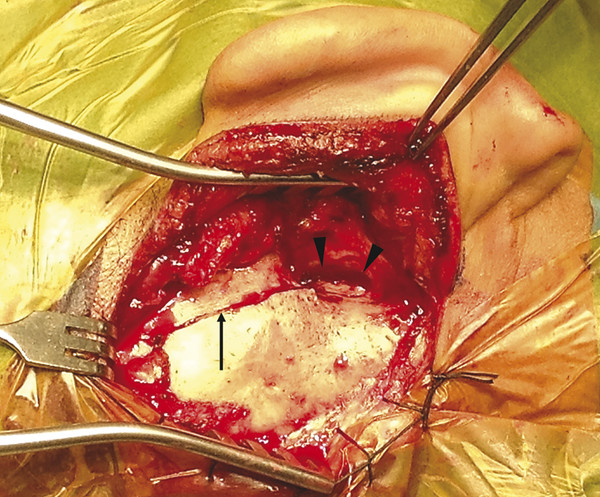
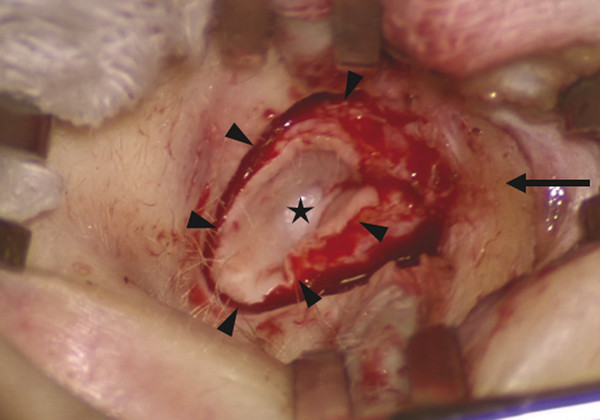
Canalplasty refers to the surgical procedure that attempts to restore or create the natural contour and patency of the external auditory canal (EAC). Meatoplasty, on the other hand, describes the surgical creation of an enlarged external ear aperture. As the external ear aperture, or meatus, is in continuity with the bony and cartilaginous portions of the EAC, surgery on the EAC should almost always be accompanied by surgery on the external ear meatus. Thus, a canalplasty should be matched with an adequate meatoplasty. Canalplasty involves surgery on both the soft tissue as well as bony components of the EAC. Surgery on just one of these components is rarely adequate. The indications for canalplasty include numerous pathologic conditions that may present as, or result in, canal stenosis or obliteration (▶ Table 20.1). These pathologies could be broadly categorized into bony or soft tissue in origin. Other conditions, such as keratosis obturans, although not causing canal stenosis, require canalplasty to prevent complications. For the purposes of this chapter, congenital aural atresia and congenital canal stenosis are not discussed (see Chapter 47 for a full discussion of these conditions). Bony stenosis Exostosis Osteoma Fibrous dysplasia Post-traumatic fracture Soft tissue stenosis Chronic stenosing otitis externa (CSOE) – secondary to recurrent or chronic inflammation. (Also known as post-inflammatory acquired atresia, obliterative otitis externa, or medial canal fibrosis.) Trauma Fracture Burns Chemical injury Iatrogenic causes Postoperative scarring Post-irradiation Dermatological diseases (e.g., dermatitis, psoriasis, etc.) Soft tissue neoplasms (benign, e.g., seborrheic keratosis, or malignant) Others Keratosis obturans External canal cholesteatoma As part of other operations (e.g., tympanoplasty, mastoidectomy) Canalplasty is also performed during excision of benign soft tissue tumors of the EAC (e.g., squamous papilloma, seborrheic keratosis, or hemangioma). These tumors are fully excised with a small margin and full-thickness canal wall skin. A widened EAC facilitates postoperative surveillance. Split-thickness skin grafts may be necessary to cover any bare bone (see Chapter 48). Canalplasty is an important part of other operations for chronic ear disease, especially tympanoplasty. In tympanoplasty, including underlay and overlay grafting techniques, canalplasty facilitates exposure and visualization of the entire tympanic membrane and annulus, especially the anterior portion. It provides access for canal skin elevation, evaluation of the ossicles, and secure placement of tympanic membrane grafts. Canalplasty also helps in postoperative care and follow-up examinations. In keratosis obturans and EAC cholesteatoma, although there is no canal stenosis per se, there are crevices and bony overhangs in the EAC that cause accumulation of debris. Frequently, a significant area of bony canal is rendered bare and potentially devitalized. The bony EAC may also be expanded. At the same time, the meatus is too small, whether for proper inspection or for debridement. Therefore, canalplasty in combination with meatoplasty is necessary to smooth the canal contour and to enlarge the EAC opening. Any bare areas in the EAC are covered by a split-thickness skin graft. Removal of all disease must be achieved and the bony contours of the EAC smoothed out before covering bare areas in the EAC with a split-thickness skin graft. A meatoplasty matching the size of the canalplasty should be performed for ease of regular surveillance and debridement. Besides the inciting events (infection, trauma, etc.), early canal stenosis does not usually produce symptoms. Recurrent external otitis may occur later because the natural elimination of cerumen and desquamated epithelium from the EAC is impeded. Conductive hearing loss is a common symptom. This may result from occlusion of the EAC or when cerumen or debris tamponades against the tympanic membrane. Less commonly, cholesteatoma may develop medial to soft tissue stenosis. In contrast to symptomatic bony stenosis, for which surgery is usually the only viable option, early soft tissue stenosis may be treated medically. This includes periodic dilation and stenting of the EAC with antibiotic- and steroid-impregnated expandable ear wicks. These wicks are replaced every 7 to 10 days for 6 to 8 weeks. Alternatively, the subcutaneous injection of steroid (triamcinolone) into the meatus may reverse or halt stenosis of the membranous EAC if applied early in the disease process. Patients who do not respond to these treatments are candidates for surgery. All patients who undergo surgery require a preoperative audiogram to document the conductive hearing loss and any preexisting sensorineural hearing loss. A computed tomography (CT) scan of the temporal bone is performed to assess the location (lateral or medial), extent, and configuration of the stenosis. It is also useful in demonstrating possible cholesteatoma medial to the stenosis and evaluating any involvement of the middle ear and mastoid. In addition, the CT scan provides valuable preoperative information on the location of vital structures, such as the facial nerve. The goals of ear canal surgery are, first, to treat any concomitant infection (including associated cholesteatoma) and, second, to improve or reverse any conductive hearing loss. The principles of canalplasty for bony canal stenosis differ from those when soft tissue stenosis is the main indication. For example, in EAC stenosis due to exostosis, the canal skin is usually normal and should be preserved during canalplasty. This promotes the re-epithelization of the enlarged canal and may obviate the need for a split-thickness skin graft. In contrast, in soft tissue stenosis, especially in chronic stenosing otitis externa, the preservation of adjacent skin is not possible or desirable given that the canal skin is either contributing to the stenosis or is largely composed of fibrotic scar tissue; thus, full-thickness resection of canal wall skin is required. The techniques of canalplasty and meatoplasty described herein are suitable for all indications, including tympanoplasty and tympanomastoidectomy. An endaural-alone approach or a combination of endaural and postauricular approaches may be used for canalplasty. The endaural approach allows for canalplasty and meatoplasty simultaneously. The postauricular approach allows soft tissue flaps to be raised around the EAC; these flaps are useful when there is extensive exposure of mastoid cells. After intubation and appropriate positioning, the patient’s upper arm (hairless skin), hip, or thigh on the ipsilateral side is also prepared and draped accordingly to facilitate possible split-thickness skin graft harvesting (▶ Fig. 20.1). Fig. 20.1 While the patient is under general anesthesia, the right upper thigh is prepared for split-thickness skin graft harvest while surgery proceeds on the right ear. The expected incisions and external ear canal are injected with 2% lidocaine with 1:80,000 epinephrine. The anterior canal wall, conchal bowl, and crus of the helix are also injected. Pearls and Pitfalls It is important to inject local anesthetic slowly with the needle in contact with bone. A too rapid or forceful injection would raise a wheal, further narrowing the already narrow canal lumen. If an endaural incision is used, the surgery uses the same incision in the helicotragal groove and terminal incisure as for meatoplasty (see later discussion). This is then connected medially to a full-thickness radial EAC incision at 12 o’clock. The EAC is then held open with two self-retaining retractors placed perpendicularly to each other. The postauricular incision is created approximately 1 cm posterior to the postauricular sulcus and carried down to the level of the temporalis fascia and periosteum in the standard manner. After incising the mastoid periosteum, the canal wall skin is then elevated off the underlying bone with a periosteal elevator. The EAC is entered posteriorly via an incision using a size 11 scalpel. The position of this incision is dictated by the location of the stenosis and should be placed just lateral to the stenosis. Otherwise, it is placed in a position beginning at about 5 mm medial to the suprameatal spine (▶ Fig. 20.2). Fig. 20.2 Postauricular approach to canalplasty for EAC stenosis in a case caused by temporal bone fracture. The fracture line is seen (arrow). The EAC has been entered via a canal incision in the skin posteriorly (arrowheads). The ear and posterior canal flap are held forward with a self-retaining retractor. In many clinical situations (e.g., medial canal fibrosis) or if drilling of the anterior canal wall is anticipated, the canal incision is continued onto the anterior canal wall into a full circumferential incision (▶ Fig. 20.3). The skin of the EAC and soft tissue lateral to the incision are then elevated over the tympanic bone and retracted forward. Fig. 20.3 An endaural approach to a case of medial canal fibrosis secondary to chronic inflammation. In this case, the endaural incision (arrow) is extended medially and is continuous with the circumferential canal incision (arrowheads) lateral to the area of fibrosis, which appears as a false fundus (asterisk). Pearls and Pitfalls It has been recommended that the anterior and posterior canal incisions be staggered to minimize the risk of circumferential stenosis. However, if the canal is further widened with drilling, the skin flaps are replaced properly, and there is meticulous postoperative care, there will be an extremely low risk of circumferential stenosis occurring. Subsequently, the medial skin is carefully and circumferentially elevated off the underlying canal wall bone to the level of the tympanic annulus (▶ Fig. 20.4).1 This exposes the whole EAC for canalplasty. In executing this step, some surgeons prefer to completely remove the anterior canal wall skin, to be later replaced as a skin graft, especially when canalplasty is performed as part of an overlay tympanoplasty (see Chapter 24).2 If the canal wall skin is not removed, it is covered with a thick piece of Silastic sheeting or tin foil from a suture package to protect it from the rotating drill bur. Fig. 20.4 Skin of the EAC is circumferentially elevated down to the level of the tympanic annulus. For underlay tympanoplasty, the anterior canal wall skin is left in place, protected by a Silastic disk during canal bone drilling, and redraped thereafter. For overlay tympanoplasty, the anterior canal wall skin is completely removed in continuum with the lateral epithelial layer of the tympanic membrane and later replaced as a free skin graft. (Used with permission from Atlas M, Eisenberg R. A Guide to Temporal Bone Dissection. 2nd Ed. Perth: Lions Ear & Hearing Institute; 2004.) The canalplasty begins by enlarging the canal laterally at the level of the suprameatal (Henle’s) spine and the tympanosquamous suture, which can be quite prominent and obstructive in some cases. Once the major bone protuberances have been smoothed laterally, the surgeon will typically drill a deep superior trough into the zygomatic root through the tympanosquamous suture line and an inferior trough into the tympanic bone, both of which are immediately adjacent to the anterior canal wall bone. Drilling of these troughs creates an appearance that is sometimes referred to as “Mickey Mouse ears.” Once these troughs are sufficiently deep to expose the annulus in the anterior-superior and inferior aspects, the anterior canal wall bone lying in between is then broadly removed to connect these troughs. In doing so, the penetration of the temporomandibular joint capsule is avoided while the entire anterior aspect of the annulus is exposed. Even after the cause of EAC stenosis has been addressed, the bony canal must be enlarged further to minimize the risk of recurrent stenosis. The canalplasty is complete when a funnel-shaped or truncated conical-shaped bony canal tapering medially is obtained and the complete tympanic annulus can be seen with one position of the microscope (▶ Fig. 20.5). In the event that exostoses of the external ear canal are present, it may be necessary to separately drill the posterior and superior aspect of the EAC more than is usually required (▶ Fig. 20.6). Fig. 20.5 Canalplasty is complete once the entire tympanic annulus can be viewed from a single vantage point without moving the microscope. (Used with permission from Atlas M, Eisenberg R. A Guide to Temporal Bone Dissection. 2nd Ed. Perth: Lions Ear & Hearing Institute; 2004.)
20.2 Patient Selection
20.3 Surgical Technique
20.3.1 Canalplasty
Soft Tissue Exposure

Bone Drilling

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


