Cataract Extraction in Patients with Glaucoma
Ronald L. Fellman
Richard J. Starita
David G. Godfrey
Arvind Neelakantan
Cataract surgery in the setting of glaucoma requires proficiency far beyond routine lens extraction. The preoperative dialog between patient and physician should center on defining the degree of nerve and field damage and how to stabilize it, secondarily how to best remove the cataract. A blend of skills is often necessary to obtain the ultimate goal of both improved visual acuity and optic nerve preservation. Patients must understand that the knowledge necessary to accomplish this objective is straightforward for some cases and exceedingly complex in others. This chapter provides a framework for achieving this worthy goal.
The care of a patient who has both cataract and significant glaucomatous damage must be in many ways totally different from that of a person with cataract uncomplicated by glaucoma. The failure to appreciate this difference may lead to unnecessary morbidity, profound loss of vision due to worsening nerve damage, or suboptimal visual performance due to inappropriate IOL selection for the glaucoma patient.
In years past, the surgical options for conjoint cataract and glaucoma were straightforward: either a combined lens extraction with filtration procedure or staged. Today, the benefits of small-incision cataract surgery alone with IOL implantation are extraordinary for many glaucoma patients. The capability to immediately improve vision, alleviate astigmatism with a toric IOL, improve contrast sensitivity with an aspheric IOL, lower intraocular pressure (IOP) long term by opening the angle and improving outflow and sparing valuable conjunctiva for future glaucoma surgery is a surgical triumph for these patients. Consequently, a stable glaucoma patient on one or two medications with mild disc damage and symptomatic cataract may no longer require a combined or staged procedure. This is a vast improvement over 11-mm incisions that were common a decade ago (Fig. 16.1)
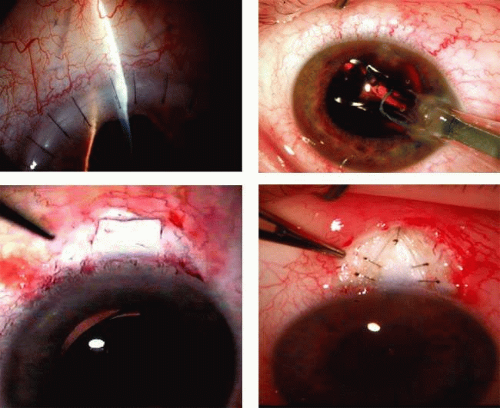 FIGURE 16.1 The anatomic advantage of small incision cataract surgery for the glaucoma patient. A: Long-term bleb function with a large cataract incision is difficult to achieve with either ECCE-trabeculectomy or trabeculectomy followed later by ECCE. This bleb failed to form sufficiently when combined with large-incision ECCE. The inflammation, bleeding, and long-term wound healing with stimulation of fibroblasts associated with this technique are more likely to cause bleb failure. In addition, the increased iris manipulation necessary to deliver the nucleus and subsequent iris repair adds to the long-term breakdown of the blood aqueous barrier. Two-site phacotrabeculectomy (B, C), has the advantage of modern-day small-incision cataract surgery combined with separate site trabeculectomy. The incision size is one-third the size of the standard clear corneal ECCE. The inflammation is less, and cataract wound healing is essentially confined to the temporal area. Visual rehabilitation with phacoemulsification and foldable IOL is much faster. The trabeculectomy is performed in an entirely different site, well away from the wound healing associated with temporal phacoemulsification. The likelihood of long-term filtration is greater than with ECCE-trabeculectomy. D: The surgeon also has the option of single-site phacotrabeculectomy with foldable IOL. Both the lens extraction and the trabeculectomy are performed through one small 3.5-mm limbal incision. |
Patients who require combined surgery are not always optimal candidates for phacotrabeculectomy. Today, there may be more favorable options especially when it is prudent to try and avoid the perils associated with trabeculectomy. A growing number of patients with mild to moderate glaucoma may only need an IOP in the mid teens and are candidates for non-bleb-related glaucoma procedures that are less risky. This is especially germane with an ever-increasing aging population with worrisome risks factors related to cardiovascular, hematologic, diabetic, neurologic, and psychosocial factors. All of these debilitating diseases may complicate recovery from a glaucoma surgical procedure.
For example, many patients with symptomatic cataract and uncontrolled IOP with mild to moderate glaucoma who require IOP control in the mid to high teens1 may be candidates for not only trabeculectomy, but for nonpenetrating glaucoma surgery (Fig. 16.2) Phacoemulsification with viscocanalostomy or deep sclerectomy is a nonpenetrating procedure with the added benefit of IOP control with less worrisome bleb formation. Canaloplasty is a new procedure designed to tension and dilate Schlemm’s canal improving outflow through the diseased outflow channels and works extremely well in conjunction with phacoemulsification. Phacotrabeculotomy is another method of improving outflow without a bleb. Phacogoniosynechialysis is a popular method of increasing outflow in narrow angled eyes with pre-existing peripheral anterior synechiae (PAS). PhacoECP is a convenient minimally invasive means of lowering IOP in patients requiring combined cataract and glaucoma surgery. Endoscopic cyclophotocoagulation (ECP) allows direct visualization of the ciliary body processes and may easily be combined with phacoemulsification. Thus there are a number of non–bleb-related procedures that may be combined with cataract extraction under the appropriate circumstances. These procedures would not be expected to reduce IOP into the single-digit range.
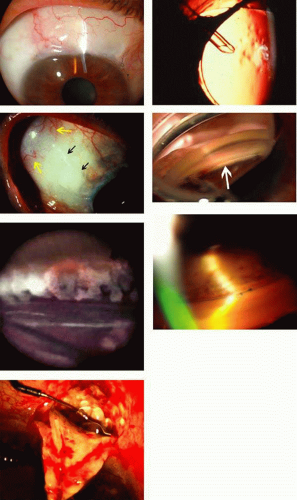 FIGURE 16.2. Incisional glaucoma surgical options for combined cataract and glaucoma procedures. A: Trabeculectomy remains the gold standard for IOP reduction in an eye with a pristine blood aqueous barrier and virgin conjunctiva. Trabeculectomy lowers IOP by diverting aqueous humor into the subconjunctival space forming a filtering bleb under the upper lid. However, when anterior segment anatomy is altered, conjunctiva violated, or the blood aqueous barrier disrupted, trabeculectomy is less effective. B,C: Glaucoma drainage implants are a viable alternative to filtration especially in eyes with an altered blood aqueous barrier or anterior segment anatomy. The tube shunts fluid from the anterior chamber (B), to an equatorial bleb promoting device (C) (yellow arrow). The black arrows point to the tube that is covered by a patch graft to prevent tube erosion. D: Trabeculotomy cleft, white arrow, created with the Trabectome® instrument (NeoMedix, Tustin, CA). A micro-bipolar cautery electrode creates an opening in the canal and the procedure is easy to combine with cataract surgery, all through the same incision. Trabeculotomy improves trabecular outflow (see section on Trabeculotomy). E: Endoscopic cyclophotocoagulation (ECP) is a very easy method of reducing aqueous production by direct ciliary body ablation that is performed in conjunction with phacoemulsification, long term the eye remains quiet without flare or cell. The white area represents coagulation and shrinkage of the ciliary body processes, and the red circle is the aiming beam on the adjacent process. F: Canaloplasty is a form of nonpenetrating surgery designed to reduce IOP by suture tensioning in the canal along with viscodilation. The two blue 10-0 prolene sutures are easily seen in the canal. G: Deep sclerectomy and viscocanalostomy are similar forms of nonpenetrating surgery that may be combined with lens extraction. These nonpenetrating procedures require additional skills that are not typically involved with trabeculectomy such as fashioning two scleral flaps and locating Schlemm’s canal. There are other related canal procedures currently under investigation. Canal surgery is the current frontier in innovative glaucoma surgery. |
Patients with advanced disc damage, progressive glaucoma at any stage, and/or complex cataract present a much more challenging situation. They are far from elementary and present the ophthalmic surgeon and patient with many demanding situations (Fig. 16.3). The knowledge and wisdom necessary to achieve a favorable outcome in these difficult cases requires a fusion of higher level preoperative, intraoperative, and postoperative decision-making skill. This situation is seen most commonly in patients requiring combined procedures who have advanced optic nerve damage complicated by any one or more of the following: systemic disease especially diabetes mellitus, secondary glaucomas, anterior segment anomalies, miosis with posterior synechiae, pseudoexfoliation, anticoagulation, keratopathy, and complex cataracts. Society’s perception of cataract surgery as a quick-fix operation with a rapid return of splendid vision is often not true for these patients who invariably perceive they are undergoing “routine” cataract surgery.2 Optic nerve damage or other concomitant eye diseases may limit visual recovery after flawless combined cataract and glaucoma surgery, leaving a disappointed patient. Moreover, glaucoma filtration surgery causes astigmatism and slows improvement in visual acuity.3,4 Informed consent with special emphasis on postoperative complications is especially important in glaucoma patients undergoing high-risk filtration surgery. Surgeons and their staff must spend additional time counseling patients who require filtration surgery due to the myriad of potential complications inherent to this procedure, which are far greater than routine lens extraction. Chair time also increases significantly due to the discussion related to the best IOL for the patient’s particular needs.
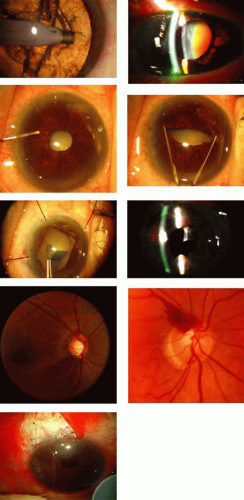 FIGURE 16.3. Complex cataract and disc damage. A: Cataract extraction by nuclear disassembly, as in divide and conquer technique, in an eye with mild to moderate nuclear sclerosis is a routine occurrence. Clear corneal phacoemulsification in itself may significantly reduce IOP in normal and glaucomatous eyes. B: However, this dense brunescent cataract in an eye post angle-closure attack, with iris atrophy and shallow chamber requires a much more complicated approach. These complex cataractous eyes may develop intraoperative aqueous misdirection requiring Mannitol or acetozolamide, or even intraoperative ocular decompression. Cataract extraction with IOL implantation is far from routine in these eyes. C–E: Many cases require iris or capsulorrhexis retractors, pupil stretch, or vision blue dye to adequately see the capsule. Phaco-chop techniques may be helpful, as well as the ability to convert to a larger incision ECCE. Special phacoemulsification tips such as the Kelman will improve the ability to emulsify this dense cataract. F: Even with perfect technique, the bag complex may dislocate or decenter after years and repositioning may be difficult. G,H: Eyes with fragile discs demonstrated by advanced cupping or disc hemorrhage require aggressive IOP control, especially when combined with cataract extraction, such as seen in I, a combined phacotrabeculectomy. |
Small incision cataract surgery combined with continuous curvilinear capsulorrhexis (CCC), improved management of miotic pupils, a better understanding of intraoperative floppy iris syndrome (IFIS), divide-and-conquer nucleofractis phacoemulsification, clear corneal incision, capsular tension rings,5 phaco-chop, improved viscoelastic, and foldable intraocular lenses greatly improves cataract surgical outcomes. The use of dyes to stain the anterior capsule (Fig. 3E) in patients with an absent red reflex as in a white or dark brunescent cataract improves visualization for anterior capsulorrhexis. These techniques, in combination with anti-metabolite-assisted fornix-based filtration surgery (GFS), and postoperative scleral flap suture lysis or releasable sutures, improve results for glaucoma patients with surgical cataracts and uncontrolled IOP.
Small-incision cataract surgery, however, is not appropriate for every glaucoma patient. The surgeon must be facile and maintain skill in all branches of cataract surgery, including intracapsular cataract extraction (ICCE), manual nuclear expression with extracapsular cataract extraction (ECCE), and phacoemulsification of soft or hard nuclei. A fusion of these skills is necessary because a subluxated rock-hard nucleus may require ICCE, the nucleus may be too dense for emulsification requiring manual expression, the cornea may be cloudy preventing phacoemulsification, or the surgeon may find it necessary to convert to ECCE techniques during small-incision surgery.
This chapter provides a framework to help the surgeon caring for a patient with both cataract and glaucoma decide when to perform a cataract extraction alone, a glaucoma procedure alone, or a combined cataract-glaucoma procedure. The case studies found later in this chapter emphasize the order and timing of surgery for patients with both cataract and glaucoma. Furthermore, techniques that are especially appropriate when performing cataract extraction in patients with glaucoma will be presented in detail with the premise that any additional surgical step carries with it the increased risk of complication.
Guiding Principles
Glaucoma is a disease in which ocular tissues become damaged by IOP that is higher than the tissues can tolerate. Glaucoma is not a single condition; the word encompasses a variety of entities of different pathogenesis and different intensity. Common to all the glaucomas is the end organ damage of an optic neuropathy with characteristic structural changes to the optic disc with associated visual dysfunction. Several systemic factors6 may also play a role in the progression of glaucoma including cardiovascular abnormalities, autonomic dysregulation, immune complex disease, sleep apnea, and a host of other factors. The total management of the glaucoma patient in the 21st century includes not only the eye but also a systemic and psychosocial perspective that involves adherence and compliance.
Knowledge of the basic principles related to the effects and side effects of cataract extraction in patients with glaucoma is essential if the surgeon is to choose a course that is most appropriate for each individual case. Some of these principles are known by all, and many are established but not well appreciated. Some of the principles that follow are neither well known nor well established but are based on our personal experience or the experiences of those whose clinical judgment appears to us to be sound. Principles not given a supporting reference usually fall into this category. An evidence-based approach to the literature is emphasized where appropriate and thoroughly reviewed.7,8
Clinical Aspects of Optic Nerve Head Damage
Short-term, moderate elevation of intraocular pressure is not likely to affect a healthy optic nerve.
Optic nerves vary in their ability to resist the damaging effects of intraocular pressure.9,10,11,12,13,14,15,16,17 Normal optic nerves of healthy adults are not usually damaged by intraocular pressures below the diastolic ophthalmic artery pressure (around 30 to 35 mm Hg) unless the pressure persists for a minimum of 2 to 3 months. The exception is patients with sickle-cell disease.18,19,20 In addition, healthy optic nerves in some healthy adults can withstand short-term (perhaps up to 2 weeks) elevations of IOP below the systolic level of ophthalmic artery blood pressure (average, 70 mm Hg) without sustaining apparent damage (with the exception of sickle-cell abnormalities). Intraocular pressures greater than systolic retinal artery blood pressure damage all optic nerves permanently when such an elevation persists for more than a few minutes.
Glaucomatous optic nerves are more likely to be damaged by elevated intraocular pressure.
There are a variety of factors associated with IOP-induced visual field loss; most notable is ocular perfusion pressure.21 Optic discs already compromised by glaucomatous disease or other optic neuropathies are at greater risk for further damage and can be permanently damaged by increases in IOP of relatively small magnitude and short duration. Precise data are lacking, but pressure elevations as small as a 50% increase (i.e., 20 to 30 mmHg) for 1 month can be expected to cause a permanent worsening of optic nerve function in patients with serious disc disease prior to the pressure elevation.
Optic discs that are badly damaged by glaucoma (“sick discs”) can be further damaged permanently by pressure elevations as short as: 1 day or less when the pressure elevation is in the range of 50 mm Hg or more, 1 day when intraocular pressure is 30 to 50 mm Hg, or several days when the IOP spike is in the range of the diastolic ophthalmic artery blood pressure.
The visually damaging pressure level of intraocular pressure can be estimated.
The pressure at which a patient develops a hemorrhage of the optic disc or at which progressive disc damage or visual field loss occurs prior to cataract extraction gives a rough estimate of the level of IOP the optic nerve is unable to tolerate. This pressure provides a baseline to use for predicting future damage. For example, a patient whose intraocular pressures are fairly consistent at the mid-teen range with progressive damage needs an IOP in the low teens to prevent or decrease further damage. In contrast, a patient who develops a disc hemorrhage when intraocular pressures are averaging around 25 mm Hg probably has an optic disc that is more resistant to the damaging effects of IOP. This patient may do well with a long-term IOP of 15 to 20 mm Hg. These factors help the comprehensive ophthalmologist decide how high and how long a postoperative intraocular pressure spike is tolerable. Under estimation of IOP may occur in a patient with a thin cornea, the combination of underestimation along with a tenuous postoperative state may rapidly exacerbate nerve damage. Preoperative knowledge of central corneal thickness, disc damage, field damage, and the damaging IOP level allow the formulation of a reasonable safe surgical plan. This is highly recommended for all glaucoma patients.
Pseudo-pits of the optic nerve are a sign of a pressure-sensitive optic nerve.
Visual Field Loss and Its Relation to Cataract–Glaucoma Surgery
Visual field defects of a diffuse type are generally characteristic of patients whose optic nerves are relatively resistant to the damaging effects of intraocular pressure.24,25,26 Dense paracentral defects, however, are characteristic of patients whose optic discs are more sensitive to the damaging effects of intraocular pressure.27,28
Factors Affecting the Likelihood of Visual Field Damage
Patients with visual field loss that extends into fixation are more likely to have their visual acuity damaged by postoperative pressure elevations than are patients whose field defects spare the area of fixation. Appropriate preoperative planning, such as combined or staged surgery to eliminate damaging postoperative pressure elevations is essential for this group of patients. In addition, patients with preoperative visual field defects that split into fixation may experience a sudden decrease in acuity associated with an otherwise uncomplicated intraocular surgery. This phenomenon of wipeout occurs in 1% to 5% of cases.29,30, 31,32 “Wipeout” also appears to be related to severe postoperative hypotony and is more common in patients whose postoperative intraocular pressures are less than 5 mm Hg. Hypotony maculopathy is a well-recognized cause of visual loss following filtration surgery. Every conceivable effort should be made to avoid long-term maculopathy and keratopathy due to excessive filtration. In spite of a surgeon’s best effort, this complication will always be an issue with filtration surgery.
The Effect of Cataract on Automated Perimetry
Nonglaucomatous patients with progressive nuclear sclerosis develop a generalized depression in their field. This is detected during automated perimetry on the Humphrey Field Analyzer, HFA, and is expressed with software analysis on the glaucoma hemifield test as a generalized depression. This generalized depression is also reported as an abnormal global index expressed as decreased mean deviation. Glaucoma patients develop both generalized and/or localized visual field defects. Nuclear sclerosis causes a worsening of both preexisting generalized and localized glaucomatous field defects. A cataract by itself does not produce a dense scotoma.33 Worsening of a scotoma without an increase in generalized depression of the rest of the field is not due to a nuclear cataract. The best method of determining whether field progression is due to cataract or glaucoma is to dilate the pupil and compare the optic disc to an earlier less cataractous state. A thorough understanding of normal and abnormal visual field indices related to automated perimetry is essential in order to reliably interpret automated visual fields.34
Following uncomplicated cataract extraction in glaucoma patients, there is an overall improvement in mean deviation,33,34,35,36,37 and foveal threshold38; however, dense paracentral scotomas may appear deeper as noted by a worsening of the corrected pattern standard deviation, (CPSD).39 This worsening of CPSD appears to be less with phacotrabeculectomy augmented with Mitomycin C.40 This statistical worsening of the CPSD is likely due to raising the height of the island of vision, whereas the floor of the scotoma remains the same.41 The SITA algorithm for threshold perimetry is commonly used today. After lens extraction in patients with glaucoma, mean deviation improves but pattern standard deviation remains similar.42
Anterior-Segment Tissue Alterations Secondary to Glaucomatous Disease Require Additional Planning
The anatomic and physiologic alterations of glaucomatous eyes are protean.
Recognition of these alterations facilitates treatment of the disease process. A severe attack of angle-closure glaucoma causes corneal endothelial damage, cataract, trabecular damage, posterior synechiae, and iris necrosis (Fig. 16.3B). These tissue alterations will alter the surgeon’s approach to cataract surgery. Corneal decompensation after otherwise uncomplicated cataract extraction is common in patients having sustained a severe attack of acute angle-closure glaucoma.43 Surgeons contemplating cataract extraction in these eyes naturally desire to avoid as much corneal trauma as possible. Glaucoma patients with concomitant corneal disease such as iridocorneal endothelial syndrome (ICE) should be informed of likely corneal decompensation associated with glaucoma or cataract surgery.
The atonic pupil that follows a severe angle-closure attack is fixed and dilated. This pupil alteration may cause the surgeon to choose an intraocular lens (IOL) with a larger optic to prevent glare and monocular diplopia associated with the larger pupil. An atonic mydriatic pupil may be repaired during cataract surgery using a McCannel suture circlage approach.44 Patients should be instructed that visual aberrations associated with abnormal pupils from glaucomatous disease might alter visual performance post cataract surgery. Eyes with short axial lengths typically have a very shallow anterior chamber. This makes it even more difficult for the surgeon to work, especially when introducing any instrument into the eye. In addition, eyes with unusual axial lengths require more sophisticated IOL calculation formulas; otherwise, undesirable postoperative hyperopia occurs.
The iris of glaucoma patients is usually abnormal.
Widespread glaucomatous iris abnormalities include abnormal blood vessel permeability, flaccid iris tone, rigid or atrophic muscles, and friability. Pigment dispersion, breakdown of the blood-aqueous barrier, and hyphema at the time of surgery and postoperatively are common in these eyes. The lens capsule and zonules tend to be more fragile in patients with glaucoma than in those without glaucoma.45,46 The problem is most severe in those with advanced glaucoma who have been treated most intensively. Surgery is extremely complicated in the exfoliation syndrome because of zonular dehiscence, loose zonules, sticky cortex, and altered blood aqueous barrier. The lenses of patients with long-standing glaucoma and advanced cataracts are often partially “loose” even though they do not appear frankly dislocated. Long-term parasympathomimetic drug therapy produces leaky iris vessels with breakdown of the blood-aqueous barrier, posterior synechiae, peripheral anterior synechiae, and rigid miotic pupils. Inability to sufficiently dilate the pupil is a leading cause of vitreous loss at the time of cataract surgery. The final outcome of cataract extraction is worsened by preoperative long-term use of parasympathomimetic drugs because the pupil does not dilate well, the iris is more likely to bleed when traumatized, breakdown of the blood-aqueous barrier is excessive,47 and there is an increased likelihood of vitreoretinal interface problems.
The conjunctiva of patients with glaucoma is often abnormal.
The tissues of patients with glaucoma who have been treated medically for glaucoma are not as healthy as the tissues of patients who do not have glaucoma.48 The conjunctiva undergoes several tissue alterations due to topical antiglaucoma therapy. These tissue alterations lead to higher intraoperative complications and long-term filtration failure, but may be partially reversed with preoperative corticosteroids.49
IOP Changes Associated with Lens Extraction
Intraocular pressure rises during the first 24 hours following cataract extraction.
Cataract extraction with complete wound closure is associated in most cases with an elevated IOP. Occasionally, the IOP may be low, less than 5 mm Hg, 30 minutes after surgery, even with an intact wound, although the majority of the time, the IOP is elevated.50 It is critical to close the clear corneal incision with a suture when combined with trabeculectomy because low IOP may predispose to break down of wound architecture and subsequent leak.
The greater the inflammation and the more seriously damaged the outflow channels, the greater the intensity and rise of intraocular pressure after cataract extraction. Viscoelastic substance,51 severity of pre-existing glaucomatous trabecular damage, suture deformation with trabecular collapse, cortical and pigmentary debris, blood components, breakdown of the blood-aqueous barrier, and altered prostaglandin metabolism all factor into the decrease in outflow facility. The severity, height, and duration of IOP rise are worse if the surgery is complicated by vitreous loss. The highest intraocular pressure after either ICCE or ECCE appears to occur around 6 hours after surgery.50,51,52,53,54 As many as 15% of nonglaucomatous patients undergoing uncomplicated ECCE with PCIOL develop pressure spikes greater than 40 mm Hg within 24 hours of surgery without prophylactic pressure-lowering drugs.55 On the first postoperative day, as many as 55% of patients post-ECCE with a PCIOL develop intraocular pressures in excess of 25 mm Hg.56 This occurs even when viscoelastic material is removed at the time of surgery but without the advantage of pressure-reducing drugs used at the conclusion of surgery.
Even in normal eyes, mean IOP rises approximately 30% on the first day after uncomplicated phacoemulsification with 6% of patients experiencing IOP’s greater than 30 mm Hg.57 In nonglaucomatous eyes, the highest IOP elevation occurs 2 to 8 hours after uncomplicated phacoemulsification, and is dependent on the type of viscoelastic.58 Intraocular pressure elevations during the first postoperative day are common following uncomplicated phacoemulsification with both scleral or clear corneal incisions59 and the majority of IOP spikes may be detected between 30 minutes and 2 hours after surgery.60 After phacoemulsification and foldable IOL implantation, the immediate postoperative IOP increase is higher in eyes undergoing sclerocorneal incisions compared to clear corneal incisions.61
Acute Pressure elevation in glaucomatous eyes after cataract extraction is much worse and of longer duration than in nonglaucomatous eyes.
Postoperative pressure spikes may lead to blindness and visual field loss in glaucomatous eyes.62 These pressure elevations are a particular problem in patients unable to tolerate carbonic anhydrase inhibitors (CAI) or topical beta-adrenergic-blocking agents. Several measures can be taken to control and monitor immediate postoperative intraocular pressure rises in all eyes undergoing cataract extraction:
Avoid excessive intraocular trauma.
Inject intracameral carbachol or acetylcholine to enhance trabecular outflow (avoid in uveitis).65
Perform peripheral iridectomy in patients with diabetes mellitus, high hyperopia, rubeosis iridis, intraoperative vitreous loss, anterior chamber IOL, and uveitis in order to avoid pupillary block glaucoma.
IOP check 30 minutes after cataract extraction is insufficient to detect elevated IOP66
Topical carbonic anhydrase inhibitors (CAI) reduce postoperative IOP better than prostaglandin analogues67 and prostaglandin analogs lower IOP better than placebo68
Prostaglandin analogs are not as effective in the immediate postoperative period as combination fixed aqueous suppressants71 and are a risk factor for the development of cystoid macular edema.70,71,72,73,74
Use of topical parasympathomimetic drugs such as 2% pilocarpine if inflammation is not excessive.
Use of nonselective alpha-agonist short-term, pre- and postoperatively,75,76 is less effective after phacoemulsification.77
Consider serial anterior chamber paracentesis when pressure is dangerously high.80
Postoperatively, patients with badly damaged optic nerves may lose considerable visual acuity and/or visual field during the above pressure-lowering efforts. Patients with mild-to-moderate glaucoma damage generally tolerate the above procedures without significant visual loss. Patients with badly damaged optic nerves require additional planning in order to prevent loss of vision. This may require treatment by combining cataract and glaucoma surgery or staging the procedures with filtration surgery followed later by cataract extraction. Patients with advanced nerve damage require more frequent postoperative visits starting as early as 2 to 6 hours after surgery in order to detect the first potentially damaging postoperative IOP spike. If the surgeon is not comfortable with a combined procedure and the IOP is dangerously elevated, a filtration procedure alone may be preferable to stabilize the glaucoma followed later by lens extraction.
Prior to cataract extraction, the surgeon should explain there may be a need to return to the operating room on an emergent basis to reduce IOP. The confident surgeon will return to the operating room when needed without hesitation to save a badly damaged nerve.
Argon laser trabeculoplasty (ALT) tends to be less effective in aphakic or pseudophakic patients than in phakic patients.
Utilize laser trabeculoplasty prior to cataract extraction to gain better control of glaucoma in preparation for cataract surgery. If indicated, ALT is more effective when performed prior to lens extraction; in addition, postoperative pressure spikes are dampened in these eyes.79,80,81,82,83 Following effective ALT, decrease glaucoma medications in anticipation of cataract extraction allowing room to resume drugs after surgery if IOP is problematic. Argon laser trabeculoplasty is effective in approximately two-thirds of patients with open angles post failed filtration surgery.84 Selective laser trabeculoplasty (SLT) appears similar to ALT in reducing IOP prior to lens extraction while maintaining IOP control in the postoperative period.85
Cataract extraction alone, after the initial pressure spike, often leads to long-term lowering of intraocular pressure, most notably after clear corneal phacoemulsification.
This lowering of intraocular pressure occurs with both ICCE and ECCE surgery. The magnitude of the pressure lowering appears to be increased in patients having PCIOL implantation at the time of the cataract extraction.84,85,86,87,88,89 This decrease in IOP is apparent as far out as 5 years from clear corneal phacoemulsification in open-angle glaucoma patients, glaucoma suspects, as well as normal eyes.90 The reduction in IOP associated with phacoemulsification is greater than ECCE. Stable, medically controlled glaucoma patients who undergo uncomplicated clear corneal phacoemulsification show a significant reduction in the number of postoperative glaucoma medications at 1 year, particularly in patients with pseudoexfoliation syndrome.91,92 Even nonglaucomatous patients with normal IOP prior to uncomplicated clear corneal phacoemulsification experience reduced postoperative IOP.93 A similar IOP lowering effect is seen at 5 years with phacoemulsification through a scleral approach.94 The mechanism of IOP lowering after phacoemulsification is unclear. However, patients with a reduced preoperative facility of outflow show a significant improvement in outflow facility following phacoemulsification at 1 year.95 Long-term IOP control after phacoemulsification with a foldable IOL is slightly better with a clear corneal approach compared to sclerocorneal.96 Uneventful clear corneal phacoemulsification with foldable IOL not only reduces IOP long term but also reduces the need for glaucoma medications.97 IOP reduction correlates with the degree of preoperative shallowing of the anterior chamber.98
IOP Changes Associated With Combined Cataract and Glaucoma Surgery
Immediate IOP control after combined cataract-glaucoma surgery is better than cataract extraction alone.
Immediate IOP control after combined procedures is especially beneficial in patients with advanced disc damage who are already on maximal medical therapy. Phacotrabeculectomy with eventual bleb failure has a similar long-term pressure-lowering efficacy of phacoemulsification alone. However, the combined procedure that eventually fails is not a complete failure if the optic nerve damage from the immediate spike in IOP is prevented.99 Combining cataract extraction with any of a variety of methods that allows for increased outflow effectively minimizes the pressure spike that occurs after cataract surgery (Table 16.1). Phacotrabeculectomy protects against early postoperative elevations in IOP compared to phacoemulsification alone. This difference in IOP is detectable at 4 hours after surgery with 5% of phacotrabeculectomy eyes experiencing IOP greater than 30 mm Hg compared to 23% with phacoemulsification alone.100 If the IOP is elevated a few days after surgery, release of scleral flap sutures enhances filtration, and the timing of this is critical to long-term bleb survival.101
TABLE 16.1 Patients Who Are Candidates for Combined Cataract and Glaucoma Procedures Include Symptomatic Cataract and Any of the following | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Long-term IOP control after combined cataract-glaucoma surgery is better than cataract extraction alone.
Combining a cataract extraction with a filtration procedure without using an antimetabolite, results in a long-term lowering of intraocular pressure slightly greater than that caused by cataract extraction alone.100,101,102,103,104,105,106 Long-term IOP control after phacotrabeculectomy is better than with ECCE-trabeculectomy with fewer medications needed in the phacotrabeculectomy group.107 Phacoviscocanalostomy provides excellent visual acuity with minimal complications and greater IOP reduction than cataract surgery alone.108
5-FU does not improve the IOP-lowering effect of combined cataract and glaucoma surgery.
Adjunctive use of 5-fluorouracil (5-FU) at the time of cataract extraction has, in the dosage and methods so far used, not appreciably improved the long-term pressure lowering associated with ECCE combined with a guarded filtration procedure.107,108,109,110,111 There also appears to be limited pressure lowering benefit from postoperative 5-FU injections for combined same-site phacotrabeculectomy.110,111,112,113,114 A recent study found 5FU phacotrabeculectomy similar in IOP reduction to 5FU trabeculectomy, although the combined group required a greater number of injections.115
Mitomycin-C (MMC) does improve the IOP-lowering effect of combined cataract and glaucoma surgery.
Antimetabolite usage is worth the long-term risks of blebitis and hypotony in patients who are likely to go blind without its application. However, patients without advanced disc damage who can tolerate one or two postoperative glaucoma medications may not need an antimetabolite and certainly should not be exposed to high concentrations of Mitomycin-C. Combined same-site phacotrabeculectomy with MMC lowers IOP more effectively with fewer postoperative medications and larger filtration blebs than without MMC.114,115,116,117,118 Mitomycin-C also improves the success rate in blacks, eyes of patients on ≥ 2 glaucoma medications, eyes with IOP ≥ 20 mm Hg, and prior failed trabeculectomy.119,120 Antimetabolite use in combined procedures is associated with a lower postoperative IOP with reduced needs for long-term glaucoma medications.121 Mitomycin C appears to have a beneficial effect on long-term filtration surgery and on combined surgery without the corneal toxicity of 5-FU.122 However, long-term bleb morphology with MMC is different from that with 5-FU. Excessive concentrations or durations of MMC cause progressive conjunctival necrosis with bleb leaks, hypotony, and possible endophthalmitis123. Antimetabolite usage has decreased with trabeculectomy surgery and is reserved for high-risk patients likely to scar down without its usage.
Combined Cataract and Glaucoma Surgery
Phacotrabeculectomy is more effective than ECCE-trabeculectomy with or without postoperative 5-FU injections.121,122,123,124,125,126,127 The smaller incision associated with phacoemulsification likely leads to less intraocular inflammation and wound healing allowing better bleb formation. Phacotrabeculectomy with intraoperative and/or postoperative 5-FU significantly lowers IOP but not as successfully as 5-FU trabeculectomy alone.128 This is probably related to the prolonged anterior chamber flare following phacoemulsification compared to trabeculectomy with peripheral iridectomy.129 Combined same-site phacoemulsification, posterior chamber IOL, and trabeculectomy without antimetabolite significantly lowers IOP.127,128,129,130,131,132,133 Results of same-site phacotrabeculectomy appear similar with either a 3.5-mm incision with a foldable IOL or a 5.2 mm incision with a rigid single-piece PMMA lens.134,135
Phacotrabeculectomy with intraoperative 5-FU is as efficacious as a 5-FU trabeculectomy followed by phacoemulsification.136 Visual acuity and complications of combined phacotrabeculectomy are comparable to a two-staged approach with the obvious benefit of earlier visual rehabilitation.137 Foldable silicone lenses are associated with an increase in postoperative inflammation compared to PMMA lenses.138 The newer generation silicone lenses are not associated with more inflammation.139
Trabeculectomy
Trabeculectomy alone or in combination with lens extraction plays a significant role in the management of patients with both cataract and glaucoma. Trabeculectomy is highly successful in patients with POAG and virgin conjunctiva. Patients with a complex cataract where complications are expected to be high may fare better with a filter alone, especially with advanced glaucomatous disease and dangerously high IOP, where immediate IOP control is required. However, there are risk factors associated with filtration surgery. A study from England found diabetes, superior rectus traction suture, subconjunctival anesthetic and nonspecialist surgeons was associated with poorer outcome.140 The Advanced Glaucoma Intervention Study (AGIS) demonstrated that failure of trabeculectomy was associated with younger age, higher preintervention IOP, diabetes, and postoperative marked inflammation.141 Trabeculectomy with mitomycin C provides acceptable long-term success in pseudophakic eyes with minimal complications.142 It is well established that trabeculectomy increases the likelihood of cataract formation.143 Progress in trabeculectomy technique (Fig. 16.4), especially in wound construction and antimetabolite application, has significantly improved bleb characteristics while maintaining excellent IOP control.
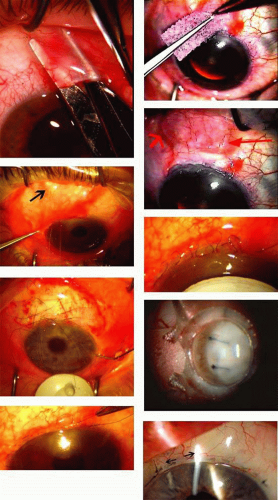 FIGURE 16.4 Trabeculectomy overview, current concepts. Recent trends in trabeculectomy technique allow better bleb architecture and IOP control. An overview of the trends include: A. A definite tendency to use a fornix-based conjunctival approach due to better bleb formation in high-risk eyes that scar. With low potential for scarring, fornix or limbus-based give similar bleb formation results. B–D: The methodology of application of MMC is critical; a large sponge (B) helps evenly spread out the antimetabolite, usually MMC 0.2 mg/cc. Place the pledget posterior to the scleral flap, black arrow, as in (C), not as in (D), where the sponge, red arrow, is placed directly over the filtration site. In order to avoid a pale avascular bleb, place the sponge posteriorly and under Tenons capsule when possible. Notice the bleb in Fig. 16.2A, it is pale but not avascular. (E): The key is to construct a scleral flap that is uniform and that will allow flow early on, in order to facilitate the formation of a healthy bleb. (F,G) Use a running horizontal mattress closure as described by Jim Wise MD, and incorporate Tenon’s capsule into it (I believe a helpful additional pearl) and close tightly. H: The timing of suture lysis is based on years of clinical judgment, but is imperative to the long-term success of the procedure. I: The meticulous limbal closure is seen at the slit lamp. Note the architecture of the closure and study it in the surgical section. Leaks are very rare with this closure, less than 1% when constructed properly. The arrows reveal the direction of the vector forces helping to tether the conjunctiva to the limbus. |
Single-Site Versus Two-Site Combined Cataract and Glaucoma Surgery
Combined ECCE-trabeculectomy techniques now yield to smaller-incision combined phacotrabeculectomy. The methods for combining phacotrabeculectomy vary, depending on physician training, preference, and patient anatomy. For example, physicians with two-site experience will have an easier access to the surgical site in a patient with enophthalmos and a prominent brow who requires a combined procedure. A temporal approach for the lens extraction is much easier in this particular case. Two-site phacotrabeculectomy with MMC and a water-tight modified fornix-based closure significantly reduced IOP from a preoperative mean of 23 mm Hg to 14.9 mm Hg with minimal complications and excellent visual acuity.144 Intraocular pressure control following one-site versus two-site phacotrabeculectomy with MMC is similar but with a trend for less postoperative glaucoma medications,145 improved IOP control,146 less induced astigmatism, 147 and better bleb formation in the two-site group.148 A longer follow-up study found equivalency when comparing one-site fornix-based phacotrabeculectomy to two-site limbus-based phacotrabeculectomy.149 Notably, in this study there was a much higher risk of early wound leak in the fornix-based group, 14% versus 0%. A comparable study found equivalency of IOP reduction with one-site vs two-site, but did note longer operating room time and a lower corneal cell count with the two-site approach.150 Another recent study revealed comparison of one-site versus two-site phacotrabeculectomy gave comparable results regarding visual acuity, IOP control, and postoperative medications.151
Phacoemulsification Combined With Glaucoma Drainage Implant Surgery
The use of glaucoma drainage implants in the management of glaucoma patients is increasing, especially with the favorable results seen with the tube versus trabeculectomy study, as well as other comparative studies.152 The tube versus trabeculectomy study demonstrated similar IOP lowering efficacy between the two groups, but with the greater need for postoperative glaucoma medications in the tube group (1.3 vs. 0.5). The authors concluded that nonvalved drainage implants were more likely to maintain IOP control than trabeculectomy in their patient group,153 and serious postoperative complications were limited, but more frequent in the trabeculectomy group.154 However, persistent diplopia remains a problem in the drainage implant group that is not seen in the filter group. Physicians are increasingly presented with drainage implant patients who need cataract surgery, and in general, visual acuity is improved and IOP control is maintained post lens extraction.155 These eyes are typically more difficult to manage due to the refractory nature of the eyes that required a drainage implant such as neovascular glaucoma, developmental glaucomas, traumatic glaucomas and of course pseudophakic eyes (PCIOL). Many of these eyes require iris hooks and more intensive follow-up post lens extraction to monitor inflammation and IOP. In general, the results from drainage implants are encouraging, even in eyes with a failed filter.156
Cataract Extraction Causes Partial or Complete Failure of Existing Filtering Blebs
Cataract extraction by any technique performed in a patient with a pre-existing filter will have an effect on the previous filtering bleb.153,154,155,156,157, 158,159,160,161 Bleb failure is more likely with ECCE compared to small-incision phacoemulsification.162 However, even patients undergoing topical anesthesia with clear corneal phacoemulsification and foldable IOL may experience bleb failure. One of three patients with a functioning filter and preoperative mean IOP of 12 mm Hg without antiglaucoma medications experiences bleb failure after lens extraction (Table 16.2). These patients require long-term drug therapy or bleb needling to control IOP.163,164 Additional incisional glaucoma surgery may be required in up to 10% of patients.165 Intraoperative iris manipulation may cause significant breakdown of the blood-aqueous barrier resulting in inflammation that causes bleb failure. Even after uncomplicated clear corneal phacoemulsification, IOP may increase an average of 2 to 3 mm Hg due to bleb fibrosis.166 Approximately 20% of filtered patients will require a long-term increase in glaucoma medications following uncomplicated clear corneal phacoemulsification with a foldable copolymer acrylic intraocular lens.167
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


