Chemodenervation of Extraocular Muscles
Edward G. Buckley
Lucas Trigler
Derek B. Hess
In the early 1970s, Dr. Alan B. Scott discovered that when botulinum A toxin was injected into an extraocular muscle, a prolonged, dose-related reversible paralysis was caused that could be used to treat strabismus.1 Beginning in 1977, hundreds of investigators injected thousands of patients with botulinum A toxin to treat a wide variety of ocular motility disorders. After establishing its efficacy and safety, botulinum A toxin was approved in December 1989 as a treatment for strabismus in adults and children over the age of 12. The addition of botulinum A toxin has greatly expanded our capabilities for treating strabismus.
MECHANISMS OF ACTION
Six antigenically distinct forms of botulinum toxin (A to F) are produced by the bacterium Clostridium botulinum. Botulinum toxin type A is used clinically because it retains its toxicity, yields highly potent culture fluids, and can crystallizes easily into a stable form. Botulinum A toxin exerts its paralytic effect by rapidly and strongly binding to the presynaptic nerve terminal of cholinergic axons.2,3 The toxin is then internalized into the intracellular compartment where it inhibits the release of acetylcholine-containing vesicles.4 Within 6 hours after injection a complete decline of miniature end plate potentials occurs, but the clinical effect does not peak for approximately 5 to 7 days.1,5 This delay may be related in part to spontaneous release of nonvesicular acetylcholine.6 Eventually, the muscle becomes denervated and atrophic changes occur. The paralytic effect usually subsides over 3 to 4 months but some effects may persist for as long as 6 months. Muscle function slowly returns when the axon terminal forms new sprouts that result in new synaptic contacts on adjacent muscle fibers.7
The clinical effectiveness of botulinum A toxin is related to the completeness and duration of the paralysis of the injected muscle and to the condition that is treated (i.e., nonparalytic versus paralytic strabismus). Prior to the use of botulinum A toxin it had been observed that patients who recovered from sixth-nerve palsies often had a residual esotropia even though lateral rectus muscle function had apparently returned to normal. In such cases, the longer the paralysis persisted the more likely it was that a permanent deviation would occur. This change in ocular alignment was thought to be secondary to a mild residual weakness of the involved muscle (i.e., lateral rectus) plus contracture of its antagonist muscle (i.e., medial rectus). A similar mechanism is postulated to be responsible for the effects seen after botulinum A toxin injection, that is, weakness of the injected muscle plus contraction of its antagonist.
Once injected into the extraocular muscle botulinum A toxin binds rapidly to the nerve terminals, thereby limiting exposure to the systemic circulation. Until recently, antibodies could not be detected in humans exposed to therapeutic botulinum A toxin injections. However, an in vivo mouse neutralization assay has been developed that can detect serum antibodies to botulinum A toxin.8 Although not yet documented in patients treated for strabismus, clinical resistance to the effects of subsequent injections of botulinum A toxin has been correlated with the presence of antibodies to botulinum A toxin detected by this bioassay.9
The commercial preparation of botulinum A toxin (Oculinum) is distributed by Allergan Pharmaceuticals, Inc. (Irvine, CA) in a frozen, lyophilized form that is very stable. Once reconstituted into a solution, it must be used within hours because its effectiveness deteriorates rapidly. Care must be used in handling the reconstituted toxin because of its susceptibility to damage from preservatives, fluctuations in pH, heat, vigorous shaking, and rapid injection.10 The standard unit for measuring the potency of botulinum A toxin is derived from a mouse assay.11 One unit of botulinum A toxin is the lethal dose for 50% of a group of 18- to 20-g female Swiss-Webster mice. The median lethal dose (LD50) for humans is estimated at approximately 40 U/kg.1 The toxin available in the United Kingdom (Dysport, Ipsen Limited, Slough, Berkshire, UK) is much more potent; 1 ng of British toxin contains 40 mouse units, whereas 1 ng of American toxin contains 2.5 mouse units.12 This may explain the higher incidence of side effects with the more potent British toxin. The doses used in strabismus applications are roughly proportional to the mass of the muscle being injected and are less than 1/100 of the estimated human LD50.13
INDICATIONS
A wide variety of ocular motility disorders can be successfully treated with botulinum A toxin and the list is still evolving (Table 1). Originally it was thought that botulinum A toxin would only be useful for comitant deviations and in situations in which extraocular muscles were functioning normally. However, with time it has become apparent that its use can be extended to such complicated entities as postretinal detachment strabismus, thyroid myopathy, as an adjunct to transposition procedures for paralytic strabismus, in the treatment of oscillopsia from acquired nystagmus and stable deviations secondary to myasthenia gravis. In addition, botulinum A toxin has been found to be effective in small-angle deviations of less than 10Δ to 15Δ which might be considered too small for surgical intervention but still bothersome to the patient. Botulinum A toxin may also be a vessel-sparing alternative to strabismus surgery after trauma or other situations in which anterior segment blood flow has been compromised.
TABLE 1. Strabismus Categories Treatable with Botulinum A Toxin | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Botulinum A toxin can also be a useful alternative in those patients in whom general or local anesthesia is contraindicated. Those individuals with a history of malignant hyperthermia, chronic obstructive pulmonary disease, or significant cardiac abnormalities can often be treated successfully with botulinum A toxin avoiding anesthesia and its potential hazards in these high-risk patients.
CONTRAINDICATIONS
As a general rule, ocular motility abnormalities caused by tight and inelastic muscles or by chronic, complete nerve palsies do not respond well to botulinum A toxin injections. For a permanent change in ocular alignment to occur after a botulinum A toxin injection, there must be contracture of the antagonist to the injected muscle and this will not occur when the injected muscle is stiff or when its antagonist muscle is weak. In conditions such as chronic thyroid myopathy with fibrotic muscles, entrapped muscles after blowout fractures, or restrictive strabismus secondary to multiple operations to correct strabismus, only minimal relaxation results after injection allowing no opportunity for the antagonist muscle to shorten. In patients with chronic sixth-nerve palsies with no lateral rectus function, injecting the ipsilateral medial rectus will only result in temporary improvement because no permanent contracture of the paretic lateral rectus can be expected. This is also true for patients with Duane’s syndrome, with an inactive lateral rectus, or in persistent strabismus secondary to excessive surgical weakening procedures (e.g., recessions, myotomies).
Anatomic considerations must also be considered in selecting patients for botulinum A toxin injection. Those patients with an abnormal orbital anatomy caused by posttraumatic (e.g., blowout fractures) or congenital conditions (e.g., Crouzon’s disease), must be approached with caution because the extraocular muscles are often in abnormal positions. The presence of other orbital abnormalities such as tumors, vascular malformations, or bony defects may make botulinum A toxin injection difficult, thereby increasing the risk of significant complications after injection.
PATIENT SELECTION
Care must be taken in selecting patients because cooperation during the injection is essential. Because the procedure is somewhat threatening, it is imperative that the patient be considered capable of remaining in control in this stressful situation. Although age is certainly a factor, it alone cannot determine who will tolerate this procedure. Time spent before the injection educating the patient about the amount and duration of discomfort will help avoid surprises at the time of injection. The ability of the patient to tolerate an office forced duction test can be used to select which patients will be cooperative for the injection. Inability to remain calm and follow directions during forced duction testing will surely be amplified during an injection procedure. This is especially helpful in trying to decide whether or not a child or teenager will be a good candidate.
Until the ophthalmologist is familiar and experienced with the injection procedure, consideration should be given to treating only the horizontal rectus muscles. The vertical rectus muscles, because they have opposite functions from the nearby oblique muscles, require a higher level of expertise to avoid unwanted complications. Likewise, experience should be gained on adults before attempting injections in children.
ANESTHESIA
The conjunctival surface is anesthetized with several repeated installations of topical anesthesia (proparacaine, tetracaine, or cocaine) given liberally over several minutes. This should be placed in both eyes to reduce the urge of the untreated eye to blink during the procedure. Occasionally, 1% lidocaine can be injected over the muscle insertion in patients with significant scar formation secondary to multiple operations, scleral buckling procedures, or trauma. This does not interfere with the electromyographic (EMG) signal if given anteriorly. Because placement of the needle into the muscle is guided by an EMG signal, peribulbar or retrobulbar anesthesia has the risk of blocking the signal and is not usually necessary. Ketamine is recommended for children when sedation is required, since it tends to preserve the EMG signal. For children 1 to 6 years of age, intravenous ketamine at a dose of 0.5 to 1 mg/kg provides adequate sedation and still preserves EMG activity.14,15 Topical anesthetic drops must be used because low-dose ketamine provides sedation but not full anesthesia. Higher doses of ketamine (up to 2 mg/kg) have also been recommended.16
When inhalation anesthesia with nitrous oxide or halothane is used, the EMG recording is diminished or extinguished. Placement of the drug in the muscle belly can be done under direct visualization or during the waking-up process. If this is attempted, careful attention to eye position and anatomy are important. Usually the medication is delivered approximately 2.5 cm posteriorly in the muscle. Without the use of EMG, a more anterior injection may minimize adjacent muscle involvement. If EMG guidance is desired, an alternative approach requires waiting until the child is coming out of light stage (stage 2–3) anesthesia. At the point when extraocular movements are seen, the electrode is inserted rapidly in an attempt to locate the muscle before the patient becomes completely awake. This requires considerable skill and is somewhat cumbersome if mask anesthesia is used. In infants under 12 months of age injections can be performed using topical anesthesia and restraint. A hungry infant can sometimes be fed a bottle and remain quiet and comfortable throughout the entire procedure.17
PROCEDURE
The best results are obtained when botulinum A toxin is placed into the muscle in the region of the motor end plate, which for rectus muscles, is approximately 2.5 cm posterior to the muscle insertion. Recording an EMG response from the tip of a monopolar injection needle is an important aid in accurately localizing this position. Special 27-gauge, 1½-inch long, Teflon-coated, monopolar injection needles can be obtained for this purpose (Fig. 1). When attached to an audio EMG amplifier, a distinct, recognizable noise pattern results that can be used during the injection process to locate the appropriate muscle (Fig. 2). It is desirable to place the needle into the muscle on the first attempt because the drug diffuses readily along needle tracts and there is a risk of hemorrhage.
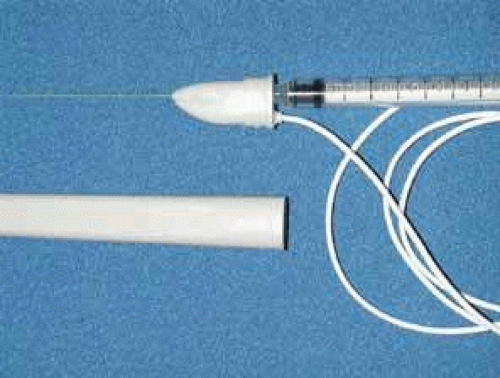 Fig. 1 Special 27-gauge, 1½-inch monopolar injection needle with Teflon coating. and positive electromyographic lead. The wire position can also be used to mark the position of the needle bevel. |
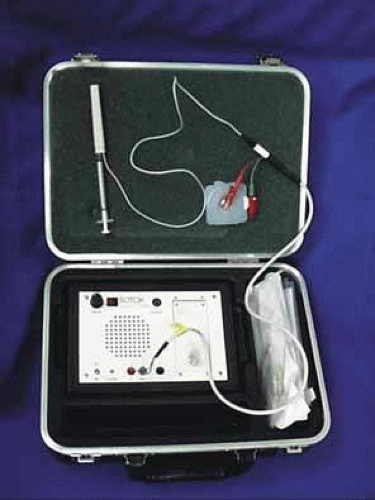 Fig. 2 Audio electromyographic device used for botulinum A toxin injections. A wire attaches to a special 27-gauge, Teflon-coated, monopolar injection needle attached to a tuberculin syringe. The device is grounded through a pediatric electrocardiographic electrode and fastened to the forehead. |
LOCATION
The patient should be made comfortable in the supine position (Fig. 3). Although this can be performed in an office chair, a flat examination table or similar setup is advisable both for patient comfort and stability of the head during the procedure. The room should be as free as possible from electrical signals that can interfere with the audio EMG recording device. Certain fluorescent fixtures and overhead wiring produce signals that can be picked up by the recorder, thereby interfering with assessment during the injection process. Loud background noise often occurs when the EMG device is turned on prior to inserting the needle into the conjunctiva. However, as soon as the needle touches the conjunctiva, this noise is greatly diminished. If this does not occur, then accurate localization of the muscle will be difficult. In this situation, reducing the illumination or turning off nonessential lights can be helpful.
 Fig. 3 Patient ready for botulinum A toxin extraocular muscle injection. Note the placement of the electrocardiographic electrode on the patient’s forehead medially for a medial rectus muscle injection. The patient is in the supine position and the head is supported comfortably on a pillow. A tray, table, or other support is necessary for the audio electromyographic device since the electrode wires are only 24 inches long. |
PREINJECTION PREPARATION
The dosage to be administers should be calculated (Table 2). Nonpreserved saline 0.9% is used to mix the Oculinum so that the desired number of units to be given are in a volume of 0.1 mL or less. Two milliliters of the reconstituted fluid is drawn into a tuberculin syringe; the monopolar electrode needle should not be used for this process. The 27-gauge, 1½-inch, Teflon-coated, monopolar electrode needle is then attached to the end of the tuberculin syringe. The total volume in the tuberculin syringe is reduced to to one-tenth of a milliliter by injecting the excess drug through the needle end. Because of the size of the needle and the small volume used, the needle barrel must be loaded with the drug to avoid undermedicating the patient. The location of the attachment of the wire onto the needle hub can be used as a reference point to determine the position of the needle bevel.
TABLE 2. Botulinum Toxin Dosage for Horizontal and Vertical Rectus Muscles (in units) | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
A pediatric electrocardiographic electrode is then attached to the patient’s forehead, making sure that a good contact is present (see Fig. 3). It should be placed medially for the medial rectus and laterally for the lateral rectus. If not already done, the patient should be informed that an audio signal will be used during the procedure so that he or she will not become startled when the amplifier is turned on. Next, turn on the amplifier and test the connections by touching the needle tip to the conjunctiva. Any background noise should become extinguished and an audible click should be heard. If this does not happen, the ground connection to the needle hub should be checked and possible interference from overhead lights, etc., investigated. This is also the time to make sure that adequate topical anesthesia has been achieved.
INJECTION TECHNIQUE
Before beginning, it should be explained to the patient that he or she will have to move the eyes into various gaze positions during the procedure. Therefore, it is important that the patient keep both eyes open and fixed on some target. It is helpful to have an assistant during the injection procedure. Standing at the head of the patient, the lids are held open with the fingers. The patient should look away from the field of action of the injected muscle, for example, when injecting the medial rectus have the patient begin by looking laterally with that eye (Fig. 4). The assistant can use a hand or other fixation target for this purpose. The patient should be reminded to keep both eyes open so that fixation is maintained.
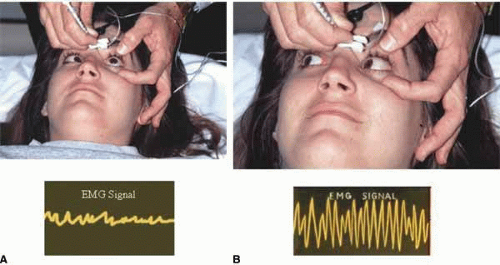 Fig. 4 Patient with a left sixth-nerve palsy undergoing left medial rectus muscle injection of botulinum A toxin. A. The eyelids are held open with the index finger and thumb and the patient is directed to look out of the field of action of the injected left medial rectus muscle. B. Once the electrode is inserted through the conjunctiva, the patient is asked to look into the field of action of the injected muscle to increase the electromyographic signal. The needle is advanced until the loudest signal is heard and then the fluid is injected. There is often attenuation of signal with injection. |
With the bevel facing the muscle, the needle is inserted through the conjunctiva 8 to 10 mm from the limbus. Once through the conjunctiva, the needle is advanced several more millimeters until the tip is beyond the equator. The assistant should move the fixation target slowly to the primary position so that the injection-muscle EMG signal can be activated. If the medial rectus is being injected, continue to advance the needle straight posteriorly aiming for the optic canal (Fig. 5). When injecting the lateral rectus the syringe has to be angled toward the ear at approximately a 45-degree angle to avoid touching the periosteum of the lateral orbital wall with the needle point, which is quite uncomfortable (see Fig. 5). A slight angle is also necessary when injecting the superior rectus. The inferior rectus is often easier to inject through the lower lid rather than the conjunctiva. As the needle is advanced and while listening to the EMG signal, continue to advance until a loud crackling noise occurs. If uncertainty exists as to whether this is from the appropriate muscle, have the patient slowly look out of the field of action of the muscle to be injected. The signal should decrease. Care must be taken to ensure that slow eye movements are made. This may be somewhat difficult because the patient may be anxious or apprehensive and may experience some discomfort. When the electrode is at the appropriate location, the reconstituted toxin is injected slowly. The EMG signal should diminish at this point as the tissue is pushed away from the tip by the entering fluid. Allow the needle to remain in this position for 10 to 15 seconds and then slowly withdraw the needle. The patient should be checked for signs of hemorrhage or other potential complications.
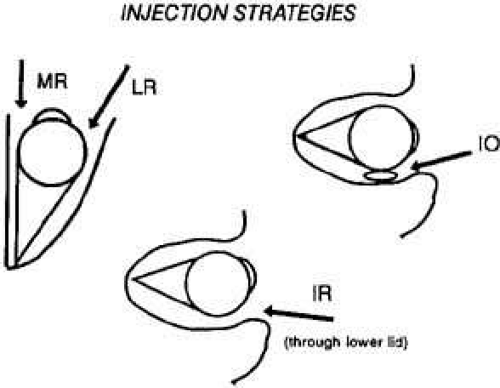 Fig. 5 The direction in which the monopolar electrode needle is advanced depends on the muscle injected. Top left. For medial rectus (MR) muscle injections the needle should be directed straight backward toward the orbital apex. For lateral rectus (LR) injections a 45-degree angle is necessary once the needle tip is past the equator. Top right. Inferior oblique (IO) injections should be directed slightly inferiorly and through the conjunctiva fornix. Bottom. Inferior rectus (IR) injections are somewhat difficult through the conjunctiva and may be easier to inject through the lower lid, especially in patients with restrictive disorders such as thyroid ophthalmopathy. |
POSTINJECTION MANAGEMENT
Once finished, the patient should be asked to sit up on the edge of the examination table but should not be allowed to stand until postinjection anxiety and bradycardia have subsided. Often the patient is so relieved that the process is over that an episode of lightheadedness or even syncope can occur. One to two minutes is usually all that is necessary at this time. It is not necessary to patch the eye or use antibiotics unless there is some concern about the injection process. The patient should be informed that topical anesthesia has been applied to the eye and ocular manipulation for the next 30 to 45 minutes should be discouraged. The patient should be observed for 5 to 10 minutes to make sure that no retrobulbar bleeding has occurred. Acetaminophen should suffice for any postinjection discomfort.
EXPECTED RESULTS
HORIZONTAL STRABISMUS
As a group, patients with horizontal strabismus as respond well to treatment with botulinum A toxin injection (Fig. 6).18192021222324 The results of several large studies are summarized in Table 3. As a general rule botulinum A toxin injections reduce a deviation by approximately 65%, and a little over half of patients have their deviation reduced to less than 10 Δ. The larger the deviation the greater the prism diopter change, but the less likely that the total deviation will be reduced to 10Δ or less. Overcorrections are rare and have occurred in fewer than 1% of patients. A single injection can be expected to reduce a deviation to less than 10Δ in approximately 30% to 35% of patients.20 Most patients, however, need more than one injection with the average number of injections varying anywhere from 1.3 to 2, depending on the type of strabismus and the size of the original deviation.19,20,23 After the toxin effect has disappeared, the stability of the postinjection deviation appears to be comparable to that achieved with surgery and is enhanced if there is potential to establish or regain fusion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


