A ciliochoroidal effusion is an accumulation of fluid in the potential space between the sclera externally and the choroid and ciliary body internally.1,2,3 The terms edema, effusion, and detachment are often used interchangeably in describing this uveal disorder. In most cases, however, the fluid is located between the fibrous strands that connect the choroid and ciliary body to the sclera and is therefore within the uvea. Thus, edema and effusion are more accurate descriptive terms.
ANATOMIC FEATURES
The suprachoroidal space forms a transition zone and potential space between the choroid and sclera and is composed of fibrous connective tissue. In its physiologic dehydrated state, the suprachoroidal space is approximately 30 µm thick. Because there are virtually no capillaries or lymphatic spaces to drain fluid that collects in this area, the fluid must re-enter the vascular channels in the choroid and exit through the vortex veins,4 the sclera itself,5 or perivascular and perineural spaces in scleral emissary channels.6
Anteriorly, the connective tissue fibers that attach the ciliary body and anterior choroid to the sclera are long and oriented tangentially. A tangential arrangement permits movement of the choroid during accommodation7; however, it also readily allows for the accumulation of fluid. The anatomic arrangement of the fibers anteriorly is analogous to the tangential fibers in the outer plexiform layer in the macula, another location where fluid selectively accumulates.
Posteriorly, the choroid is more firmly connected to the sclera by fibers that are short and oriented perpendicularly between the choroid and sclera.8 The choroid is also firmly anchored to the sclera at the optic disc, at the ampullae of the four vortex veins, and by the ciliary body at the scleral spur. The attachments at the disc and four ampullae account for the characteristic four-lobed structure of a large ciliochoroidal effusion.
The term detachment is often used clinically to describe a ciliochoroidal effusion. Indeed, in some cases, there is an actual cleavage of the fibers that connect the ciliary body and choroid to the sclera. Moses8 showed that a force of about 5 g per cm2 is required to break these connecting fibers. In such cases, the fluid separates the ciliary body and choroid from the sclera and is properly referred to as a detachment.
CLINICAL FEATURES
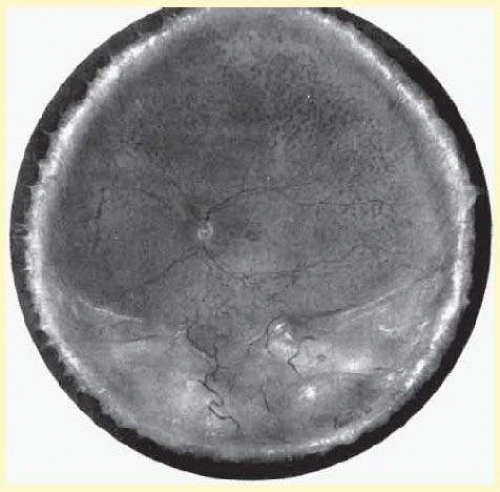
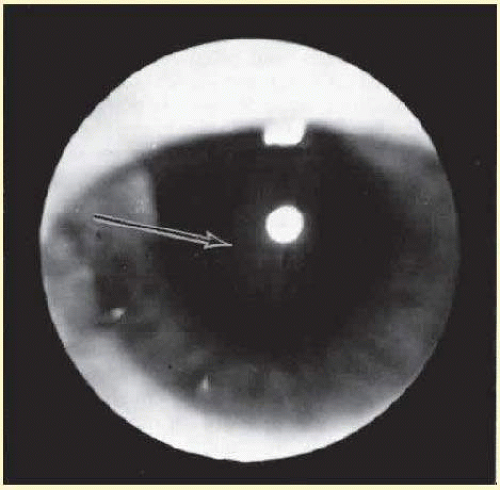
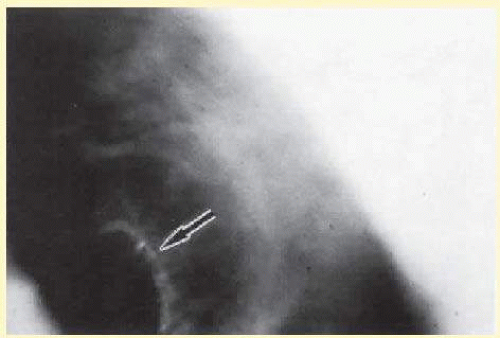
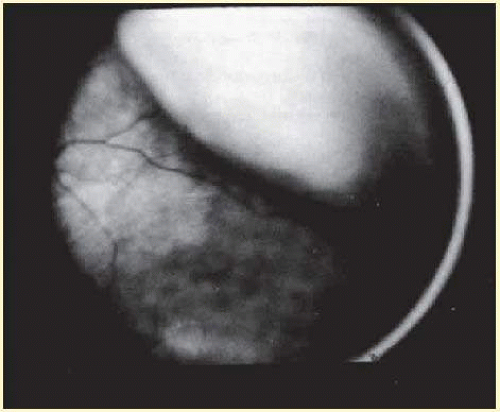
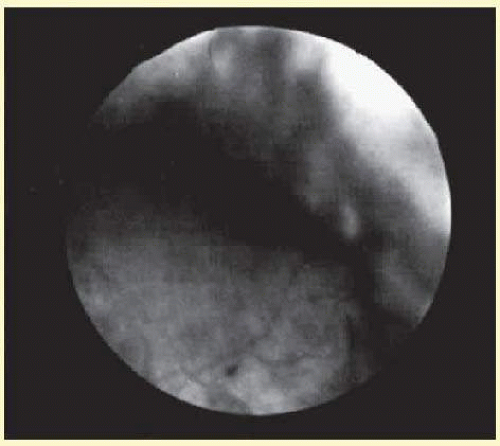
The presence of certain clinical characteristics may assist in the diagnosis of a ciliochoroidal effusion (Table 52.1). One clinical feature is choroidal edema. Choroidal edema may resemble a retinal detachment at first glance; however, darkness of the uvea, lack of tremulousness, and normal retinal vessels indicate a probable uveal process (Fig. 52.1). A shallow anterior chamber and a low intraocular pressure may also suggest the diagnosis. The effusion may extend under the pars plana, allowing visualization of the ora serrata without scleral depression (Fig. 52.2).9 As shown in Figure 52.2, the surface of the elevation is convex and smooth, with a solid appearance and a homogeneous grayish color. Myopia in the presence of anterior displacement of the lens-iris diaphragm may be another diagnostic clue.10,11
TABLE 52-1 Characteristic Clinical Features of a Ciliochoroidal Effusion
Choroidal edema
Shallow anterior chamber
Low intraocular pressure
Visualization of the ora serrata without scleral depression
Nonrhegmatogenous retinal detachment with shifting subretinal fluid
Verhoeff streaks23
Annular, lobular, or flat ophthalmoscopic appearance
Hagen sign28
FIG. 52.1 Painting of the ophthalmoscopic features of uveal effusion syndrome. There is a diffuse pigmentary disturbance in a dot, blot, or linear configuration and an annular ciliochoroidal effusion with secondary inferior retinal detachment.
FIG. 52.2 The ora serrata is visible in the pupillary space due to a ciliochoroidal effusion that developed after retinal detachment surgery in an aphakic eye. The arrow indicates the ora bay. (Courtesy of Retina Service, Wills Eye Hospital, Philadelphia, Pennsylvania.)
Although a ciliochoroidal effusion is usually associated with low intraocular pressure, it may sometimes result in anterior rotation of the ciliary body, secondary angle-closure glaucoma, and elevated intraocular pressure in some cases.12,13,14,15,16,17,18,19,20,21 A ciliochoroidal effusion presenting as secondary angle-closure glaucoma has been reported in several patients with AIDS.16,17,18,19 The etiologic and pathophysiologic mechanisms of ciliochoroidal effusion formation in HIV-positive patients have not been elucidated.
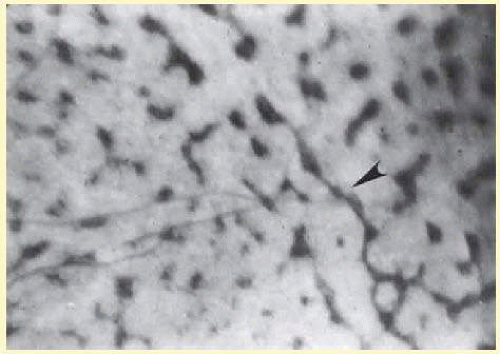
In a chronic ciliochoroidal effusion, breakdown of the blood-ocular barrier at the level of the retinal pigment epithelium (RPE) may occur, leading to a nonrhegmatogenous retinal detachment characterized by shifting subretinal fluid. The protein content of this fluid may be more than three times greater than that of plasma, causing it to shift to a dependent position as the eye and head move.22 The amount of subretinal fluid increases as the chronicity of the effusion increases. A total retinal detachment may result, making the detection of shifting fluid difficult. Linear areas of RPE hypertrophy and hyperplasia may also be observed in chronic effusions (Fig. 52.3). These streaks, noted by Verhoeff,23 suggest a chronic and recurrent process.
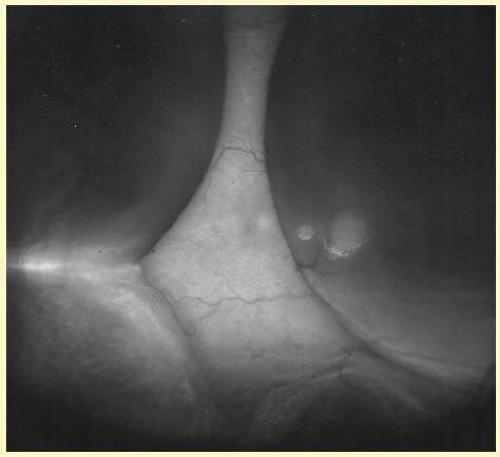
Ciliochoroidal effusions may have an annular, lobular (Fig. 52.4), or flat (Fig. 52.5) ophthalmoscopic appearance. Annular effusions occur around the ciliary body and peripheral choroid. Lobular effusions are large hemispheric detachments that bulge toward the center of the globe. Flat effusions are most often apparent in isolated peripheral choroidal areas, where local structures limit fluid extension. A local stimulus, such as a limbal incision, can lead to suprachoroidal edema, even in remote areas, by way of free dissection of fluid. Occasionally, patients will present with coexisting ciliochoroidal effusion and rhegmatogenous retinal detachment.24,25,26 The retinal hole may be hidden in the choroidal mounds. Such detachments tend to occur in older patients who have a history of previous ocular surgery.
FIG. 52.3 Retinal pigment epithelial abnormality with streaks of hypertrophy and hyperplasia in an eye with resolving ciliochoroidal effusion. The arrowhead indicates Verhoeff streak. (From Verhoeff FH. The nature and origin of the pigmented streaks caused by separation of the choroid. JAMA. 1931;97:1873, with permission.)
FIG. 52.4 Clinical appearance of a lobular type of ciliochoroidal effusion.
FIG. 52.5 Flat ciliochoroidal effusion. The ora serrata is visible without scleral depression in a patient with Schepens-Brockhurst syndrome. The arrow indicates the ora bay.
DIFFERENTIAL DIAGNOSES
A ciliochoroidal effusion may be mistaken for a malignant melanoma in the ciliary body or choroid.27 Transillumination, fluorescein angiography, ultrasonography, and computed tomography may assist in distinguishing an effusion from a melanoma. Increased transillumination may be observed with a serous ciliochoroidal effusion and has been referred to as the Hagen sign.28 Pigmented choroidal melanomas may not transilluminate; however, in some cases of ciliary body melanoma, particularly nonpigmented tumors, transillumination may not be reduced. In fact, in some cases the tumor may even transilluminate. A rare case of coexisting ciliochoroidal detachment and choroidal melanoma has been reported.29 The eye had a typical postoperative ciliochoroidal detachment that masked a multilobed uveal melanoma that was not appreciated preoperatively.
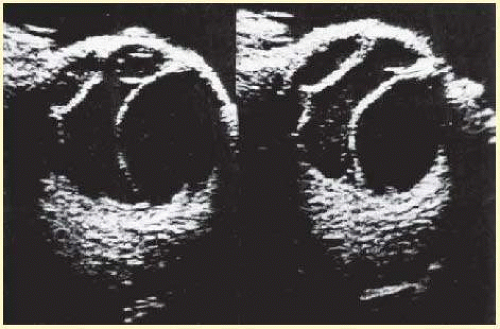
A ciliochoroidal effusion and other benign processes may be accurately differentiated from choroidal tumors with B-scan ultrasonography, as reported by Coleman,30 in more than 60% of cases. Ultrasonography can distinguish a ciliochoroidal effusion from a retinal detachment by the acute anterior angle of the acoustic shadow of an effusion and its extension anterior to the ora serrata (Fig. 52.6). The ultrasound finding of a diffusely thickened choroid posteriorly should alert the ultrasonographer and ophthalmologist to the possibility of a ciliochoroidal detachment more anteriorly. If posterior choroidal thickening is not associated with a peripheral ciliochoroidal detachment, other clinical entities should be excluded, such as posterior scleritis, choroidal inflammation, and intraocular tumors.31 Scleral infolding may ophthalmoscopically simulate a ciliochoroidal effusion in a hypotonus eye, and B-scan ultrasonography may assist in the diagnosis.32
FIG. 52.6 B-scan ultrasound of a choroidal effusion. An acute anterior angle and extension anterior to the ora serrata help to distinguish this as a choroidal effusion, rather than a retinal detachment.
These adjunctive tests can also differentiate a serous from a hemorrhagic ciliochoroidal effusion. In a serous ciliochoroidal effusion, fluorescein angiography demonstrates characteristic background fluorescence, RPE abnormalities, and leakage from the large choroidal vessels, whereas a hemorrhagic ciliochoroidal effusion blocks these angiographic patterns.12,33 Peyman et al.32 demonstrated the usefulness of computed tomography in differentiating a serous effusion from a hemorrhagic choroidal detachment.
ETIOLOGIC CLASSIFICATION
A ciliochoroidal effusion may be idiopathic, or it may be due to a systemic or ocular abnormality (Table 52.2).
Iatrogenic and Traumatic Injury
A ciliochoroidal effusion may result from iatrogenic medical or surgical intervention or ocular trauma. Systemic medications that have been associated with ciliochoroidal effusions include hydrochlorothiazide-triamterene,11 hydrochlorothiazide,34 buproprion,35 indapamide,36 acetazolamide,37 methazolamide,38 and topiramate,39 as well as other sulfonamides.40,41 Topical treatment with the prostaglandin analogs latanoprost42 or travoprost43 has also resulted in choroidal effusions.
Various surgical procedures may be complicated by a ciliochoroidal effusion during or after the procedure. An expulsive effusion can mimic an expulsive hemorrhage during cataract extraction44,45,46,47or glaucoma surgery, especially in patients with prominent preoperative episcleral vessels, as in Sturge-Weber syndrome.48 Varying degrees of postoperative suprachoroidal edema may develop after cataract extraction (Figs. 52.7 and 52.8),1,9,33,44,45,49,50,51,52,53,54,55,56,57 iridectomy (Fig. 52.9), filtering procedures (Fig. 52.10),1,9,33,48,58,59,60 retinal detachment surgery (Fig. 52.11),61,62,63,64,65 panretinal photocoagulation,66,67,68 or cryotherapy. Effusions have also been reported after uneventful laser in situ keratomileusis (LASIK) in two patients with hypermetropia but otherwise normal eyes.69 A postoperative ciliochoroidal effusion can occur weeks, months, or even years after surgery.51,70 In the late postoperative period after filtration surgery, hypotony and ciliochoroidal detachment have developed in patients when timolol, dorzolamide, or acetazolamide therapy was instituted.70,71
Intraoperative hypotony combined with intrinsic vascular disease may lead to a serous or hemorrhagic ciliochoroidal effusion during or after retinal detachment surgery.61,62,63,64,65 The hypotony that occurs during the drainage of subretinal fluid is usually of relatively short duration. Diathermy, cryotherapy, and vortex vein compromise due to buckle placement,67 may further disturb the choroidal vasculature, and contribute to the leakage of fluid into the suprachoroidal space. The incidence of effusion formation correlates with the circumferential length and posterior position of the scleral buckle.62 Scleral suture placement less than 14 mm posterior to the limbus decreases the risk of an effusion.
TABLE 52-2 Etiologic Classification of Ciliochoroidal Effusion
Iatrogenic Injury
Medications11,34-43
Anterior segment surgery (with or without cyclodialysis)
Cataract extraction1,9,33,44,45,47,49-57
Glaucoma filtering procedures1,9,33,48,58-60
Iridectomy
Laser in situ keratomileusis (LASIK)69
Glaucoma surgery in patients with prominent episcleral vessels
(Sturge-Weber syndrome)48,157
Panretinal photocoagulation66-68
Retinal detachment surgery61-65,130
Traumatic Injury
Accidental ocular perforation1
Blunt trauma72
Inflammation
Campylobacter jejuni98
Episcleritis88-90
Influenza (H1N1)99
Nonspecific vasculitis
Occlusive vasculitis78
Orbital pseudotumor86,87
Pars planitis82,83
Polyarteritis nodosa96,97
Rheumatoid arthritis81
Scleritis9,20,21,78,81,91,92
Subconjunctival abscess85
Sympathetic uveitis78-80
Syphilitic posterior uveitis77
Systemic lupus erythematosus93,94
Toxoplasmosis retinochoroiditis78
Uveitis73-76
Vogt-Koyanagi-Harada syndrome84
Wegener granulomatosis95
Vascular Causes9,100-107,160
Valsalva maneuver100,101
Carotid-cavernous sinus fistula105
Dural-sinus fistula104,106,107
Hypertension
Eclampsia160
Hypoproteinemia9,102,103
Malignancy
Metastatic carcinoma to the choroid109
Leukemia9
Choroidal melanoma108
Multiple myeloma78
Orbital lymphoma110
Myelodysplastic syndrome111
Primary Scleral Abnormality
Nanophthalmos112-117
Uveal effusion syndrome12,13,82,83,116,118
Idiopathic ciliochoroidal effusion9,78
FIG. 52.7 Large lobule of a ciliochoroidal effusion that occurred after cataract extraction.
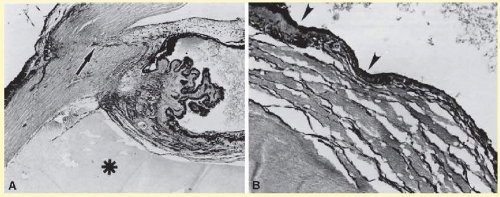
FIG. 52.8 This choroidal and ciliary body detachment, which occurred after intracapsular cataract extraction, was mistaken for a malignant melanoma. A: Iris incarceration in the wound (arrow) and extensive ciliary body effusion consisting of a dense, proteinaceous material (asterisk) (hematoxylin-eosin, 115X). B: Effusion of the choroid near the ora serrata by a moderately dense, proteinaceous material without inflammatory cells. Note folds of choroid (arrowheads) (hematoxylin-eosin, 115X). (From Bard LA. Eyes with choroidal detachments removed for suspected melanoma. Arch Ophthalmol. 1965;73:320, with permission.)
The formation of suprachoroidal edema and secondary shallowing of the anterior chamber angle has been documented after panretinal photocoagulation.66,67,68 The mechanism may involve leakage from thermally affected vessels, resulting in increased permeability of the choriocapillaris. Serous fluid may then collect in the suprachoroidal space and form an effusion.67 This may be prevented by staging the laser treatment so that less than 1,000 laser burns are applied during one treatment session, or by limiting cryotherapy to less than two rows for no more than 180 degrees. If an effusion develops despite these measures, treatment with corticosteroids may be beneficial.
Blunt and penetrating ocular trauma and perforated corneal ulcers may also be associated with choroidal edema.1,72 Trauma that causes prolonged hypotony or severe inflammation is likely to produce ciliochoroidal edema.
Inflammation
Intraocular inflammation may lead to ciliochoroidal effusion. Inflammation is accompanied by vasodilation, which can lead to leakage and accumulation of serous fluid within the suprachoroidal space. Involvement of the ciliary body may produce symptoms of myopia and blurred vision.
Various uveitides,73,74,75,76 including syphilitic uveitis,77 sympathetic ophthalmia (Fig. 52.12),78,79,80 toxoplasmosis (Fig. 52.13),78 rheumatoid arthritis,81 pars planitis,82,83 and Vogt-Koyanagi-Harada syndrome,84 may be associated with the collection of suprachoroidal fluid. In Vogt-Koyanagi-Harada syndrome, a diffuse, bilateral uveitis may lead to an exudative choroidal effusion and secondary nonrhegmatogenous retinal detachment. In addition to associated extraocular clinical features (e.g., vitiligo, poliosis, dysacousia), the presence of pleocytosis in the cerebrospinal fluid (CSF) may help differentiate Vogt-Koyanagi-Harada syndrome from uveal effusion syndrome, which characteristically lacks pleocytosis.
FIG. 52.9 A: This serosanguineous ciliochoroidal effusion (arrow), which occurred after iridectomy for an iris melanoma in a 68-year-old man, was mistaken for a choroidal melanoma (hematoxylin-eosin, 25X). B: Site of the limbal wound (arrowhead) with incarceration of the iris base and residual melanoma in the iris, anterior aspect of the ciliary body, and trabecular meshwork (hematoxylin-eosin, 60X).
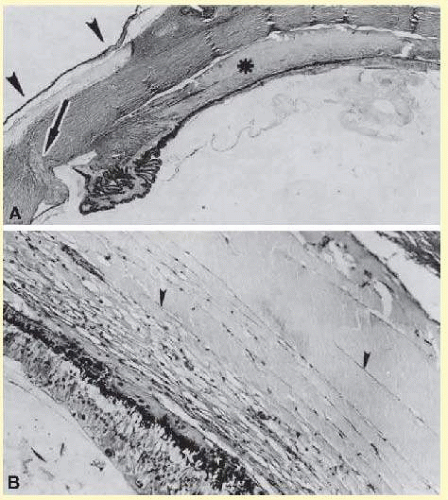
FIG. 52.10 A: This extensive ciliochoroidal effusion (asterisk), which occurred 4 years after iridencleisis in a 70-year-old man,50 was mistaken for a malignant melanoma. The iris (arrow) is incarcerated in the limbal wound, and a flat, edematous filtration bleb (arrowheads) is present (hematoxylin-eosin, 25X). B: Area of the ora serrata shows a ciliochoroidal effusion with proteinaceous material separating the tangentially oriented collagen fibers (arrowheads) that connect the choroid and ciliary body to the sclera (hematoxylin-eosin, 115X). (From Bard LA. Eyes with choroidal detachments removed for suspected melanoma. Arch Ophthalmol. 1965;73:320. with permission)
FIG. 52.11 A ciliochoroidal effusion that developed after retinal detachment surgery. (Courtesy of Retina Service, Wills Eye Hospital, Philadelphia, Pennsylvania.)
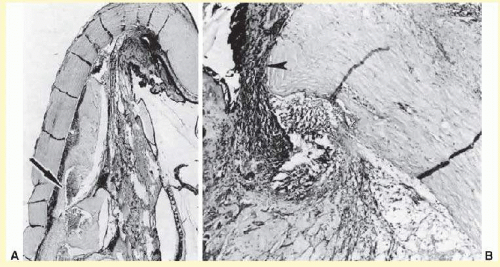
FIG. 52.12 A ciliochoroidal effusion in the eye of a 16-year-old boy, who developed sympathetic uveitis after a corneal laceration. A: Scar of the traumatic corneal perforation, with fibrous tissue ingrowth (asterisk) and adherent lens remnants (arrowhead) (hematoxylin-eosin, 18X). B: The appearance of a ciliochoroidal effusion (asterisk) that was first observed in the eye 2 months after corneal perforation and before the development of uveitis in the fellow eye (hematoxylin-eosin, 96X). C: The choroid posteriorly is greatly thickened by intense lymphocytic infiltration in which foci of epithelioid cells (arrowheads) display pigment phagocytosis in the absence of necrosis (hematoxylin-eosin, 185X).
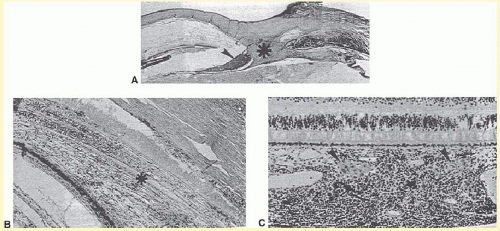
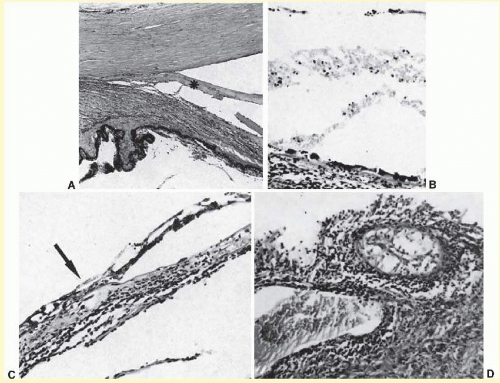
FIG. 52.13 A: A ciliochoroidal effusion (asterisk) associated with Toxoplasma retinochoroiditis (hematoxylin-eosin, 50X). B: The retina temporally is totally necrotic with encysted T. gondii (hematoxylin-eosin, 25X). C: An old chorioretinal scar (arrow) posterior to the area of necrotic retina (hematoxylin-eosin, 160X). D: Intense vasculitis and perivascular lymphocytic infiltration of the central vessels in the optic nerve head (hematoxylin-eosin, 185X).
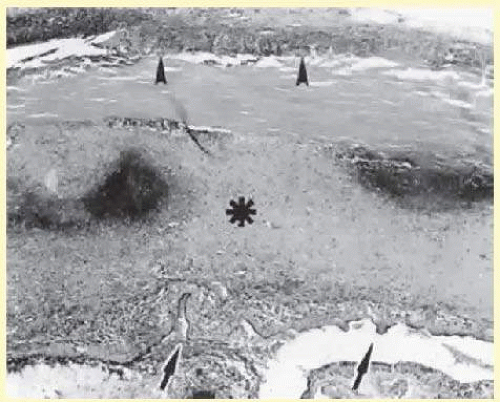
FIG. 52.14 Extensive ciliochoroidal effusion (asterisk) associated with a zonular granulomatous inflammatory infiltration in the episclera (arrowheads) of the eye of a 78-year-old man with rheumatoid arthritis. Diffuse, nodular inflammatory infiltrates are present in the markedly edematous ciliary body and choroid. There are several folds of retinal pigment epithelium and inner layers of choroid (arrows) and a flat serous detachment of the retina (hematoxylin-eosin, 40X). (From Hurd ER, Snyder WM, Ziff M. Choroidal nodules and detachments in rheumatoid arthritis. Am J Med. 1970;48:273, with permission.)
A subconjunctival abscess,85 orbital pseudotumor,86,87 episcleritis,88,89,90 scleritis (Fig. 52.14),9,20,21,78,81,91,92 and vasculitides (Figs. 52.15 and 52.16)93,94,95,96,97 such as systemic lupus erythematosus,93,94 Wegener granulomatosis (Fig. 52.16),95 polyarteritis nodosa,96,97 occlusive vasculitis,78 or nonspecific vasculitis (Fig. 52.15) can produce suprachoroidal edema even without overt signs of inflammation. Scleritis may sometimes produce choroidal inflammation with secondary vasodilation and serous effusion into the suprachoroidal and subretinal space. An infected scleral buckle may also produce a ciliochoroidal effusion months to years after its placement. Removal of sutures and all implanted material is necessary to promote resolution of the effusion.
Only gold members can continue reading. Log In or Register to continue