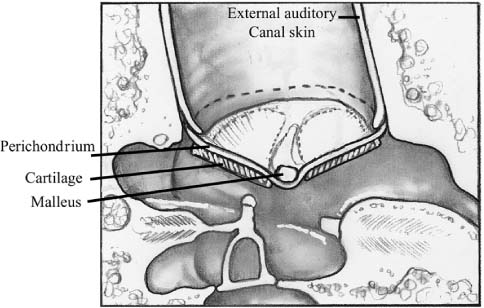
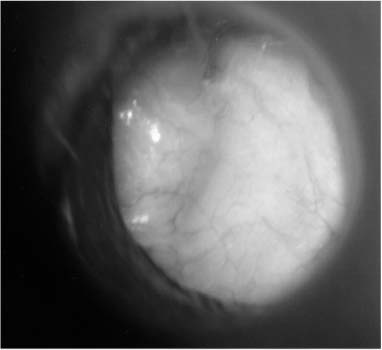
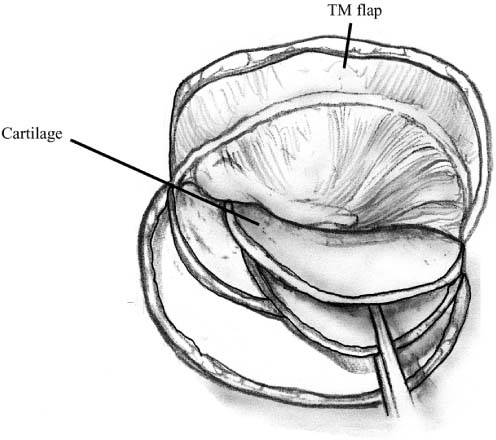
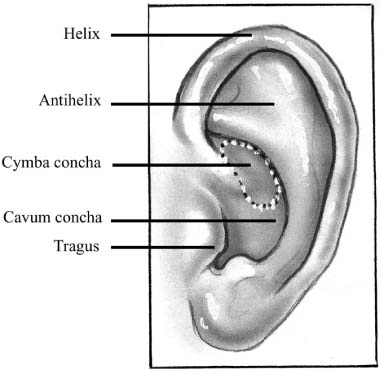
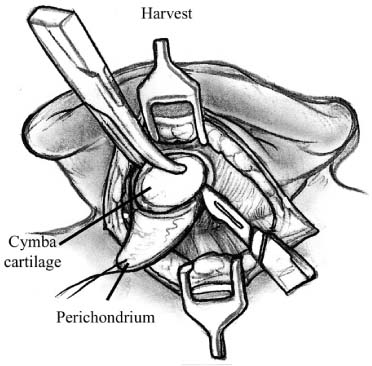
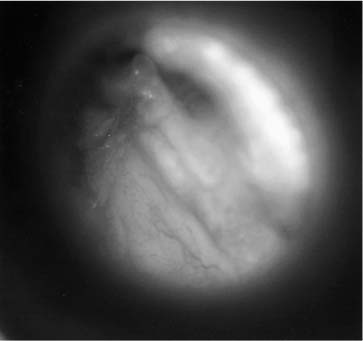
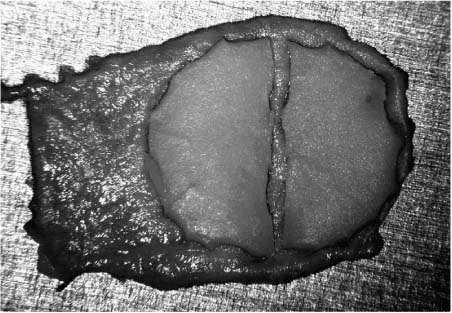
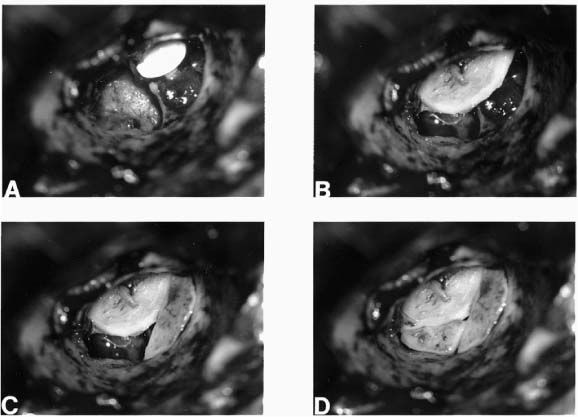
Chapter 6 Generally speaking, there are two distinct techniques utilized for cartilage reconstruction of the tympanic membrane (TM): the perichondrium/cartilage island flap, which uses tragal cartilage, and the palisade technique, which uses cartilage from the tragus or cymba, depending on the surgical approach. Either technique can be used to reconstruct the TM; however, the choice of technique is typically dictated by the specific middle ear pathology or, in cases where the TM reconstruction is in conjunction with ossiculoplasty, the status of the ossicular chain. The palisade technique is preferred in cases of cholesteatoma and when ossicular reconstruction is needed in the malleus-present situation. The perichondrium/cartilage island flap is preferred for management of the atelectatic ear and the high-risk perforation. This chapter describes the two techniques in detail, followed by descriptions of the modifications that should be taken in response to specific surgical indications. Tympanoplasty, or repair of the TM, was first introduced by Zoellner1 and Wullstein2 in 1952. Since that time, numerous graft materials and methods of placement have been described to reconstruct the TM. Skin, fascia, vein, and dura mater have all been described as grafting materials for the TM.3–9 Temporalis fascia and perichondrium remain the most commonly employed materials for closure of TM perforations, and successful reconstruction is anticipated in approximately 90% of primary tympanoplasties.10 In certain situations, such as the atelectatic ear, cholesteatoma, and revision tympanoplasty, however, the results have not been as gratifying. In these situations, fascia and perichondrium have been shown to undergo atrophy and subsequent failure in the postoperative period, regardless of placement technique.11 The recurrent perforation and discharging ear are likewise associated with less than optimal results.12–14 These observations have led to the use of less compliant, more rigid grafting materials for TM reconstruction, such as the cartilage graft. Although one might anticipate a significant conductive hearing loss with cartilage, due to its rigidity, it is this quality that tends to resist resorption and retraction, even in the milieu of continuous eustachian tube dysfunction. It has been shown in both experimental and clinical studies that cartilage is well-tolerated by the middle ear, and long-term survival is the norm.15–18 It appears that cartilage grafts are nourished largely by diffusion and become well-incorporated in the TM.19 Human and animal studies20,21 have shown that although some softening occurs with time, the matrix of the cartilage remains intact, but with empty lacunae, demonstrating degeneration of the chondrocytes. The use of cartilage in middle ear surgery is not a new concept, but the last decade has shown a renewed interest in this material as an alternative to more traditional grafting materials for TM reconstruction. Cartilage has been recommended on a limited basis to manage retraction pockets by ad-vocates such as Sheehy,22 Glasscock and Hart,23 Levinson,19 Eviatar,24 and Adkins,25 all of whom have reported excellent anatomic results. Cartilage also has been described for use in cases of recurrent perforation and revision tympanoplasty with encouraging results.14,26,27 Given the good anatomic results, more attention also has been given to the acoustic properties of cartilage compared with more traditional grafting materials. In a retrospective comparison between perichondrium and cartilage in type I tympanoplas-ties, we reported no significant difference in hearing between groups.28 Graft take was 100% in the cartilage group and 85% in the perichondrium group. These results were supported by other researchers who have shown excellent closure of the air bone gap with cartilage tympanoplasty techniques.14,26,27,29 Cartilage for TM reconstruction is typically har-vested from two areas, the tragus and the cymba, depending on the type of reconstruction to be performed. The perichondrium/cartilage island flap is nearly always constructed with cartilage harvested from the tragus. This cartilage is ideal because it is thin, flat, and in sufficient quantities to permit reconstruction of the entire TM. The cartilage is used as a full-thickness graft and is typically slightly less than 1 mm thick in most cases. Although Zahnert et al30 suggested a slight acoustical benefit could be obtained by thinning the cartilage to 0.5 mm, this advantage is offset by the unacceptable curling of the graft that occurs when the cartilage is thinned and perichondrium is left attached to one side. When the palisade technique is used for reconstruction of the TM, cartilage can be harvested from either the tragus or the cymba. Cartilage from the cymba area of the conchal bowl is used if the surgical approach involves a postauricular incision. Tragal cartilage is used if the approach is transcanal or endaural. The cartilage of the cymba is similar to the tragus in that it has an acceptable thickness of about 1 mm compared to other areas of the concha, which are thicker and irregular. It is different, however, in that it is curved, making it difficult to create a perichondrium/cartilage island flap suitable for reconstruction of the entire TM. The general technique of reconstruction using the perichondrium/cartilage island flap begins with harvest of the cartilage from the tragal area.28 An initial cut through skin and cartilage is made on the medial side of the tragus, leaving a 2-mm strip of cartilage in the dome of the tragus for cosmesis (Fig. 6–1). The cartilage, with attached perichondrium, is dissected medially from the overlying skin and soft tissue by spreading a pair of sharp scissors in a plane that is easily developed superficial to the perichondrium on both sides. At this point, it is necessary to make an inferior cut as low as possible to maximize the length of harvested cartilage. The cartilage is then grasped and retracted inferiorly, which delivers the superior portion from the incisura area. The superior portion is then dissected out while retracting, which produces a piece of cartilage typically measuring 15 × 10 mm in children and somewhat larger in adults. The perichondrium from the side of the cartilage furthest from the ear canal is dissected off, leaving the thinner perichondrium on the reverse side. A perichondrium/cartilage island flap is constructed as described previously.28 Using a round knife, cartilage is removed to produce an eccentrically located disk of cartilage about 7 to 9 mm in diameter for total TM reconstruction. A flap of perichondrium is produced posteriorly that will eventually drape over the posterior canal wall. A complete strip of cartilage 2 mm in width is then removed vertically from the center of the cartilage to accommodate the entire malleus handle (Fig. 6–2). The creation of two cartilage islands in this manner is essential to enable the reconstructed TM to bend and conform to the normal conical shape of the TM. When the ossicular chain is intact, an additional triangular piece of cartilage is removed from the posterior-superior quadrant to accommodate the incus. This excision prevents the lateral displacement of the posterior portion of the cartilage graft that sometimes occurs because of insufficient space between the malleus and incus. FIGURE 6–1 Harvest of cartilage, leaving small rim of cartilage in dome for cosmesis (right ear). FIGURE 6–2 Prepared perichondrium/cartilage island graft, showing strip of cartilage removed to facilitate malleus. The entire graft is placed in an underlay fashion, with the malleus fitting in the groove and actually pressing down into and conforming to the perichondrium, as shown in FIGURE 6–3. The cartilage is placed toward the promontory, with the perichondrium immediately adjacent to the TM remnant, both of which are medial to the malleus. Failure to remove enough cartilage from the center strip will cause the graft to fold up at the center instead of lying flat in the desired position. Likewise, if the strip is insufficient, the cartilage may be displaced medially instead of assuming a more lateral position in the same plane as the malleus. FIGURE 6–3 Lateral line drawing demonstrating proper placement of graft. FIGURE 6–4 Postoperative ear with perichondrium/cartilage island graft (left ear). Gelfoam (Upjohn Laboratories, Kalamazoo, MI) is packed in the middle ear space underneath the anterior annulus to support the graft in this area, and the posterior flap of perichondrium is draped over the posterior canal wall. Middle ear packing is avoided on the promontory and in the vicinity of the ossicular chain. One piece of Gelfoam is placed lateral to the reconstructed TM, and antibiotic ointment is placed in the ear canal (Fig. 6–4). In the palisade technique, the cartilage is cut into several slices that are subsequently pieced together, like the pieces of a jigsaw puzzle, to reconstruct the TM (Fig. 6–5). Because of the nature of the reconstruction, it is not necessary to have one large, flat piece of cartilage, and the more curved cymba cartilage, which is harvested from the postauricular incision, is suitable (Fig. 6–6). A large area of conchal eminence can be exposed by elevating the subcutaneous tissue and postauricular muscle from the conchal perichondrium. The cymba cartilage is the prominent bulge at the superior aspect of the concha (Fig. 6–7). A circumferential cut the size of the anticipated graft is made through the perichondrium and cartilage, but not through the anterior skin. The perichondrium is removed from the postauricular side, and the cartilage, with the perichondrium on the anterior aspect, is dissected from the skin. This technique is also used for harvesting cartilage for canal wall reconstruction when the retrograde mastoidectomy technique is used for cholesteatoma surgery. The technique described here differs somewhat from the palisade tympanoplasty of Heermann et al.31 Instead of placing rectangular strips of cartilage side to side, an attempt is made to cut one major piece of cartilage in a semi-lunar fashion, which is placed directly against the malleus on top of the prosthesis (Fig. 6–8A,B). This acts to reconstruct a major portion of the posterior half of the TM and serves as a foundation for the rest of the cartilage pieces. A second semi-lunar piece is placed between this first piece and the canal wall to reconstruct the scutum precisely (Fig. 6–8C). Any spaces that result between this cartilage and the canal wall or scutum are filled in with small slivers of cartilage to prevent prosthesis extrusion and recurrent retraction (Fig. 6–8D). The reconstruction is then covered with the previously harvested perichondrium draped over the posterior canal wall (Fig. 6–9). FIGURE 6–5 Schematic of palisade technique (right ear). FIGURE 6–6 Schematic illustrating location of cymba cartilage (left ear). FIGURE 6–7 Harvesting of cymba cartilage with post-auricular incision (right ear). Although this technique can be used for TM reconstruction without ossicular reconstruction, it is favored when ossiculoplasty is performed in a malleus-present situation and is especially suitable for cholesteatoma surgery. Because the prosthesis is placed prior to the cartilage reconstruction, this technique allows direct visualization and contact of the notched prosthesis to the manubrium handle, which has been shown to provide superior hearing results.32 The prosthesis acts as a scaffolding on which the cartilage is placed, which serves to reconstruct the TM as well as prevent prosthesis extrusion. It likewise allows a precise and watertight fit between the reconstructed TM and the canal wall in the posterior area, where recurrent cholesteatoma most frequently occurs. Typically, in these situations, the anterior half of the TM is not altered or is grafted with conventional materials to allow cholesteatoma surveillance and possible intubation in the post-operative period if necessary. Typically, the packing material of Gelfoam and antibiotic ointment is completely suctioned from the external canal 1 to 2 weeks after the surgical procedure. Antibiotic steroid-containing drops are used for an additional 2 weeks to clear the ear of residual ointment and Gelfoam, the latter of which can lead to granulation and fibrous tissue formation if inadequately removed from the TM. The adult patient is instructed to begin the Valsalva maneuver, and children are instructed to use the Otovent (Invotec International, Jacksonville, FL), three times a day beginning 2 to 3 weeks after the surgery. A postoperative audiogram is obtained 6 to 8 weeks later, and the TM is examined. If the hearing result is good and the TM is clear, the ear is examined at 6 months and again at 1 year from the date of surgery. If effusion is present, nasal steroids are added, the Valsalva (or Otovent) is encouraged, and the ear is examined at 3 months. If the effusion is still present at that time, the ear is intubated. If a total cartilage reconstruction had been performed, tube insertion using traditional techniques can be difficult. In this situation, a CO2 laser myringotomy is preferred, followed by insertion of a soft tube, such as the Goode T-tube (Medtronic Xomed Surgical Products Inc., Jacksonville, FL). FIGURE 6–8 Series demonstrating sequence of palisade reconstruction (left ear). (A) Total ossicular replacement prosthesis (TORP) in place. (B) Initial cartilage placement. (C) Reconstruction of the scutum. (D) Reconstruction of remainder of posterior tympanic membrane. FIGURE 6–9 Postoperative appearance of tympanic membrane after palisade reconstruction (right ear).
CARTILAGE TYMPANOPLASTY
TECHNIQUES FOR RECONSTRUCTION
HARVEST OF THE CARTILAGE GRAFT
PERICHONDRIUM/CARTILAGE ISLAND FLAP

THE PALISADE TECHNIQUE
POSTOPERATIVE CARE
SPECIFIC INDICATIONS AND SUBSEQUENT MODIFICATIONS TO THE SURGICAL TECHNIQUE
THE HIGH-RISK PERFORATION
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


