Congenital narrowing of the nasal airway at the posterior choanae, which can be uni- or bilateral, is an uncommon condition in pediatric patients. The surgical management of choanal atresia varies widely in different centers. This article discusses the different surgical strategies including: dilation and stenting; trans-palatal repair; and transnasal resection utilizing endoscopic sinus surgery (ESS) techniques. The merits of stents, lasers, CT-guided surgery, and the use of additional agents including mitomycin C are reviewed, as well as the particular problems associated with managing bilateral choanal atresia in neonates.
Congenital narrowing of the nasal airway at the posterior choanae, which can be uni- or bilateral, is an uncommon condition in pediatric patients. The surgical management of choanal atresia varies widely in different centers. This article discusses the different surgical strategies including: dilation and stenting; trans-palatal repair; and transnasal resection utilizing endoscopic sinus surgery (ESS) techniques. The merits of stents, lasers, CT-guided surgery, and the use of additional agents including mitomycin C are reviewed, as well as the particular problems associated with managing bilateral choanal atresia in neonates.
Incidence
Choanal atresia is manifested by narrowing and closure of the posterior choanae of the nose. It has been recognized for more than 200 years and was first described by Roederer in 1755. The reported incidence is between 1 in 5000 to 1 in 9000 live births. There may be mixed bony or membranous obstruction, but, in the majority of cases, it is bony. Original reports suggested a 90% bony stenosis and 10% membranous obstruction, but more recent analysis suggests a mixed bony/membranous in 70% and pure bony in 30%.
There is not just a membrane across the posterior choanae but also medialisation of the pterygoid plates and lateral wall of the nose. The boundaries of the atretic plate are created by the undersurface of the body of the sphenoid bones superiorly, the medial pterygoid lamina laterally, the vomer medially, and the horizontal portion of the palatine bone inferiorly. The lateral wall is the principle challenge of choanal atresia surgery, as most surgical corrections tend to address the septum and atretic plate only. There may also be abnormalities of the skull base with either very thickened atretic plates or with defects in the skull base. These associated abnormalities may make surgery considerably more challenging.
There is a predominance of females over males in most series and unilateral is more common than bilateral, although the reported series often come from specialized centers and they may have over-representation of bilateral cases. About one half of these patients have other associated anomalies or syndromes such as CHARGE, Crouzon, Pfeiffer, Antley–Bixler, Marshall–Smith, Schinzel–Giedion, and Treacher Collins syndromes.
Embryology
A number of embryological models for the development of choanal atresia have been proposed, although none of them are wholly supported by convincing clinical evidence. Theories include: the persistence of the buccopharyngeal membrane from the foregut; failure of perforation of the nasobuccal membrane of Hochstetter; abnormal persistence or location of mesoderm forming adhesions in the nasochoanal region; or misdirection of neural crest cell migration.
Molecular models
Retinoic Acid
More recently other molecular pathological theories have been developed. Abnormalities in vitamin A metabolism are associated with choanal atresia. Retinoic acid is metabolized from vitamin A by retinaldehyde dehydrogenase (Raldh). Retinoic acid (RA) then transduces a cellular signal via nuclear receptors for retinoids (eg, RA receptor and 9-cis-RA receptor). This signal is indispensable for ontogenesis and homeostasis of numerous tissues. Dupe and colleagues showed in mice that a Raldh3 knockout suppresses RA synthesis and causes malformations restricted to ocular and nasal regions, which are similar to those observed in vitamin A-deficient fetuses or in retinoid receptor mutants. A Raldh3 knockout mouse (unable to produce any Raldh3) notably causes choanal atresia, which is responsible for respiratory distress and death of Raldh3-null mutants at birth. Dupe suggests that choanal atresia may be caused by impaired RA down-regulation of FGF-8 expression to allow perforation of the nasobuccal membrane. Remarkably, they also showed in this knockout mouse model that choanal atresia was prevented by a simple maternal treatment with RA. Supporting a role for FGF signaling in choanal atresia is the observation that there is often choanal stenosis or atresia in human craniosynostosis syndromes resulting from constitutive activation of FGF-receptors.
Thionamides and Choanal Atresia
Several case reports have associated prenatal use of thionamides (eg, methimizole or carbimizole) with choanal atresia in the offspring. A case control study by Barbero and colleagues investigated 61 children with nonsyndromic choanal atresia and found that 10 of 61 had mothers that were treated for hyperthyroidism with thionamides, compared with only two of 183 age-matched controls. This increased incidence of choanal atresia in hyperthyroid mothers treated with carbimizole is likely caused by either hyperthyroidism or the thionamides. The majority of hyperthyroid mothers have Graves’ disease and elevated levels of stimulating antibody for the thyrotropin receptor. In both animal models and human studies, elevation of thyrotropin can cause altered expression of FGF, FGF receptors and angiogenic factors, which plausibly may play a role in development of choanal atresia.
Ongoing research into the molecular mechanisms that may cause choanal atresia may reveal further insights into the pathobiology of choanal atresia.
Genetic Causes
The CHARGE association was first described in 1979 by Hall, in 17 children with multiple congenital anomalies who were ascertained by choanal atresia. In the same year, Hittner and colleagues reported this syndrome in 10 children with ocular colobomas and multiple congenital anomalies, hence the syndrome is also called Hall-Hittner syndrome. Pagon and colleagues, in 1981 first coined the acronym CHARGE association (Coloboma, Heart defect, Atresia choanae, Retarded growth and development, Genital hypoplasia, Ear anomalies/deafness). More recently an expert group defined the major (the classical four C’s: Choanal atresia, Coloboma, Characteristic ears and Cranial nerve anomalies) and minor criteria of CHARGE syndrome. Individuals with all four major characteristics or three major and three minor characteristics are highly likely to have CHARGE syndrome ( Table 1 ).
| Major | Minor | Diagnosis |
|---|---|---|
|
| Typical CHARGE: four majors or three majors and three minor |
Studies prior to the modern definition of CHARGE reported that about 30% children with choanal atresia had CHARGE syndrome, based on clinical diagnosis. However, these quoted rates may change now that abnormalities in the CHD7 gene have been identified in 64% of patients diagnosed with CHARGE, allowing screening of the gene. The function of the CHD7 gene is largely unknown. Certainly, the presence of uni- or bilateral choanal atresia should precipitate active examination for other signs of CHARGE.
Embryology
A number of embryological models for the development of choanal atresia have been proposed, although none of them are wholly supported by convincing clinical evidence. Theories include: the persistence of the buccopharyngeal membrane from the foregut; failure of perforation of the nasobuccal membrane of Hochstetter; abnormal persistence or location of mesoderm forming adhesions in the nasochoanal region; or misdirection of neural crest cell migration.
Molecular models
Retinoic Acid
More recently other molecular pathological theories have been developed. Abnormalities in vitamin A metabolism are associated with choanal atresia. Retinoic acid is metabolized from vitamin A by retinaldehyde dehydrogenase (Raldh). Retinoic acid (RA) then transduces a cellular signal via nuclear receptors for retinoids (eg, RA receptor and 9-cis-RA receptor). This signal is indispensable for ontogenesis and homeostasis of numerous tissues. Dupe and colleagues showed in mice that a Raldh3 knockout suppresses RA synthesis and causes malformations restricted to ocular and nasal regions, which are similar to those observed in vitamin A-deficient fetuses or in retinoid receptor mutants. A Raldh3 knockout mouse (unable to produce any Raldh3) notably causes choanal atresia, which is responsible for respiratory distress and death of Raldh3-null mutants at birth. Dupe suggests that choanal atresia may be caused by impaired RA down-regulation of FGF-8 expression to allow perforation of the nasobuccal membrane. Remarkably, they also showed in this knockout mouse model that choanal atresia was prevented by a simple maternal treatment with RA. Supporting a role for FGF signaling in choanal atresia is the observation that there is often choanal stenosis or atresia in human craniosynostosis syndromes resulting from constitutive activation of FGF-receptors.
Thionamides and Choanal Atresia
Several case reports have associated prenatal use of thionamides (eg, methimizole or carbimizole) with choanal atresia in the offspring. A case control study by Barbero and colleagues investigated 61 children with nonsyndromic choanal atresia and found that 10 of 61 had mothers that were treated for hyperthyroidism with thionamides, compared with only two of 183 age-matched controls. This increased incidence of choanal atresia in hyperthyroid mothers treated with carbimizole is likely caused by either hyperthyroidism or the thionamides. The majority of hyperthyroid mothers have Graves’ disease and elevated levels of stimulating antibody for the thyrotropin receptor. In both animal models and human studies, elevation of thyrotropin can cause altered expression of FGF, FGF receptors and angiogenic factors, which plausibly may play a role in development of choanal atresia.
Ongoing research into the molecular mechanisms that may cause choanal atresia may reveal further insights into the pathobiology of choanal atresia.
Genetic Causes
The CHARGE association was first described in 1979 by Hall, in 17 children with multiple congenital anomalies who were ascertained by choanal atresia. In the same year, Hittner and colleagues reported this syndrome in 10 children with ocular colobomas and multiple congenital anomalies, hence the syndrome is also called Hall-Hittner syndrome. Pagon and colleagues, in 1981 first coined the acronym CHARGE association (Coloboma, Heart defect, Atresia choanae, Retarded growth and development, Genital hypoplasia, Ear anomalies/deafness). More recently an expert group defined the major (the classical four C’s: Choanal atresia, Coloboma, Characteristic ears and Cranial nerve anomalies) and minor criteria of CHARGE syndrome. Individuals with all four major characteristics or three major and three minor characteristics are highly likely to have CHARGE syndrome ( Table 1 ).
| Major | Minor | Diagnosis |
|---|---|---|
|
| Typical CHARGE: four majors or three majors and three minor |
Studies prior to the modern definition of CHARGE reported that about 30% children with choanal atresia had CHARGE syndrome, based on clinical diagnosis. However, these quoted rates may change now that abnormalities in the CHD7 gene have been identified in 64% of patients diagnosed with CHARGE, allowing screening of the gene. The function of the CHD7 gene is largely unknown. Certainly, the presence of uni- or bilateral choanal atresia should precipitate active examination for other signs of CHARGE.
Presentation of choanal atresia
The presentation of choanal atresia depends on three factors: whether the obstruction is unilateral, bilateral or associated with other craniofacial abnormalities.
Bilateral
The bilateral abnormalities present at birth with asphyxia neonatorum. Neonates are obligate nasal breathers and more than 50% desaturate if nasally obstructed. Bilateral choanal atresia presents as a medical emergency at birth. The usual presentation is of obvious airway obstruction, stridor, and paradoxical cyanosis (where infants turn pink when crying as they begin to breathe through an open mouth). A temporizing measure, such as an oral airway, McGovern nipple, or intubation is often required prior to definitive surgical treatment.
Unilateral
These typically present later (usually 5–24 months) and have unilateral obstruction and persistent nasal discharge. Diagnosis can rarely be delayed to adulthood and, on occasion, has been recognized after unsuccessful septal surgery.
Craniofacial Abnormalities
The children with craniofacial abnormalities make up a small but important subgroup of the choanal atresia population. They often have abnormal skull bases,with defects into the cranial cavity; intracranial injury following surgery has been reported. Furthermore, children with craniofacial abnormalities often have very thickened pterygoid lamina rather than a simple bony partition or membranous web across the posterior choanae. It is important that other airway issues, including other sites of airway obstruction, muscle tone, associated abnormalities, requirement for tracheotomy and feeding issues are considered during the assessment and surgical planning of these complex patients.
Investigation
Bilateral choanal atresia presents early with airway compromise, but unilateral atresia typically presents later in childhood with nasal discharge, unilateral nasal obstruction, or occasionally with unilateral otitis media. The clinical examination is revealing, and techniques, such as observing fogging on a cold metal speculum, movement of a wisp of cotton wool, or even detection using a tympanometer to confirm a closed cavity can raise the suspicion of atresia. A fine catheter introduced through the nose which fails to pass to the pharynx can aid diagnosis, although care must be taken in patients with other craniofacial abnormalities to prevent intracranial passage of the catheter. A flexible nasendoscope may be passed through a nasal cavity prepared with a decongestant and suctioned clear; this technique may reveal the atretic plate, although the view is sometime obscured with mucus.
The definitive diagnosis is established with a CT of the paranasal sinuses and skull base, preferably after suctioning and decongestion of the nasal cavity, because it is difficult to distinguish radiologically a membranous occlusion from mucus in the unprepared nose. Radiological evaluation of choanal atresia should be obtained after stabilization of the patient. CT is performed to identify the nature and severity of the anatomic deformity and to estimate the size of the nasopharynx. When the diagnosis is questionable, CT will differentiate other causes of bilateral nasal obstruction, such as pyriform aperture stenosis or bilateral nasolacrimal duct cysts from choanal atresia.
Unilateral causes of nasal obstruction, such as nasal foreign body, turbinate hypertrophy, septal deviation, antrochoanal polyp, or nasal tumor, can also be differentiated from choanal atresia by CT. CT usually shows narrowing of the posterior nasal cavity with medial bowing and thickening of the lateral wall of the nasal cavity, with impingement at the level of the anterior aspect of the pterygoid plates and enlargement of the posterior portion of the vomer, with or without a central membranous connection ( Fig. 1 ). The mean width of the posterior choanal airspace in the newborn (measured from the lateral wall of the nasal cavity to the vomer) is 0.67 cm, increasing to 0.86 cm at 6 years and to 1.13 cm by 16 years of age. In patients less than 8 years of age, the vomer generally measures less than 0.23 cm in width and should not exceed 0.34 cm; in children over 8 years, the mean vomer width is 0.28 cm and should not exceed 0.55 cm.

Surgical strategies
A variety of surgical strategies have been adopted for the treatment of choanal atresia. Johann George Roederer first described CA in 1755. Adolf Otto further described the anomaly in association with the description of the deformity of the palatine bones. In 1854, Carl Emmert was the first to described the blind transnasal puncture of the palate using a curved trochar to establish an airway in a living infant.
Unfortunately, although more than 350 articles have since been published on the surgical management of choanal atresia, the majority of series are single surgeon or institution studies of small numbers of patients collected over a number of years, and often receiving a variety of techniques. This literature makes it difficult to make firm recommendations for surgical technique. The main outcome measures are “patency” of the choanae, although there is no standard definition of patency. Other measures, such as the number of operations and duration of stenting and symptoms, are used variably by different authors. The interpretation is made more difficult as the overall development of these children, including rates of tracheotomy and difficulties with feeding and global progress, are often determined by other comorbid conditions associated with choanal atresia. Consequently, although there is a substantial literature on the treatment of choanal atresia, the optimum technique is not fully established. The choice comes down, in part, to surgical preference.
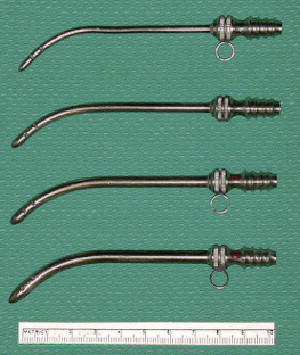
Transnasal Puncture
Transnasal puncture with Fearon dilators or urethral sounds is a long-used and safe technique to establish an airway ( Fig. 2 ). It is essential that the sounds are passed under direct vision with either a 120° endoscope or mirror examining the posterior aspect of the atretic plate, to ascertain that the dilators are passing into the correct position. If the plate is thick, it may be difficult to pass the dilators, and other techniques may be required, including drilling the atretic plate under direct vision. Simple transnasal puncture has a high recurrence rate of re-stenosis and it should be combined with other techniques including endoscopic resection, stenting or both. It is a very useful technique for the treatment of membranous and thin bony stenosis, and is simple to perform quickly and effectively, even in very small infants.