Cataracts and Glaucoma
Marc Ellman
Jeffrey S. Schultz
Cataracts and glaucoma have common factors linking their development and progression. Both occur with greater prevalence with advancing age, and there may be a causal relationship between the two in some cases. In an attempt to clarify these two common ocular diseases, which are usually noted as being the second and third leading causes of visual impairment in the United States, a simple classification based on the types of glaucoma and associated cataracts is suggested. Both naturally occurring and iatrogenic factors under each classification can be defined, and it is hoped that this allows a rational approach to the management of the individual glaucoma patient with cataracts.
Hippocrates made no distinction between cataracts and glaucoma. According to the Greek writings, the term glaucoma defines a “glazed appearance without luster.” In the translation from Greek to Latin, and subsequently into Arabic, this disorder was termed “suffusio.” In the translation of the Arabic teachings back to Latin during the Middle Ages, the term cataract, meaning “waterfall,” was used in reference to suffusio. The term cataract was not known to the Greek writers. Subsequently, the distinctions between the two distinct diseases were first made and accepted during the 17th and 18th centuries. Since that time, they have been treated and approached as two separate but not mutually exclusive causes of human visual impairment.
CATARACTS AND CONGENITAL GLAUCOMA
INFANTILE GLAUCOMA
In infantile glaucoma (without other associated anomalies) there have been notations of cataracts before the patients underwent glaucoma surgery. However, in the majority of patients with infantile glaucoma without anomalies, there are no associated congenital cataracts. When lens opacities do occur, they typically occur after surgical intervention, including both angle and filtering surgery. During the surgery for resistant infantile glaucoma, if fistulizing procedures are necessary, occasionally the crystalline lens is lax and may have a tendency to dislocate; this accounts for the prolapse of the lens into the anterior chamber and the fistula that results in cataractous changes.
Another association of the lens with infantile glaucoma is microphakia. However, this may be a misnomer because of the buphthalmic enlargement of the globe.3 Fortunately, overall, uncomplicated infantile glaucoma without congenital or secondary cataracts is encountered most commonly.
Performing lensectomy during the first 4 weeks of life is associated with a higher risk of subsequent glaucoma than when surgery is performed at a later date. The reason for this association is unknown, but it seems reasonable to delay surgery until the infant is more than 1 month old. These children must undergo regular screenings for glaucoma because it can develop at any time.4 A conflicting report suggests that early cataract surgery (within the first 2 weeks of life) is associated with the fewest postoperative complications, including glaucoma, nystagmus, strabismus, and secondary membranes.5
ANIRIDIA
Aniridia is a rare congenital disorder characterized by bilateral iris hypoplasia. The incidence ranges from 1:64,000 to 1:96,000.6 Aniridia has been associated with glaucoma, cataracts, corneal opacities, foveal hypoplasia, optic nerve hypoplasia, and nystagmus.7 The term aniridia, signifying an absence of the iris, is a misnomer. In most, if not all cases of aniridia, a stump of tissue is present at the base of the iris.8 Six percent to seventy-five percent of patients with aniridia develop glaucoma, usually during late childhood or adolescence.6 The development of glaucoma results from progressive changes in the anterior chamber angle occurring during the first two decades of life.7 Although the angle was felt by many to be maldeveloped, glaucoma is most likely caused by a progressive mechanical rolling up of the iris stump (Fig. 1).9 Recently it has been discovered that patients with congenital aniridia have significantly increased central corneal thickness (average of 631.6 μm), thus potentially leading to inaccurate measurements of intraocular pressures.10 Unfortunately, aniridic glaucoma seems to be refractory to both medical and surgical treatments. Swanner and co-workers have proposed performing prophylactic goniosurgery in select aniridic eyes with early progressive angle changes, and have achieved encouraging results.7
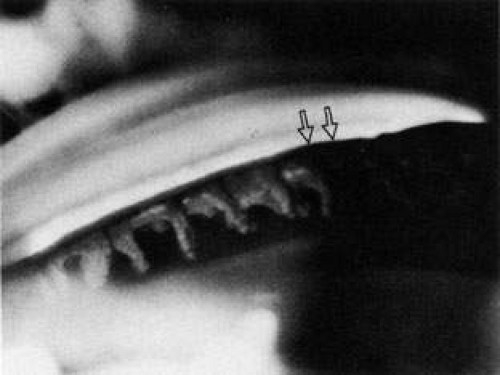 Fig. 1. Aniridia with stump rolled up (arrows). |
Cataracts may be present in a large number of aniridic patients, appearing with advancing age. They are most often developmental and are cortical or polar in location. Cataracts also may be present at birth owing to subluxed or dislocated lenses with adherence to the cornea endothelium. Any surgical procedures performed for aniridia, such as goniotomy for lysis of iris stump adhesions or filtration procedures, also may hasten or cause the development of cataracts. If a child’s vision is threatened, cataract formation in aniridia must be treated surgically in an effort to prevent amblyopia. Membranous cataracts and glaucoma formation also have been reported with aniridia.9
ANTERIOR SEGMENT ANOMALIES (IRIDOCORNEAL DYSGENESIS)
Congenital glaucoma can be seen in virtually the entire spectrum of anterior segment anomalies.
Axenfeld-Rieger syndrome commonly is associated with glaucoma and occasionally with cataracts as well. It is characterized by posterior embryotoxon (anterior displacement of Schwalbe’s line) combined with other ocular findings, such as attached iris strands, iris hypoplasia, and anterior chamber dysgenesis. Fifty percent of these eyes develop glaucoma in late childhood or adulthood.11 Cataracts also are occasionally found in these patients, although not as commonly as glaucoma. When present, lenticular changes vary from nuclear cataracts to anterior polar cataracts. Coloboma of the lens and ectopia lentis also may be present. The glaucoma usually develops before any significant cataract formation in the second or third decade of life. Of note, posterior embryotoxon can be seen as an isolated finding in 15% of normal patients.
Peter’s anomaly consists of a posterior corneal defect with opacity of the stroma. In some cases, iris strands adhere to the border of the corneal defect and in severe cases the lens itself adheres to the corneal defect. Peter’s anomaly is often the final result of defects such as congenital rubella and the Axenfeld-Rieger’s syndrome.11 Peter’s anomaly is the most severe of the spectrum of mesodermal dysgeneses, representing difficulties with cataracts and glaucoma often occurring at birth. Because of the severity of the problem, early cataract extraction may be necessary, possibly combined with corneal transplantation. In some instances, only corneal surgery is needed. Goniotomies are difficult to perform in these patients and may be of no benefit. Often the associated glaucoma has to be treated essentially as open-angle glaucoma; fistulizing operations may be necessary. Trabeculotomy for this condition has been associated with secondary cataracts.11
ASSOCIATED SYNDROMES
MARFAN’S SYNDROME
Marfan’s syndrome is an entity involving the musculoskeletal, cardiovascular, and ocular tissues. Ectopia lentis is seen in up to 70% of those afflicted. The lens also may be globular and have small cortical opacities. Glaucoma can be seen in up to 75% of people with Marfan’s syndrome, and often is congenital with anterior chamber anomalies. However, the glaucoma also can be caused by the forward dislocation of the anomalous lens, resulting in secondary angle-closure glaucoma. Miotics have been known to increase pupillary block with such lenses, giving a “paradoxic” angle closure. Treatment may be directed to mydriasis or peripheral iridectomy for this secondary angle-closure glaucoma. If the glaucoma is on the basis of angle anomalies, goniotomies have been attempted. Removal of the lens often results in vitreous loss and should be done only in a vision-threatening situation. Also, any time surgery is performed in a patient with Marfan’s syndrome, thromboembolic phenomena associated with anesthesia should be addressed as possible complications.
MARCHESANI’S SYNDROME
Weill-Marchesani’s syndrome can be associated with microspherophakia, lens subluxation, and angle anomaly associated with mesodermal dysgenesis.12 Congenital glaucoma can occur from the angle dysgenesis or a lens dislocation can give rise to a secondary angle closure. Although no reports of cataracts primarily occurring in this syndrome have been described, cataract formation can occur. Capsular tension rings may be a useful adjunct to cataract surgery in these and similar patients.13
LOWE’S SYNDROME
The oculocerebrorenal syndrome known as Lowe’s syndrome was first described in 1952.14 It is one of the two major syndromes with naturally occurring cataracts and congenital glaucoma (the other is rubella). The cataracts are bilateral and occur in virtually all reported cases.3 They are present prior to the fifth week of development in utero, with defects of the anterior, equatorial, and posterior subcapsular areas. This is a sex-linked inherited disease. Female carriers exhibit punctate opacities of the lens, which do not cause visual impairment (Fig. 2). Glaucoma, which is present in 60% to 70% of patients, is of an infantile variety with angle anomalies. Systemic manifestations include mental retardation and renal anomalies resulting in aminoaciduria.
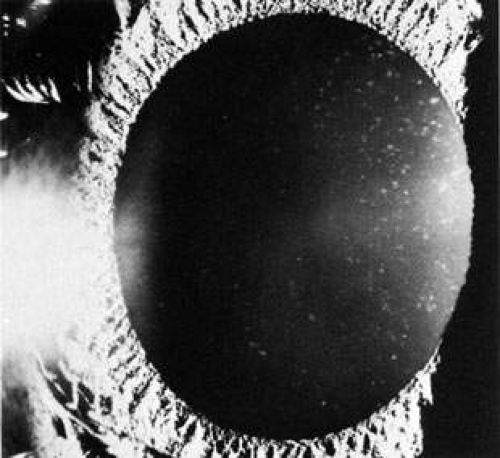 Fig. 2. Carrier state of Lowe’s syndrome. |
Ocular treatment usually is directed toward prevention of amblyopia by aspiration of cataracts and includes goniotomy for the glaucoma. It may be best to do the glaucoma surgery first, followed by lens aspiration. These eyes often respond poorly, with secondary hemorrhages resulting from goniotomies and, despite intensive therapy, blindness may result. Because of the systemic defects, including mental retardation and bone abnormalities resulting from secondary rickets, the overall prognosis is poor.
RUBELLA SYNDROME
The other major common syndrome in which infantile glaucoma is associated with congenital cataracts is rubella, also known as German measles. This is classified as a syndrome and is caused by an in utero rubella virus infection.3
In patients in whom the virus infection occurs during the first trimester of pregnancy, cataracts and glaucoma may both develop. If the infection occurs later, such as during the second trimester, only the glaucoma ensues, because by this time the lens has completed its embryonic capsular development. The glaucoma is frequently attributed to angle maldevelopment. Glaucoma occurs in 10% to 20% of those with rubella, whereas cataracts develop 10 times more frequently. The two may be mutually exclusive in some cases.
Heart anomalies, mental retardation, and hearing abnormalities are associated along with the ocular problems. These have to be considered in determining the time of surgical intervention. The cataracts are usually nuclear in location, but the cortical fibers often become involved secondarily. There have been reports of persistence of the virus in the lens, and this should be considered when performing aspiration of the lens in the infant.3 Spherophakia has been noted histologically and could conceivably result in pupillary block in rare instances. Continued development of the angle after birth could account for some of the reported cases of spontaneous resolution of the infantile glaucoma. An interesting observation of specks or pigmentation of the angle has been described in infantile glaucoma.15 This is in addition to the typical mottled pigmentation of the retinal posterior pole. A concomitant keratitis may complicate the picture when one is attempting to make a determination as to whether the pressure is elevated in infancy. This keratouveitis may rarely cause a secondary form of glaucoma. When cataracts and glaucoma occur together, the glaucoma usually should be treated before the cataract surgery.16 Secondary glaucoma can occur after cataract surgery. Despite modern surgical techniques, visual acuity after cataract extraction still remains poor in many of these patients.17
HOMOCYSTINURIA
Homocystinuria is caused by an autosomal recessive enzymatic defect, resulting in increased blood concentrations of homocysteine and methionine. Inability to metabolize homocystine is apparently caused by the absence of cystathionine beta-synthase.18 Aminoaciduria, mental retardation, a fair appearance, malar flush, and a stature similar to Marfan’s syndrome are possible systemic findings. The ocular findings include dislocated lenses in 90% of patients and often a pupillary block with secondary glaucoma.19 Cataracts are seen in 20% of patients, and glaucoma on a secondary or congenital basis is seen in approximately 10% of patients. A nonsurgical treatment consisting of a low methionine diet and supplementary vitamin B6 during the early weeks of infant life has been shown to significantly reduce the risk of ocular complications associated with this disease.19,20 Any surgical treatment must take into account the tendency for thromboembolic phenomena under general anesthesia in those with this disease.
CHROMOSOMAL ANOMALIES
Many chromosomal anomalies have been associated with ophthalmic disorders, including cataracts and glaucoma. These and other eye findings usually are seen together with other systemic signs such as deafness, heart defects, mental retardation, polydactyly, seizures, and cleft lip. Three of the more common chromosomal anomalies are trisomy 21, 18, and 13 (Down’s, Edward’s and Patau’s syndromes, respectively), which all can have ophthalmic manifestations.
Trisomy 21 affects approximately 1.69 in 1000 live births, making it the most common major chromosomal abnormality.21 Ophthalmic disorders are encountered in 60% of these patients, with congenital cataracts seen in approximately 3%, according to one source.22 A majority of Down’s syndrome patients have acquired lens opacities by adulthood as a complication of the premature senescence commonly seen.23
Trisomy 18 and 13 occur at much lower incidences than trisomy 21. Both have poor 1-year survival rates and only rarely do patients live into their teen years. Patients with these two disorders often suffer from a variety of physical developmental problems, including microphthalmia. If the microphthalmia is severe enough, it can lead to primarily nuclear cataract formation and persistent hyperplastic primary vitreous (PHPV), the latter sometimes associated with glaucoma. Surgical intervention for cataracts and glaucoma must be weighed in view of the overall poor prognosis of these and the many other chromosomal syndromes.24
PIERRE ROBIN’S SYNDROME
This syndrome of micrognathia, cleft palate, and glossoptosis has varied ocular anomalies, including congenital glaucoma and cataracts.25 Retinal detachment, high myopia, microphthalmia, and esotropia also are noted. Failure of the lower jaw to come forward with normal development at approximately the fourth month of fetal life could be associated with concomitant angle anomalies, resulting in angle maldevelopment at the same stage of embryogenesis. The cataracts consist of posterior subcapsular opacities. The glaucoma may require surgical intervention. When surgery is necessary, any heart defects must be considered when assessing risk. The prognosis is not poor, however, and attempts to prevent visual deprivation or blindness often are rewarding.
PERSISTENT HYPERPLASTIC PRIMARY VITREOUS
Persistent hyperplastic primary vitreous is a congenital anomaly in which the primary vitreous adheres to the posterior capsule of the lens, resulting in cataract formation. Glaucoma is not on the basis of angle anomalies, but usually is secondary to angle closure, because of either intumescence of the lens or hemorrhage from the persistent vessels on the posterior aspect of the lens. The glaucoma usually is approached as a secondary angle-closure glaucoma, with iridectomy or lens aspiration as the treatment of choice.
Retinopathy of Prematurity
In advanced retinopathy of prematurity, tissue from the retinal periphery can extend to the retrolental area, and this fibrovascular tissue can form a pseudotumor. As this progresses, total retinal detachment, secondary hemorrhage, swelling and edema of the mass, and the development of posterior synechia can occur. The anterior chamber can become shallow, resulting in secondary angle-closure glaucoma. This has been noted to occur in approximately 2% of patients. Lens aspiration may be performed to relieve the forward displacement of the iris-lens diaphragm (Fig. 3), and iridectomy usually is necessary. This is often done for cosmetic purposes to prevent enucleation, as vision is usually poor because of the underlying retinal problems.
 Fig. 3. Forward displacement of iris lens diaphragm and RLF (arrows indicate total central synechia). |
Angle-closure glaucoma after photocoagulation for retinopathy of prematurity has been reported.26 Confluent laser photoablation also has been associated with cataracts and other complications,27 mostly related to anterior chamber ischemia.28 Overall, the incidence of cataract formation in patients who have undergone argon laser photocoagulation for retinopathy of prematurity is approximately 1%. The occurrence of cataracts may be higher when persistent hyaloidal vessels are present on the lens.26
OTHER SYNDROMES
For a complete list of all the associated syndromes of lenticular opacities with infantile glaucoma, several other syndromes would have to be included that are beyond the scope of this text.
GLAUCOMA SECONDARY TO CONGENITAL CATARACT SURGERY
Both open and angle closure glaucoma can occur after congenital cataract surgery, although the open-angle variety occurs much more commonly. Open-angle glaucoma after congenital cataract surgery has been reported to occur in 3% to 41% of patients, depending on the series.29 The glaucoma may be of a congenital variety or may be associated with the cataract surgery itself. As opposed to congenital glaucoma, glaucoma after congenital cataract surgery is usually asymptomatic despite high intraocular pressures.30
There are many possible causes, including lens remnants with swelling, postoperative uveitis with occlusion of the pupil and peripheral anterior synechiae, and postsurgical flat anterior chambers with resultant synechia of the angle. Blockage of the pupil by vitreous may occur. Hyphema and, rarely, epithelial invasion of the anterior chamber have been noted. The uveitis may result from the presence of virus (as in the rubella syndrome), the surgical procedure itself, or retained lens particles. Measures directed toward each of these etiologies can be instituted. One report31 indicates that even though the angle remains completely free of any debris or inflammation, glaucoma may ensue after congenital cataract surgery. This glaucoma may result from underlying angle anomalies and could represent the coexistence of congenital glaucoma and cataracts. The postoperative appearance of the angle with an anterior iris insertion and prominent uveal scleral meshwork supports this. The time interval between the original cataract surgery and the onset of glaucoma is variable, with glaucoma occasionally occurring many years later.32 Thus, patients should be followed indefinitely for pressure stability, even if this requires examination under anesthesia.
Interestingly, aphakia may be a risk factor for open-angle glaucoma. Research suggests that placing a posterior-chamber intraocular lens during congenital cataract surgery significantly decreases the incidence of postoperative glaucoma, although the mechanism for this is unclear.33
Treatment for postcataract surgery glaucoma is usually the same as that for open-angle glaucoma, with medications being the initial modality of choice. Surgical intervention is shown to have limited success.34
TRAUMA
With blunt ocular trauma there may be an immediate rise in pressure or, if the trauma is of sufficient magnitude, a delayed rise years later in a small percentage of patients. The trauma may induce an angle recession,35 and in many of these traumatized eyes a contusion cataract ensues with either subluxation or dislocation of the lens. Rarely the lens may become swollen and intumescent, giving rise to phacolytic glaucoma, or, because of mechanical reasons, pupillary block glaucoma. Steroid use for iritis or other conditions after trauma is associated with an increased risk of ocular hypertension and cataract formation, especially if steroid use is prolonged.
If the lens anomaly is the cause of the glaucoma or visual impairment resulting from cataractous changes is present, removal of the lens may be indicated. A peripheral iridectomy in the presence of a subluxated clear lens may relieve the glaucoma. The treatment of angle-contusion glaucoma is essentially the same as for open-angle glaucoma, regardless of age.
If hyphema is present, a secondary glaucoma may result. This is more commonly seen in the eight-ball or total anterior chamber hemorrhage. In these patients, cataracts, either of posterior subcapsular or anterior subcapsular location, often are seen. Treatment is directed toward control of the bleeding. If blood staining of the cornea or intractable intraocular pressure ensues, irrigation of the chamber may be attempted. Various methods, including diathermy, fibrinolysis, and cryoextraction of the clot, have been tried in the treatment of this difficult problem.31 Essentially, treatment has to be individualized because there is no commonly accepted mode of therapy.
CATARACTS AND PRIMARY ANGLE-CLOSURE GLAUCOMA
The lens plays a vital role in primary angle-closure glaucoma. It is involved in the physiologic block of forward aqueous flow and, in turn, can develop opacities as a result of the acute rise in pressure. Because of the forward position of the lens in eyes with genetically determined shallow anterior chambers, the resistance to aqueous flow caused by apposition of the iris to the lens lifts the peripheral iris forward toward the trabecular meshwork and often causes angle closure. In addition to the anterior position of the lens in such eyes, intumescence or swelling of the lens or a slightly anteriorly dislocated lens may cause the same problem. This latter factor is discussed in the section on secondary angle-closure glaucoma and cataracts.
ANGLE-CLOSURE GLAUCOMA CAUSED BY PUPILLARY BLOCK
Cataracts are often the cause of angle-closure glaucoma resulting from pupillary block. Lenticular opacities may appear and are felt to be characteristic of this variety of glaucoma. They have been called glaukomflecken, are of a subepithelial nature, and usually are found underneath the anterior capsule.36 The presence of these punctate opacities in quiet eyes usually indicates previous attacks. However, it has been noted that they may occur in patients with glaucoma with high intraocular pressure associated with contusion injury or iridocyclitis.37,38 After an attack, these opacities may progress from multiple discrete subcapsular spots to round or oval densities, usually located in the pupillary area. Apparently, these result from necrosis of the subcapsular epithelium as a result of the high intraocular pressures.39 However, these are not related to all cases of angle closure and seem to be dependent on the level of pressure, the number of previous attacks, and, possibly, the duration of the attacks. In addition to these lens opacities, senile cataracts can be precipitated or, even more often, aggravated by acute angle-closure episodes.
If the cataract is of such a nature to decrease vision significantly, the treatment is cataract removal and iridectomy. It is well known that treatment with parasympathomimetic agents, such as pilocarpine, has been implicated in the formation of lens opacities,40 although this may be related to older studies of its previous long-term use in open-angle glaucoma rather than short-term use in angle-closure glaucoma. Miotic therapy is discussed in further detail later in this chapter.
A peripheral iridectomy is the treatment of choice for pupillary block glaucoma. Most iridectomies today are performed by laser, although surgical iridectomies are still performed in many parts of the world. The incidence of lens opacities after surgical peripheral iridectomy is increased, usually related to direct injury from a surgical instrument. Meticulous care at the time of surgery may decrease the incidence of direct traumatic cataracts.38 Prolonged flat anterior chambers occurring after peripheral iridectomy also may lead to a higher incidence of cataracts.
Although the advent of laser iridotomy has greatly decreased the incidence of cataract development compared to surgical iridotomy, laser iridotomy (Fig. 4) also can cause lenticular changes. Several reports have demonstrated small lens opacities appearing at the site of the laser beam after laser iridotomy (Fig. 5),36,41,42 but no progression of these opacities has been described. Zonular rupture can occur from the laser as well.43 One case report describes an “exploding” cataract with posterior capsular rupture and release of cortical material into the vitreous following a YAG laser peripheral iridectomy.37
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


