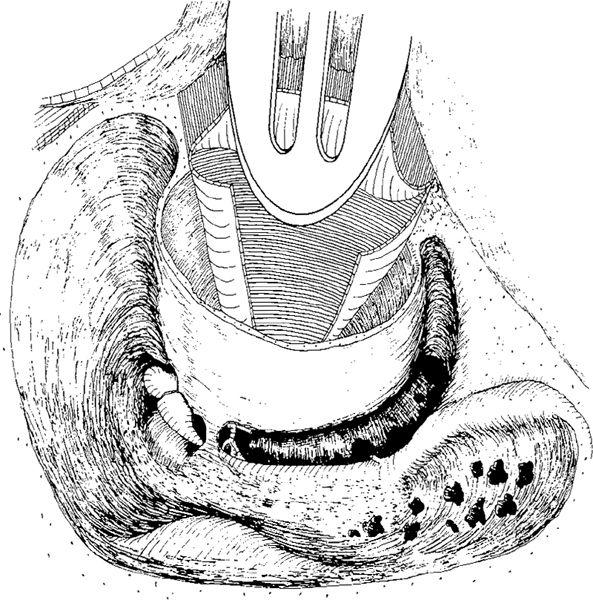
Fig. 301 The drilling is continued far anteriorly. The hypotympanic cells are exposed
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


