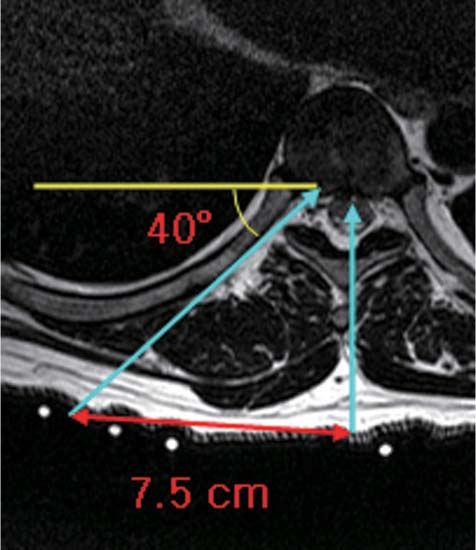
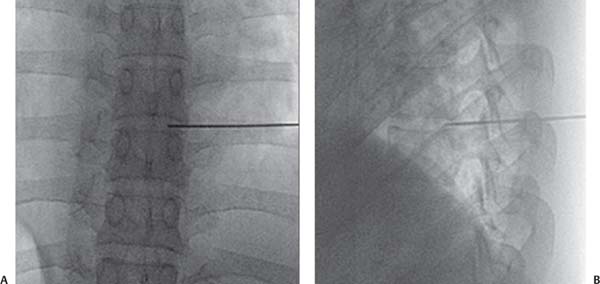
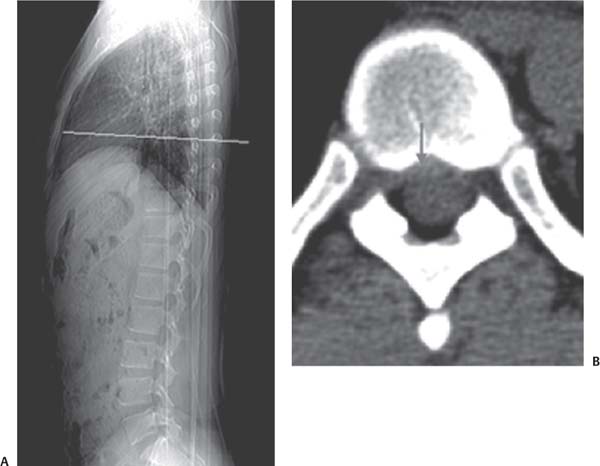
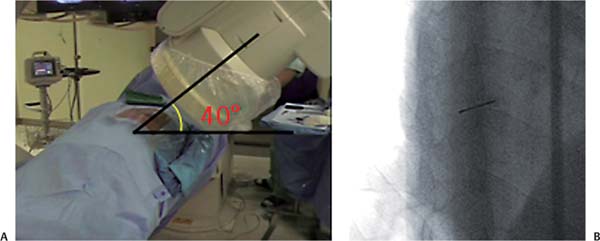
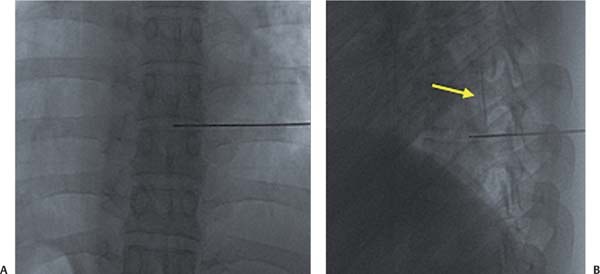
12 Case Presentations and Surgical Technique: Percutaneous Endoscopic Thoracic Diskectomy • A 29-year-old male patient presented with leg and back pain. • The leg pain was scored at 7/10 on the visual analog scale, whereas the back pain was scored at 5/10. • Chief complaint was mild paraparesis (grade IV/IV). • Preoperative imaging studies were conducted. • Magnetic resonance imaging (MRI) sagittal and axial views show a central disk extrusion at the T7-T8 level (Fig. 12.1). • A computed tomographic (CT) scan shows a soft disk herniation at the T7-T8 level (Fig. 12.2). • It is determined that the patient will undergo a percutaneous endoscopic thoracic diskectomy (PETD) to correct the central disk extrusion at T7-T8. Fig. 12.1 Sagittal (A) and axial (B) MRIs showing a central disk extrusion at the T7-T8 level. Fig. 12.2 AP radiograph (A) and CT scan (B) showing a soft disk herniation at the T7-T8 level (arrow). Fig. 12.3 The skin entry point is 7.5 cm from the midline as shown on this axial MRI scan. • A right-sided approach is selected, and the skin entry point is determined as 7.5 cm from the midline according to axial MRI (Fig. 12.3). 1. The needle position must be located between the pedicle and the rib head on the C-arm oblique view while the needle is being inserted (Fig. 12.4). The final needle position can be seen in anteroposterior (AP) and lateral views (Fig. 12.5). 2. Diskography is conducted to show epidural leakage of the contrast media (Fig. 12.6). 3. The obturator is advanced over the guide wire (Fig. 12.7). 4. The final working channel is positioned as shown with AP and lateral views (Fig. 12.8). • The holmium:yttrium-aluminum-garnet (Ho:YAG) side-firing laser directed toward the posterior longitudinal ligament (PLL) can be seen in Fig. 12.9A. Notice the annulus tear site and that the herniated fragment can be seen through the tear. Fig. 12.4 (A) The fluoroscope is aligned to provide an oblique view. (B) The needle is located between the pedicle and rib head as shown in the oblique fluoroscopic view. Fig. 12.5 The final needle position is shown in AP (A) and lateral (B) fluoroscopic views.
Central Disk Extrusion at the T7-T8 Level
Clinical Findings
Preoperative Plan

Surgical Procedures
Endoscopic Findings
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


