Chapter 38 Central Neck Dissection
Technique
 Please go to expertconsult.com to view related video Central Compartment Dissection.
Please go to expertconsult.com to view related video Central Compartment Dissection.
Introduction
The wisdom of the Oracle of Delphi in the Temple of Apollo for advice and prophecy was renowned in ancient Greece as well as Boston. The term Delphian was first suggested by fourth-year medical student Raymon Randall to Oliver Cope, professor of surgery at Harvard Medical School, as an eponym for the prelaryngeal node and is found first in James Mean’s textbook The Thyroid and Its Diseases published in 1948. A pathologic Delphian node thus foretold a malignant diagnosis.1,2
Thyroid cancer lymph node (LN) metastases are common, and this is especially true in the central compartment. LN metastasis incidence rates vary depending on the mode of detection and definition of node positivity from 21% to 81% of patients with PTC overall.3 Studies of patients with PTC show macroscopic cervical nodal metastasis (as determined by preoperative physical exam (PE)/ultrasound/intraoperative detection) in 21% to 35% of patients at presentation.4–8 Thus, nodal surgery is required in approximately one third of patients presenting with PTC. Microscopically positive nodes in the neck overall are far more prevalent, occurring in 23% to 81% of patients with clinically negative preoperative nodal assessments who are operated on prophylactically.5,7,9–16 Recent studies show microscopically positive nodes occur in from 38% to 62% of the clinically N0 central neck.17–19
Indeed, the 2009 American Thyroid Association (ATA) guidelines note “completeness of surgical resection is an important determinant of outcome… , residual metastatic lymph nodes (LN) represent the most common site of disease persistence/recurrence… , and adequate surgery is the most important variable influencing prognosis.”20 Although empiric or prophylactic lateral lymph node dissection (pLND) has long been abandoned as overly aggressive surgical treatment, this debate continues to rage on with respect to the role of prophylactic central lymph node dissection (pCND) during total thyroidectomy for newly diagnosed papillary thyroid carcinoma.21 This debate is thoroughly discussed in the accompanying chapter, Chapter 37, Central Neck Dissection: Indications. Therefore, this chapter focuses on first defining the anatomy in the central neck and the terminology that should be used in describing this operation and then on the surgical technique to perform a comprehensive, yet safe clearance of lymph nodes in this area as judged necessary. Central neck dissection (CND) technique has been varyingly presented by numerous authors.22–26 Revision central neck dissection will be reviewed here briefly and is more thoroughly discussed in Chapter 53, Reoperative Thyroid Surgery.
Often primary therapeutic central neck dissection is performed in the setting of known macroscopic significant nodal disease. There is recent evidence that detection of macroscopic nodal disease is a goal achievable by preoperative radiographic mapping utilizing computed tomography/ultrasound (CT/US).27
Anatomy and Terminology
The ATA convened a working group of surgeons and endocrinologists to help elucidate the relevant anatomy and terminology in the central neck. The impetus for this effort was the lack of consistent definition and reporting of central neck dissection data in the literature. The end product of this effort was a manuscript published in the journal Thyroid in 2009 with endorsement from several societies including the ATA, the American Association of Endocrine Surgeons (AAES), the American Academy of Otolaryngology–Head and Neck Surgery (AAOHNS), and the American Head and Neck Society (AHNS).28
The central neck includes lymph node levels VI and VII. Level VI lymph nodes fall within the following boundaries: superior (the hyoid bone), inferior (the sternal notch), lateral (the carotid artery), posterior (the prevertebral fascia), and anterior (the undersurface of the sternothyroid muscles). Level VII lymph nodes are those associated great vessels superior mediastinal including the brachiocephalic vein and innominate artery and are included as the lowest portions of the ATA-defined central neck dissection. The approximate level of the innominate crossing of the trachea essentially defines the inferior border, on the cranial caudal axis, of central neck dissection. It should be acknowledged that this is an arbitrary inferior border designation when it comes to the left paratracheal region because the innominate artery does not extend to the left paratracheal region. Also the sternal notch and the innominate artery have a variable relationship with the artery rising above the notch in 25% of cadaveric dissections.29 Mediastinal lymphadenopathy located caudal to the brachiocephalic vein adjacent to the tracheal bifurcation is rare in patients with existing central neck metastases and is significantly related to poor tumor differentiation, and the presence of distant metastases and can be identified by preoperative CT scanning.30 Blood supply of lower paratracheal and pretracheal nodes may originate from the aortic arch and drain to subclavian or brachiocephalic veins. Adequately securing these often small diameter vessels is important during central neck dissection.
Although nodes can occur in a variety of locations within the central neck, the majority of central neck lymph nodes occur in four discrete regions (see Figure 38-1):
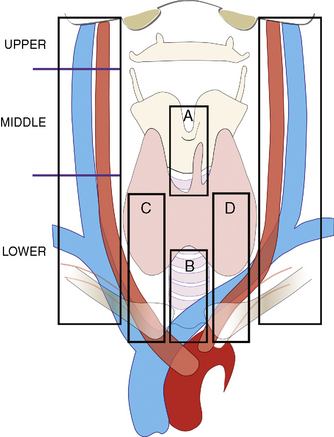
The important bilateral paratracheal regions are defined as a rectangle-oriented space starting cranially at the lower margin of the cricoid cartilage (typically below the area of the superior parathyroid) extending caudally to a level of the inferior central neck defined as noted above the level of the innominate artery crossing of the trachea. Although lymph nodes may occur in a variety of disparate locations within the central neck, such as paralaryngopharyngeal nodes, nodes deep to the omohyoid muscles as they extend to the lateral neck, retrocarotid nodes, and nodes associated with the course of the superior thyroid vessels and the omohyoid crossing of the carotid sheath, the majority of lymph nodes in the central neck clinically occur in these four areas (see Figure 38-1). All of these regions are readily available at primary thyroidectomy.
The paratracheal nodes have also been described as the recurrent laryngeal nerve chain of nodes that are a continuation of the ascending lateral tracheal chain of nodes. The number of nodes in the paratracheal regions range from 3 to 30 in number.31 Harrison in cadaveric and clinical dissections found 2 to 10 paratracheal nodes per side.32 Pereira has shown CND is typically associated with an average of 8 nodes on pathologic examination.33
The surgical literature on central neck dissection is problematic because of a lack of standardization in data reporting and anatomic definitions. The ATA consensus manuscript indicates that at a minimum, to qualify as central neck dissection the dissection must include prelaryngeal, pretracheal, and at least one paratracheal nodal basin.28 The specific regions dissected as part of the central neck dissection should, of course, be clearly identified in the operative report. A distinction should also be made by the surgeon as to whether the central neck dissection is prophylactic (i.e., intended to remove normal or microscopically positive lymph nodes) versus therapeutic (i.e., the removal of macroscopic nodal disease grossly apparent through physical exam, preoperative radiographic imaging, or intraoperative inspection; also termed clinically apparent). It should be noted that retrocarotid nodes hold an intermediate position between pure definitions of central and lateral neck regions. Although their position is intermediate, we feel due to their proximity to the recurrent laryngeal nerve as well as the vagus nerve, they are best managed as paratracheal (i.e., central neck nodes) nodes in terms of the required dissection for safe removal around the recurrent laryngeal and vagal nerves.
The ATA consensus manuscript on central neck dissection highlights that a central neck dissection may include only one paratracheal region and still be considered a central neck dissection.28 It is, of course, important to appreciate that the significant and dramatic possible complications from central neck surgery all arise from bilateral paratracheal dissection. One must therefore allow for aggressive bilateral paratracheal dissection only when there is a clear-cut definitive benefit to be achieved given the potential for both hypocalcemia and significant airway complications through bilateral nerve injury.
Evidence over many years demonstrated isolated removal of only macroscopically involved nodes, known as berry picking, violates compartment nodal surgery philosophy and is associated with higher rates of recurrence, which in turn brings the risk of increased morbidity associated with revision surgery.10,34 Thus, when nodes are detected, the surgeon should endeavor to dissect the entire subcompartment of the central neck, in which the nodes reside (i.e., regions A, B, C, and D in Figure 38-1).
Preoperative Evaluation
Prior to surgery requiring central neck dissection, preoperative laryngeal exam is necessary in all cases (see Chapter 15, Pre- and Postoperative Laryngeal Exam in Thyroid and Parathyroid Surgery).35 Subtle findings found on initial fiber-optic exam may require video stroboscopic examination.
The diagnosis of central neck nodal disease identified preoperatively warranting central neck dissection requires some clarification. For revision CND, rising thyroglobulin and isolated PET scan findings may suggest but do not definitively diagnose and target cervical nodal disease. Preoperative radiographic anatomic nodal mapping studies for the detection of macroscopic nodal disease are required. Of note, central neck node detection is hampered by the poor sensitivity of ultrasound in the detection of nodes in this compartment when the thyroid is present (often less than 25%) but is substantially improved with the addition of contrast-enhanced CT. Ultrasound and CT scan have been found to be superior to ultrasound alone for the detection of central neck lymphadenopathy.27 When ultrasound and CT scan preoperative mapping studies identify a highly suspicious node of 8 mm or larger, dissection of the nodal compartment is warranted. This objective radiographic map becomes part of the surgical plan and is preoperatively discussed with the patient and the endocrinologist. A radiographic map provides a valuable baseline study of nodal status at the time of surgery. The administration of iodinated contrast requires a minimal delay in the administration of radioactive iodine postoperatively in those patients requiring this modality, which is of no consequence and simply requires coordination between surgery and postoperative medical management.
Some prefer to document nodal disease requiring therapeutic dissection with preoperative ultrasound-guided fine-needle aspiration (FNA). If, however, high-resolution anatomic studies of ultrasound and CT scan strongly suggest highly suspicious metastatic disease, compartmental dissection can be implemented without FNA confirmation. These studies and, in turn, the resultant plan for therapeutic or prophylactic central neck dissection should be thoroughly reviewed and discussed with the patient preoperatively (see Chapters 14, Preoperative Radiographic Mapping of Nodal Disease for Papillary Thyroid Carcinoma, and 37, Central Neck Dissection: Indications).
Surgical Technique
We will outline primary central neck operation as a safe procedure in accordance with oncologic compartmental principles offered during primary thyroidectomy. The incision for complete central neck dissection during thyroidectomy is that of the standard thyroidectomy. Skin flaps are raised upward to the level of the thyroid notch and downward to the sternal notch. A vertical incision opens the midline between the strap muscles, from the thyroid notch to the sternal notch. Loupe magnification can be helpful in parathyroid and nerve identification during thyroidectomy and has great utility as well in central neck dissection. There is, in fact, evidence that the routine use of magnification is associated with a lower incidence of inadvertently removed parathyroid glands.36
Step 1: Prelaryngeal Dissection
The prelaryngeal nodes are easily visualized during the resection of the pyramidal lobe. They can be dissected at this time or after thyroidectomy. The prelaryngeal dissection starts inferiorly at the upper margin of the thyroid isthmus and extends superiorly to the anterior arch of the cricoid cartilage. The dissection extends superiorly into the tissue over the cricothyroid membrane and then over the anterior surface of the thyroid cartilage up to the thyroid notch. Nodal tissue may be residing in the indented cricothyroid membrane, so dissection in the area of the cricothyroid membrane must extend deeply enough to recognize and excise such Delphian nodes. The fascia over the cricothyroid muscle should be preserved, and all soft tissue should be dissected off this area preserving the perichondrium of the respective cartilages. Special care is taken to avoid injury to the cricothyroid muscles. There is often a small bleeder on the surface of the cricothyroid muscle, but cautery on the surface of the muscles is ill advised. Given the muscle’s thinness, such cautery injury would significantly disrupt muscular function with a possible postoperative pattern of dysfunction similar to superior laryngeal nerve paralysis. A pyramidal lobe, if present, is dissected as part of this initial prelaryngeal dissection and is reflected downward on to the thyroid. The orientation that is provided to the surgeon by this initial brief prelaryngeal dissection is helpful in that the exact midline, the anterior arch of the cricoid, and the cricothyroid muscles are all clearly identified, providing helpful anatomic information for later portions of the case (see Chapter 30, Principles in Thyroid Surgery).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


