15 years, which coincides with the age of participation in sports for most athletes [3, 4]. Some patients may have what is called “tonsillar ectopia,” another normal variant in which the cerebellar tonsils are descended <5 mm beyond the foramen magnum, and is essentially never of clinical significance in the athlete. The Chiari malformation is so common that some authors have recently suggested it should be called the Chiari anomaly [5].
Evaluation
Chiari I malformations are thought to be due to a mismatch in size between the brain and skull. Due to a possible congenital mesodermal insufficiency during skull development, a small posterior fossa develops, and due to the compactness of the posterior fossa, the cerebellar tonsils herniate [6, 7]. Patients may be asymptomatic, or present with symptoms due to their tonsillar herniation, an associated syrinx which can be present, or both. The descended cerebellar tonsils can cause compression of the cerebellum, brain stem, and upper cervical spinal cord [2, 8]. This crowding is thought to cause the most common symptom, namely, headaches. These headaches, which are described as “tussive,” are exacerbated by transient increases in intracranial pressure such as when the patient coughs, laughs, or has some other transient spike in intracranial pressure related to physical exertion. These headaches are usually located in the occiput at the craniocervical junction, and the patient may describe them as either occipital headaches or neck pain. Other clinical findings from the compression which are less common include cranial nerve findings from brain stem compression, such as snoring, difficulty swallowing, double vision, or sleep apnea [9].
The compression at the level of the foramen magnum, in addition to causing direct pressure effects, can also disrupt normal egress of cerebrospinal fluid (CSF) of the fourth ventricle of the brain into the foramen magnum. When this happens, the Chiari malformation can lead to the development of syringomyelia, or a dilated cystic space within the spinal cord (see “Syringomyelia” section) [2].
When a Chiari I malformation is seen on a spine MRI, one must be careful to exclude mass lesions, hydrocephalus, or other conditions of the brain that may cause downward herniation of the cerebellar tonsils. The normal position of the cerebellar tonsils should not exceed 5 mm below the foramen magnum, based on studies of normal MRIs [10], which is usually taken as a line connecting the basion to the opisthion on a midsagittal image [11] (Fig. 8.1). Care should be taken to look for evidence of platybasia, basilar invagination, and atlanto-occipital assimilation as they may herald cervical instability [12]. There is also evidence that it not just the absolute magnitude of tonsillar descent that is concerning: tonsils that are peg-like or pointed are more concerning than those that are rounded and smooth [11, 13]. A syrinx secondary to Chiari I malformation, which is usually located in the cervical spine as opposed to lower in the spine, can also be seen in patients with Chiari I malformations (50–70 %) (Fig. 8.2). Therefore, in patients with a significant Chiari I malformation, it is prudent for them to undergo imaging of the spinal axis as well [11, 13].
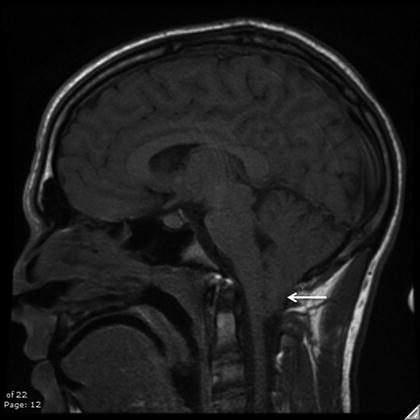

Fig. 8.1
Midsagittal T1-weighted MRI reveals a Chiari malformation with characteristic tonsillar herniation (white arrow)
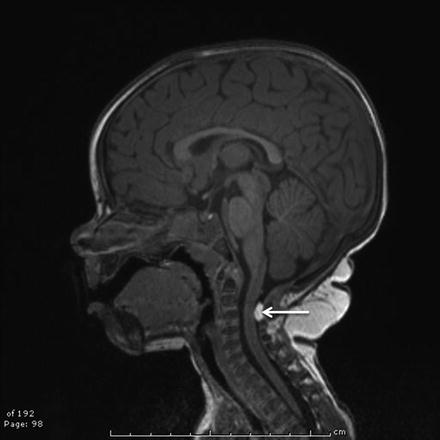
Fig. 8.2
Midsagittal T2-weighted MRI revealing a Chiari malformation (solid white arrow) with associated cervical syrinx (dotted white arrow)
Flow studies are occasionally employed in patients with CMI. The tight foramen magnum is thought to cause disturbance in CSF flow dynamics, and there is evidence that this can be seen on flow-sensitive phase contrast MRI sequences [14]. There is evidence that this CSF flow disturbance may be causally related to the formation of the syringomyelia [15]. Some authors have used this modality to determine the need for surgery and to measure the success of their surgical treatment [16]. Overall, it is not a critical study and generally does not add more information than the clinical symptomatology.
Treatment
It is important to delineate the etiology of a patient’s complaints, as many symptoms can be multifactorial, and the presence of a Chiari malformation does not always imply that it is the cause of the symptoms. In fact, most CMI are asymptomatic. For instance, many patients suffering a concussion undergo imaging of the brain, and an incidental Chiari malformation may be discovered because of its high prevalence in the population. Genuinely symptomatic patients can benefit from surgery, but most neurosurgeons agree that an asymptomatic Chiari malformation does not require surgery [5, 8, 17].
What are the reasons to consider operating on an athlete with asymptomatic Chiari malformation? One concern is that the Chiari malformation can become symptomatic over time, and therefore, the surgery should be performed prophylactically [18, 19]. This is not an adequate reason to perform surgery, as the condition can always be treated if symptoms develop. The more concerning issue is that a patient with a significant Chiari malformation could present with a catastrophic central nervous system (CNS) injury after trauma owing to preexisting spinal cord or brain stem compression from the malformation. There are anecdotal case reports of this phenomenon occurring [20, 21], but no prospective study has ever shown an asymptomatic Chiari presenting with catastrophic neurological injury. Therefore, the true incidence of this event is probably quite low, and several studies that have looked prospectively at patients with Chiari malformation have suggest that the natural history is benign [5, 8, 22]. The surgery to decompress a Chiari does carry some risks, and the very low risk of spinal cord injury in the asymptomatic patient needs to be weighed against the risks and potential complications of surgery. Although the literature has yet to define the exact degree of concern that a sport medicine clinician should have in this situation, most neurosurgeons do not advocate prophylactic surgery for asymptomatic Chiari malformations in competitive athletes. A recent retrospective review of over 100 patients diagnosed with Chiari malformations seen at our institution revealed that none of these patients sustained an injury resulting in death, paralysis, or coma in over 1500 athletic seasons. Similarly, in over 150 collision sports seasons, none of these athletes sustained an injury resulting in death, paralysis, or coma [4].
Return to Play
In general, in a patient with a Chiari malformation that is asymptomatic and has no associated syrinx, it is felt that there is no significant contraindication to return to play. It is our practice to allow these athletes to participate but to also inform the athletes and their families of the potential concerns that the Chiari malformation may become symptomatic or, as anecdotally reported, be implicated in the causation of severe neurologic injury. These decisions are complex enough that a multidisciplinary team consisting of a neurosurgeon and a sports medicine physician should be considered, although the vast majority of athletes will not experience adverse effects from participating in sports with this condition. We do not limit patients who have required surgical decompression but are now neurologically intact from future participation in any sport.
Syringomyelia
Syringomyelia is a condition in which the spinal cord is distended by the accumulation of fluid inside of the cord. The central canal, which runs the length of the spinal cord, is thought to be an extension of fluid-filled ventricular system of the brain. It had previously been thought to be collapsed after birth, but in the current era of increased high-quality MRIs being done on patients, it is being seen more regularly [23]. On the opposite end of the spectrum is the large syringomyelia cavity, which may be associated with conditions such as Chiari malformation, tethered spinal cord, spinal cord tumor, prior spinal cord injury, or prior infection around the spinal cord [2]. In general, it is easy to distinguish the normal dilated central canal from a pathological syrinx, as the former is centrally located and does not distend the spinal cord. Between these two extremes are occasional patients with slightly larger central canal expansion of unclear significance and prognosis that probably benefit from neurosurgical evaluation [14].
Evaluation
Imaging characteristics of the benign dilated central canal should include the absence of any other CNS pathology, a normal caliber of the spinal cord, and if contrast is administered, no enhancement. When this finding is discovered, it is often advisable that the entire spinal axis be imaged, to rule out a Chiari malformation or spinal cord tethering (Fig. 8.3).

Fig. 8.3
Idiopathic syrinx (white arrow) with no associated Chiari malformation or tethered cord (not shown)
A careful history will rule out preexisting conditions, such as Chiari-type symptoms as defined previously, prior meningitis, or prior spinal cord injury. If a syrinx is large enough to compress the crossing fibers in the spinal cord that are transmitting pain and temperature sensation subserved by the lateral spinothalamic pathway, patients may have a cape-like “suspended” sensory loss to pain and temperature or a pain syndrome marked by unusual burning or dysesthetic pain. Back pain, which is a common finding in athletes, is relatively unusual in patients with syringomyelia unless there is concomitant scoliosis. Physical exam findings can include reflex changes, including loss of an abdominal reflex, or hyperreflexia in the legs as compared to the reflexes in the arms. There are some case reports of a large syrinx causing more serious problems such as hemiplegia [24].
Treatment
It is not uncommon for a neurosurgeon to see athletes referred for syringomyelia, especially after imaging for back pain. The vast majority of these syrinxes are benign dilatations of the central canal [2, 23] and require no further imaging or treatment. As stated previously, it is important, especially for large syringes, that the extremes of the spinal axis be imaged to rule out a Chiari malformation or a tethered spinal cord. In the absence of concerning findings on the physical exam, or concerning details in the history, no treatment or additional investigation is required for these findings. When a true syringomyelia is present, the treatment must be designed to treat the underlying conditions. For instance, if the syrinx is the result of CSF circulation alterations caused by a significant Chiari malformation, surgical decompression of the Chiari malformation is encouraged. This surgical decompression often leads to regression of the resultant syringomyelia [17, 25]. Direct surgery on a syrinx is often unnecessary and unsuccessful [26, 27].
In general, any syrinx-associated conditions, including tumor, tethered cord, postinfectious or secondary to traumatic spinal cord injury, or Chiari malformation, require referral to a neurosurgeon.
Return to Play
Athletes should not be restricted from play because of a benign dilatation of the central canal. The athlete should be reassured that this is a normal anatomic variant, and as long as there are no associated findings on imaging, no further workup is required [23, 28].
It is important that if there is an underlying condition causing a syringomyelia, this underlying condition be treated. The syrinx usually will regress after dealing with the underlying condition, and the recommendations about return to play will in general coincide with the recommendations associated with this underlying condition.
Spinal Cysts
Spinal cysts are different from syringomyelia in that they are areas of fluid external to the spinal cord, rather than within the spinal cord. They may occur in different areas of the spinal cord, and due to their heterogeneity in presentation and rarity, generalizations about management are difficult. Arachnoid cysts, which are contained beneath the dura, are often found ventrally in the cervical spine and dorsally in the thoracic and lumbar spine [29]. When associated with an expansion of the dural sac along the nerve root, these cysts are called perineural cysts, and if in the lumbosacral spine, these are called Tarlov cysts [30]. Meningoceles are extradural cysts that occur in the caudal end of the dural sac, and patients often present with deep tailbone pain, but also occasionally with bowel and bladder dysfunction.
Evaluation, Treatment, and Return to Play
A comprehensive review of all the different spinal cysts and their management is beyond the scope of this chapter. However, due to their rarity and nuances, a neurosurgical consultation is recommended for patients found to have such lesions. Most patients will not require surgical intervention and will be allowed to return to play. Again, a case-by-case evaluation and multidisciplinary approach is needed when dealing with these lesions.
Tethered Cord
Tethered spinal cord refers to any condition in which the spinal cord is pathologically attached to the bones or soft tissues of the back. Most of these conditions are discovered in infancy or early childhood due to the presence of lumbar or sacral cutaneous stigmata such as a dimple, hairy patch, fatty mass, discoloration of the skin, or other unusual findings such as a skin appendage. Later presentations in childhood or in teenage years are thought to be due to symptoms from tension on the lower spinal cord, including back pain, bowel and bladder control difficulties, limb asymmetry or scoliosis, or neurologic dysfunction [31, 32]. These later presentations might be seen in the athlete and present to the sports medicine physician. In addition, tethering can rarely be seen in the cervical region, often the result of prior pathology such as surgery or neck injury, and therefore not likely to present without prior knowledge. However, congenital tethering of the cervical region can occur (Fig. 8.4).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
