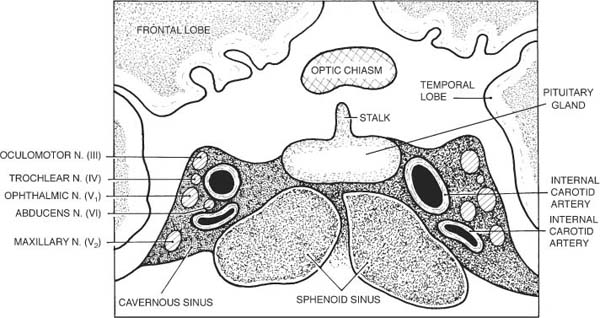
Chapter 33 The cavernous sinus (CS) is the skull base structure with the densest concentration of critical neural and vascular structures. Close proximity to the sella explains the high rate of endocrine dysfunction in cases of CS disease. There is a high prevalence of vascular etiologies for CS lesions. CS pathology can present in highly variable ways. Awareness of the multiple, unpredictable, and subtle manifestations of CS anatomy and pathophysiology is crucial for correct diagnosis.1 With the exception of benign, slow-growing tumors of the CS, the vast majority of CS lesions require urgent attention within 24 hours. Figure 33–1 illustrates a coronal view of the structures crossing the CS. The close proximity of the oculomotor, trochlear, abducens, trigeminal (V1–2), and sympathetic nerves to one another enables small mass lesions to cause multiple, simultaneous cranial neuropathies. The combination of multiple cranial neuropathies and vascular engorgement of the orbit or globe also represents a distinct presentation of CS pathology, given the close proximity of the previously-mentioned cranial nerves to the internal carotid artery and a rich venous sinus, which respectively feed and drain the ocular and adjacent structures. Clinical diagnosis is frequently suspected before radiologic diagnosis is achieved. Furthermore, even when CS pathology is strongly assumed, multiple neuro-imaging attempts are necessary to localize the lesion, with ever more precise imaging protocols. Not uncommonly, an imaging study is misread as normal by the unsuspecting radiologist. Conversely, it is not unusual for CS lesions to be missed clinically when first encountered. Table 33–1 lists the potential clinical neuro-ophthalmic permutations typically encountered in individuals with CS lesions.2 CS disorders may occur at any age. The specific demographic distribution of different types of lesions follows the demographics specific to each lesion. The spectrum of manifestations of CS pathology is particularly variable, although there are some important rules of thumb to follow. Pain is a frequent symptom of mass lesions involving the CS. The pain is typically visceral (deep and nonlocalizing) and may radiate to the hemicranium, orbit, or ear. Vascular lesions such as aneurysms, fistulas, and hemangiomata are usually painless unless the lesions are large and encroach on trigeminal sensory fibers. Visual loss is unusual unless the space-occupying lesion is so large that it impacts on the optic nerve or chiasm. This fact underscores why careful assessment of afferent visual function and visual fields is critically important even in seemingly uncomplicated cases of ophthalmoplegia. Any past history of an intermittent “red eye” linked to any cranial neuropathy of CS nerves should be considered suspect because dural arteriovenous CS fistulas may close off spontaneously. FIGURE 33–1 Coronal view of the cavernous sinus, sella, pituitary gland, stalk, and chiasm. Any history of fluctuating ptosis, changing pupil size, facial numbness, or diplopia, particularly if associated with known cranial nerve III, IV, or VI palsies, is suspicious for CS disease. A bruit audible to the patient suggests the presence of an intracavernous internal carotid artery aneurysm, which can expand or rupture, or a dural cavernous fistula. A history of dental procedure, chronic sphenoid sinusitis, endocarditis, or facial pustule should alert the clinician to the ominous possibility of a cavernous sinus abscess. Dramatic presentation with multiple cranial palsies (III, IV, V1–2, and VI) readily leads to correct localization of the lesion as involving the CS. The more subtle and partial manifestations of CS pathology warrant special emphasis. For instance, a cranial nerve VI palsy coupled with mild ipsilateral ptosis (forme fruste of a cranial nerve III palsy vs. oculosympathetic dysfunction) is suggestive of CS disease. Similarly, faint corneal hypesthesia (sign of V1 dysfunction) may accompany a cranial nerve IV palsy, as initial presentation of CS pathology. The following four presentations may lead to imprecise localization or delayed diagnosis: 1. Simultaneous cranial nerve III and IV palsy (IV nerve dysfunction is difficult to ascertain in the setting of an ipsilateral III nerve palsy), unless absence of the normally associated incyclotorsion on downgaze is carefully sought 2. A cranial nerve III palsy with ipsilateral oculo-sympathetic dysfunction (i.e., in third nerve palsy the pupil and eyelid are so dysfunctional that the ptosis and miosis present in oculosympathetic dysfunction are “hidden” within) 3. The presence of subtle corneal or facial hypesthesia is not always easy to detect when evaluating ophthalmoplegia. 4. Onset of aberrant regeneration of the third nerve without history of an acute cranial nerve III palsy (see Chapter 30) Table 33–2 describes four basic clinical presentations of CS pathology. Table 33–3 illustrates the differences between high-flow and low-flow arteriovenous fistulas involving the CS.
CAVERNOUS SINUS DISORDERS
URGENCY OF EVALUATION
DIAGNOSIS
ANATOMIC OVERVIEW
DEMOGRAPHICS
SYMPTOMS
Pain
Visual Loss
Red Eye
Ptosis, Pupils, or Diplopia
Bruit
Past Medical History
SIGNS
Red Flags
 Arteriovenous fistula between adjacent dural arterioles and the CS, misdiagnosed as conjunctivitis, scleritis, or inflammatory orbital disease (see Chapter 40)
Arteriovenous fistula between adjacent dural arterioles and the CS, misdiagnosed as conjunctivitis, scleritis, or inflammatory orbital disease (see Chapter 40)
 Low-flow carotid-cavernous sinus fistula missed because of reported “normal” computed tomography (CT) or magnetic resonance imaging (MRI). These neuroimaging studies are not very sensitive for detecting this condition
Low-flow carotid-cavernous sinus fistula missed because of reported “normal” computed tomography (CT) or magnetic resonance imaging (MRI). These neuroimaging studies are not very sensitive for detecting this condition
 Lymphoma, metastasis, or other neoplasm of the CS region misdiagnosed as Tolosa-Hunt syndrome
Lymphoma, metastasis, or other neoplasm of the CS region misdiagnosed as Tolosa-Hunt syndrome
 Cavernous sinus thrombosis (due to abscess or to hypercoagulable disorder) misdiagnosed as orbital cellulitis
Cavernous sinus thrombosis (due to abscess or to hypercoagulable disorder) misdiagnosed as orbital cellulitis
 Pupil-sparing cranial nerve III palsy in diabetic or nondiabetic individual not fully investigated
Pupil-sparing cranial nerve III palsy in diabetic or nondiabetic individual not fully investigated
 Failure to detect a cranial nerve IV palsy (lack of incyclotorsion in the affected eye) in the setting of a cranial nerve III palsy
Failure to detect a cranial nerve IV palsy (lack of incyclotorsion in the affected eye) in the setting of a cranial nerve III palsy
 It is difficult to diagnose oculosympathetic dysfunction within an ipsilateral cranial nerve III palsy.
It is difficult to diagnose oculosympathetic dysfunction within an ipsilateral cranial nerve III palsy.
VI nerve palsy/vascular congestion of the orbit and/or conjunctiva (“red eye”) • Look for arteriovenous fistula between dural arterioles and CS Cranial nerve VI palsy/ptosis and/or miosis • Partial Horner’s syndrome Pupil-sparing cranial nerve III and IV palsy • Caution: it is difficult to diagnose a cranial nerve IV palsy in the setting of a cranial nerve III palsy Any uni- or bilateral cranial nerve palsy of CS nerves + proptosis • Look for orbital invasion of CS region tumor through the optic canal Any uni- or bilateral cranial nerve palsy of CS nerves/optic neuropathy • Look for superiorly expanding tumor or aneurysm compressing optic nerve or chiasm Any uni- or bilateral cranial nerve palsy of CS nerves + chiasmal visual field defect • Look for superiorly or laterally expanding pituitary tumors Any uni- or bilateral cranial nerve palsy of CS nerves + endocrine signs/symptoms • Look for involvement of the adjacent pituitary gland Any cranial nerve palsy of CS nerves + orbital or facial pain • Look for involvement of pain sensitive trigeminal fibers in the CS Any cranial nerve palsy of CS nerves/contralateral hemiparesis/hemisensory loss and/or ipsilateral central retinal artery occlusion • Look for internal carotid artery thrombosis Bilateral cranial nerve palsy of CS nerves • Look for metastasis to CS or arteriovenous fistula between adjacent dural arterioles and CS Sudden onset proptosis + red eye + any cranial nerve palsy of CS nerves • Intracavernous internal carotid artery aneurysm rupture Severe unilateral orbitofacial pain and ophthalmoplegia (any cranial nerve palsy of CS nerves) Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|