Bullous Diseases of the Skin and Mucous Membranes
Sophie X. Deng
Anthony J. Aldave
Nirit Bourla
John A. Hovanesian
Uwe Pleyer
Bartly J. Mondino
Bullous diseases of the skin and mucous membranes consist of two major entities: pemphigoid and pemphigus. The difference is the site of separation of epithelium, the former at the subepithelial level and, the latter, at the intraepithelial level. Both can be associated with severe ocular involvement. Of all the bullous diseases, mucous membrane pemphigoid (MMP), erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) involve the conjunctiva most frequently and also cause the most severe conjunctival disease. Severe ocular involvement associated with other bullous diseases is rarely encountered in clinical practice.
Although advances have been made in elucidating the pathogenesis of bullous diseases in recent years, no unifying pathogenic mechanism has been accepted. Although many bullous diseases, such as MMP, pemphigus, and bullous pemphigoid, are thought to be autoimmune in etiology, some, such as the nonacquired form of epidermolysis bullosa, demonstrate a hereditary basis.
Mucous Membrane Pemphigoid
Mucous membrane pemphigoid, previously known as cicatricial pemphigoid,1 is a group of chronic, recurrent inflammatory disorders of mucous membranes and skin characterized immunopathologically by the linear deposition of autoantibodies at the epithelial basement membrane zone (BMZ). The classic clinical feature of MMP is recurrent mucous membrane and cutaneous bullae that may lead to scar formation and the associated loss of function.2 Ocular involvement is characterized by progressive conjunctival shrinkage and the development of symblephara, entropion with trichiasis, aqueous tear deficiency, and reduced vision from corneal opacification.3 The disease has no geographic or racial predilection and has been shown to be discordant in monozygotic twins.4 The peak age of onset is after 70 years, although a wide range of the age of onset is noted, with patients typically presenting between the ages of 30 and 90.3,5,6,7 MMP affects more women than men, at a ratio of 1.6:1 to 1.8:1.2,3,5 Patients who present with ocular involvement at a younger age (<60 years) tend to have more severe ocular and systemic disease that progresses more rapidly, even with the use of aggressive immunosuppressive therapy.7
Clinical Presentation
Extraocular Involvement
Skin involvement, which is found less frequently than mucous membrane involvement, is reported in 9% to 33% of cases.2,3,4,5,6,8 The skin lesions of MMP can be divided into two types: (a) a recurrent, vesiculobullous, nonscarring eruption that may involve the inguinal area and extremities and occasionally becomes generalized (Fig. 1); and (b) localized, erythematous plaques with overlying vesicles and bullae that appear on the scalp and face near the affected mucous membranes and heal, leaving smooth, atrophic scars (Fig. 2).9 MMP can involve the following mucous membranes: conjunctival, nasal, oral, pharyngeal, laryngeal, esophageal, anal, vaginal, and urethral. The oropharynx and the conjunctiva are the most commonly involved sites. In a dermatologic study, oral lesions were found in 91% and conjunctival lesions in 66% of patients with MMP.8 In ophthalmic studies, 15% to 50% of patients showed involvement of the oral mucosa, whereas 100% had ocular involvement.2,3,4,5
 Figure 1. Intact and ruptured blisters of forearm in a patient with mucous membrane pemphigoid. |
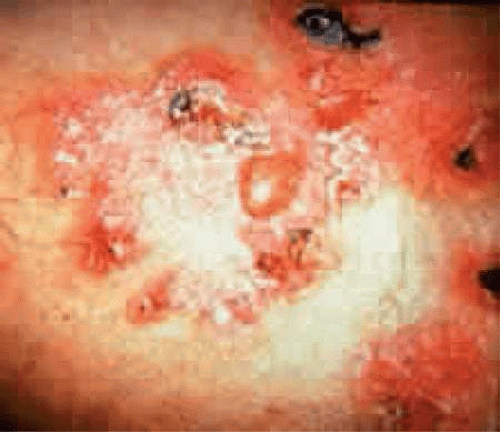 Figure 2. Localized erythematous plaque, with intact and ruptured blisters on it, in a patient with mucous membrane pemphigoid (MMP). |
Mucous membrane pemphigoid is associated with two types of oral lesions.9 The first is a desquamative gingivitis that may be patchy or diffuse, heals slowly, and may persist for years. The second type is characterized by vesicles and bullae of the oral mucosa that develop rapidly, remain intact for a few days, and then rupture. Mucous membrane erosions can heal with scarring and strictures. Stenosis of the nasopharynx or larynx can obstruct the airway causing obstructive sleep apnea or even requiring tracheotomy. Esophageal strictures can result in asphyxiation and death when food is swallowed.10 Patients with only oral mucosal or skin involvement tend to have less scarring and respond better to medical treatment, whereas those with ocular, nasopharyngeal, esophageal, and genital involvement demonstrate a greater tendency to develop localized scarring and secondary loss of function as well as progressive disease, despite the use of immunosuppressive therapy.3,11
Ocular Involvement
The risk of developing ocular disease in patients who initially present with only extraocular MMP is estimated at 0.04/person-year.6 MMP with ocular involvement (MMPO) presents with symptoms that are common to many other causes of chronic bilateral conjunctivitis such as ocular irritation, burning, and tearing.12 A mucopurulent discharge suggests a complicating bacterial blepharoconjunctivitis. Breakdown of the corneal epithelium leads to foreign-body sensation, photophobia, and reduced visual acuity.
Fibrosis beneath the conjunctival epithelium is the hallmark of MMPO.13,14 Interestingly, although the subconjunctival fibrosis was thought the result of the formation and subsequent rupture of conjunctival bullae,13 the bullae are rarely observed. Symblepharon form initially between the inferior palpebral and bulbar conjunctiva are best demonstrated early in the disease by drawing the lower eyelid down and having the patient look up (Fig. 3). Aqueous tear deficiency may develop secondary to subconjunctival fibrosis that occludes lacrimal and accessory lacrimal gland ductules, and a reduced number of mucus-producing goblet cells may also contribute to an unstable tear film.15 Further insult to the ocular surface can result from tarsal conjunctival scarring that produces entropion with trichiasis and distichiasis or lagophthalmos with secondary exposure. Corneal erosions may develop secondary to the poor tear film quality and quantity, and exposure and trauma from the eyelashes and entropic eyelid. These erosions may become infected by local flora and lead to ulceration. Predisposing factors for the development of secondary microbial keratitis include topical corticosteroids, bandage contact lenses, trichiasis, corneal surgery, lagophthalmos, and meibomianitis.16 The chronic and recurrent ocular surface inflammation can result in both limbal and conjunctival stem cell deficiency.17 As a result, slow but relentless conjunctivalization of the corneal surface may lead to corneal blindness and significant functional impairment. Glaucoma may be more prevalent in patients with MMPO and could further increase the risk for visual loss.18
 Figure 3. Symblepharon formation demonstrated by drawing lower lid down and having the patient look up. |
Course of Ocular Disease
Mucous membrane pemphigoid with ocular involvement generally runs a chronic course, characterized by progressive shrinkage of the conjunctiva with chronic inflammation. When the end stage of this disease is reached, the eye lacks tears and has obliterated conjunctival fornices, ankyloblepharon, and a keratinized ocular surface. Episodes of acute disease activity characterized by redness and ulceration of conjunctiva may interrupt this chronic progressive course and result in rapid shrinkage of the conjunctiva.19 Acute disease activity can be precipitated by surgical trauma, such as biopsy of the conjunctiva, lysis of symblepharon, eyelid procedures and even cataract extraction, and manifest as either localized, ulcerated conjunctival mounds (Fig. 4) or diffuse, severe conjunctival hyperemia and chemosis (Fig. 5). Before concluding that an acute exacerbation of the conjunctival inflammation has been precipitated by a certain intervention, other possible causes (e.g., trichiasis, exposure, and bacterial blepharoconjunctivitis) should be excluded.
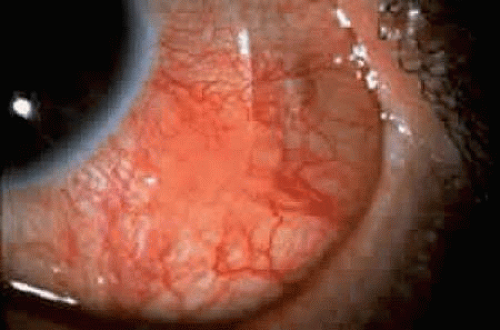 Figure 4. Localized ulcerated conjunctival mound indicated by slit-beam. |
 Figure 5. Diffuse conjunctival hyperemia and edema as an acute manifestation of mucous membrane pemphigoid with ocular involvement (MMPO). |
When evaluating a patient with MMPO, the extent of conjunctival shrinkage should be determined.8 The most useful positions for examination and photography include upward gaze with the lower eyelid retracted and downward gaze with the upper eyelid retracted. The staging system of Mondino and Brown20 is based on the percentage of conjunctival shrinkage (Fig. 6).3 The staging system of Tauber et al.21 describes conjunctival destruction, as follows:
Stage I—chronic conjunctivitis and subepithelial fibrosis
Stage II—early forniceal foreshortening
Stage III—the development of symblephara
Stage IV—ankyloblepharon formation and a frozen globe.
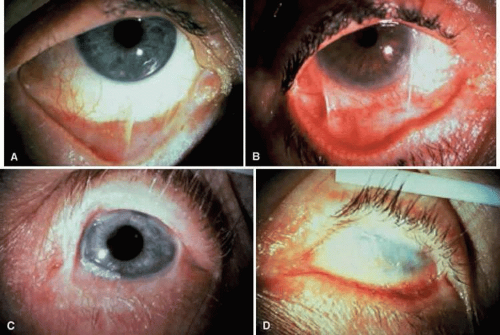 Figure 6. Staging system of membrane pemphigoid with ocular involvement (MMPO). A: Stage I, showing 25% or less shrinkage of the conjunctival fornices. B: Stage II, showing 25% to 50% conjunctival shrinkage. C: Stage III, showing conjunctival shrinkage of about 75%. Inferior fornix is nearly obliterated. Shallow superior fornix is still present. D: Stage IV or end stage of MMPO, showing obliteration of conjunctival fornices. |
A patient with MMPO is more likely to have a dry eye, corneal vascularization, trichiasis, and positive eyelid and conjunctival cultures as the disease progress from one stage to another (Table 1).2
TABLE 1. Correlation of Clinical Data With Stage in Patients With Mucous Membrane Pemphigoid | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
In addition to staging the extent of conjunctival shrinkage that has taken place, it is important to assess the degree of conjunctival inflammation. Stage and level of inflammatory activity are important parameters to assess but are not necessarily correlated. For example, an eye at stage IV may show no conjunctival inflammatory activity, whereas an eye at stage II may show severe conjunctival inflammatory activity. MMPO may be asymmetric in severity (i.e., both eyes may not be at the same stage) and disease progression (i.e., disease in both eyes may not necessarily progress or fail to progress to another stage).20 Although disease in most eyes does progress over time, untreated disease may demonstrate significant variability as eyes in all stages may not progress, although progression is more likely to occur in more advanced stages (Table 2).
TABLE 2. Differential Diagnosis of Bullous Diseases | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Because early detection of disease progression may aid in the management of the disease, especially in the early stages, disease progression should be determined by clinical examination and comparison with previous external ocular photographs.12,20 Progression is defined as increased conjunctival shrinkage, which may involve forniceal foreshortening, the development of new symblephara, or enlargement of an existing symblepharon. As detecting progression of disease may be difficult, Rowsey et al.22 have proposed a relatively objective means of detecting progressive forniceal foreshortening. The method that they have described involves measuring the distance between the limbus and the edge of conjunctiva at the inferior lid margin (with the lower eyelid retracted) in millimeters (mm) in three gazes: straight up, up and left, and up and right. The sum of these measurements is compared between visits and a decrease of more than 3 mm is considered indicative of disease progression.
Histopathologic Findings
Mucous membrane pemphigoid is characterized by subepithelial blisters or bullae. Electron microscopy studies show that the separation at the margin of a blister is located within the lamina lucida between the plasma membrane of the basal cells and the electron-dense lamina densa. Immunoelectron microscopy demonstrates the presence of immune deposits in both the lamina lucida and lamina densa.8,23,24 The conjunctival epithelium in MMPO shows squamous metaplasia, parakeratosis, keratinization and scarce or lacking goblet cells.15,25 Smears of conjunctival scrapings from patients with MMPO reveal neutrophils, keratinized squamous cells, and eosinophils (Fig. 7).26,27
 Figure 7. Conjunctival biopsy from patient with membrane pemphigoid with ocular involvement (MMPO) showing squamous metaplasia, absent goblet cells, and mononuclear cells beneath conjunctival epithelium (hematoxylin and eosin, original magnification ×300). |
In the early stages of conjunctival disease, granulation tissue is found beneath the conjunctival epithelium, with an infiltration predominantly of lymphocytes and plasma cells, with occasional eosinophils and relatively few neutrophils.26,27 In acute manifestations of MMPO, numerous neutrophils, macrophages, Langerhans’ or dendritic cells and T lymphocytes are observed within and beneath the conjunctival epithelium (Fig. 8).5,19,28 In the chronic phase of the disease, only mild infiltration of macrophages and T cells is seen, but pronounced fibrosis takes place in the conjunctival stroma, which is responsible for the conjunctival shrinkage that characterizes the disease.13,14 The molecular mechanisms of conjunctiva fibrosis are still largely unclear, although hyperproliferation of conjunctival fibroblasts from patients with MMPO has been demonstrated in tissue culture.29 Evidence suggests that early stage of scarring might result from inflammation mediated by inflammatory or activated conjunctival cells.30 Continuous remodeling of the extracellular matrix stimulated by fibrogenic cytokines might also be an essential process in the conjunctival scarring in the chronic phase of MMPO.30,31,32,33
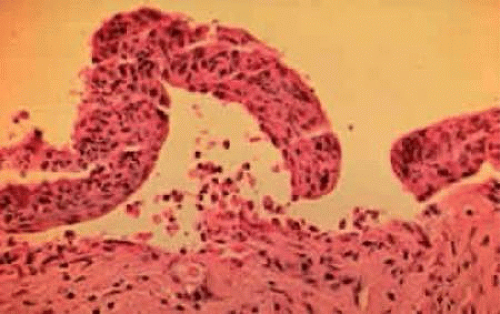 Figure 8. Subepithelial bulla with neutrophils within and beneath the conjunctival epithelium (hematoxylin and eosin, original magnification ×400). |
Immunopathologically, MMPO is characterized by the linear deposition of immunoglobulins (mostly IgG) and components of both the classic and alternative complement pathways on the BMZ of skin and mucosa.34,35 This is in contrast to pemphigus in which IgG is found within the epithelial layer on the epithelial cell membrane. Conjunctival biopsies taken from patients with MMPO demonstrate immunoglobulins and complement bound to the basement membrane (Fig. 9).36,37,38,39,40,41,42 Antibodies may be directed against specific T-cell antigens expressed in the conjunctival epithelium and basement membrane, and circulating serum antibodies against the BMZ have been found in up to 50% of patients with MMP (Fig. 10).5,6,37,38,42,43,44,45 It is thought that binding of these autoantibodies to the BMZ activates the complement pathway, initiating the inflammatory cascade.
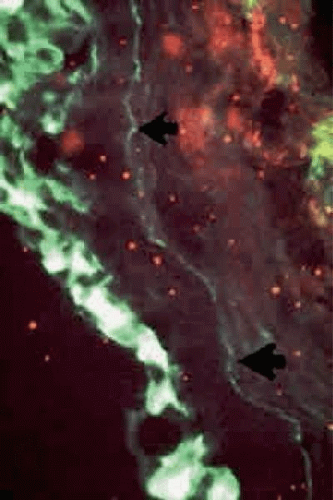 Figure 9. Direct immunofluorescence shows linear deposition of IgA along basement membrane zone of conjunctiva (arrows). IgA deposition is also seen in overlying epithelium. |
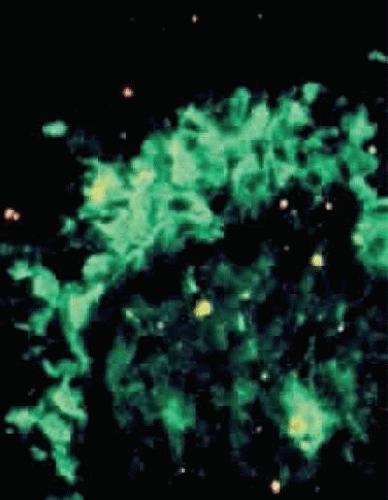 Figure 10. Direct immunofluorescence shows IgM deposition in conjunctival epithelium. |
Many components of the BMZ are recognized by autoantibodies, although only some of them have been identified at the molecular level. The predominant antigens in MMPO include BP230 (BP antigen I) and BP180 (collagen XVII/BP antigen II),46,47,48 laminin 5 (epiligrin),49,50,51,52,53,54 laminin 6,51,52,55 the β4 subunit of α6β4 integrin,56,57 and type VII collagen.58 An animal model of subepithelial blistering diseases has been developed using antilaminin antibodies in neonatal mice.55 The destruction of laminin, which normally binds basal epithelium to its basement membrane, leads to blister formation.51 Progressive destruction causes fragmentation of the basement membrane and subsequent repair with aberrant forms of basement membrane collagen.59 Co-incubation of anti-β4 integrin autoantibodies from patients with MMPO with normal human conjunctiva leads to BMZ separation, indicating a pathogenic role for these autoantibodies in the process of blister formation.60 About half of patients with MMPO have elevated serum IgA levels and IgA deposition in tissue.38,43,61 The presence of a dual circulating antibody response with IgG and IgA might be associated with more severe and persistent disease.62 No definite proved correlation, however, exists between the clinical phenotype and specific target antigens or classes of autoantibodies, supported by the observation that anti-laminin 5 antibodies have been detected in patients with MMPO with minimal and severe scarring.63 Whether these autoantibodies are pathogenic might be related to the particular antigen(s), and more likely, the specific epitope to which these autoantibodies bind.
Many different types of inflammatory cells are detected in all stages or phases of the disease. Perivascular inflammatory cell infiltration is observed in 20% of specimens, including substantial mast cell participation and degranulation.5,64 The conjunctiva of patients with MMPO shows an increased number of specific T lymphocyte subsets, with more helper T cells than suppressor T cells within the epithelium and substantia propria.30,65 A recent study has identified autoreactive T cells that recognize the same region of BP180 as the autoantibodies.66 The presence of costimulatory molecules locally may upregulate T-cell activity.67 Thus, a new concept that autoreactive T cells recognizing components of the BMZ, such as BP180, initiate autoantibody production by B cells has emerged.
Macrophages are the next most common cell type found in the substantia propria, followed by B cells and plasma cells.68 Decreased serum levels of interleukin-6 and increased serum levels of tumor necrosis factor-alpha (TNF-α) may be present.35,69 Studies showing the presence of transforming growth factor-beta 1 and 3, IL-2, IL-4, β-fibroblast growth factor, and connective tissue growth factor suggest that these cytokines might play a role in the formation of fibrosis.32,33,68,70
Differential Diagnosis
Drug-induced conjunctival scarring, which may closely resemble MMPO, has been associated with topical drugs such as idoxuridine,73 echothiophate iodide,73 pilocarpine,74 demecarium,74 epinephrine,75 and timolol,76 as well as the systemic drugs practolol77 and penicillamine.78 Drug-induced conjunctival shrinkage may be self-limited or progressive,79 although affected patients do not have extraocular involvement of mucous membranes or skin.73,74,79,80 Patients with drug-induced conjunctival shrinkage that is progressive and demonstrates immunoglobulins bound to conjunctival basement membrane should be considered as being affected with MMPO; in such a case, the taking of a drug and the development of MMPO may be coincidental, or the drug may accelerate the development of MMPO, which would have developed later anyway.
A practical approach to the problem of drug-induced conjunctival scarring is to discontinue the topical agents if possible, and follow the patient for persistent conjunctival inflammation or progressive conjunctival shrinkage. Alternative glaucoma agents could be used, such as a prostaglandin analog or an adrenergic agonist, which have not been associated with conjunctival scarring. Conjunctival biopsy with immunohistopathologic studies should be considered to rule out MMPO if progressive conjunctival scarring is observed.
Conjunctival scarring can result from irradiation and severe chemical burns, especially alkali. Symblephara have also been reported with Sjögrens syndrome,81 atopic keratoconjunctivitis, and sarcoidosis,82 but not to the extent and not with the relentless progression of MMPO. Conjunctival scarring can develop in association with scleral buckles and conjunctival squamous cell carcinoma, but these conditions are usually unilateral. Scleroderma can be associated with a dry eye and progressive conjunctival shrinkage.83 Trachoma causes conjunctival scarring, but this usually begins and predominates in the superior fornix and the upper palpebral conjunctiva.
A membranous conjunctivitis that results in conjunctival scarring can be caused by adenovirus types 8 and 19, a primary infection of herpes simplex virus, diphtheria, or β-hemolytic streptococcus.40,84 The acute, self-limited nature of these infections contrasts with the chronic, progressive conjunctival shrinkage found with MMP.
Other bullous diseases usually do not cause much diagnostic confusion with MMPO (Table 2). Bullous pemphigoid and pemphigus do not usually cause conjunctival scarring.42,85 An acute episode of EM major or SJS/TEN may cause conjunctival shrinkage but the shrinkage is not chronically progressive, as it is with MMPO.
Mucous membrane pemphigoid and bullous pemphigoid can be associated with malignancy as paraneoplastic syndrome. These neoplasms include bronchogenic squamous cell carcinoma,86 gastric carcinoma,87 renal cell carcinoma,88 and lymphoid malignancy.89,90 A recent series showed a 29% occurrence of solid tumors in patients with MMP carrying anti-lamina 5 IgG antibodies,91 although the exact relationship of antilamina 5 antibodies and malignancy has yet to be elucidated.
Treatment
Artificial tears should be used to treat the dry eye associated with MMPO. Artificial tears without preservatives may be necessary if the preservatives in commercial tear preparations irritate the eyes or if allergies develop to them. Punctal occlusion can be performed if the puncta have not already been occluded by scarring. MMPO can be complicated by secondary bacterial blepharoconjunctivitis. The staphylococcal blepharitis that frequently accompanies this condition may be treated with eyelid scrubs followed by an antibiotic ointment, such as erythromycin or bacitracin. Oral tetracycline or doxycycline may be useful in the treatment of meibomian gland dysfunction.
In the presence of sufficiently deep fornices, therapeutic soft contact lenses may be used in selected patients to protect the corneal epithelium from trichiasis and drying. Some patients with MMPO develop limbal stem cell deficiency as a result of chronic conjunctival inflammation, with secondary recurrent corneal epithelial defects that are painful and, in some cases, may require continuous use of a bandage soft contact lens, amniotic membrane graft, or coverage of the cornea with a conjunctival flap. Artificial tears may need to be used frequently to prevent desiccation of the contact lens, and because patients who have dry eyes and wear contact lenses are at increased risk of infection, these patients must be followed up at regular intervals. Cryotherapy or electrocautery using a hyfrecator may be performed to eliminate trichiasis, and associated entropion may be corrected with the appropriate eyelid surgery.
Foster et al.37 and Mondino and Brown20 found that long-term systemic immunosuppressive therapy suppressed conjunctival inflammatory activity and inhibited progression of conjunctival shrinkage. The response to treatment depends on the stage of disease. Patients with disease at an early stage are less likely to have their disease progress and more likely to respond to systemic immunosuppressive therapy than those with advanced disease (Table 3).2 Topical therapy with steroids, cyclosporine, and retinoids has not been demonstrated to be effective in controlling ocular inflammation and progressive conjunctival scarring, however.
TABLE 3. Number of Eyes Showing Progression of Conjunctival Shrinkagea in Control and Treatment Groups (Mean Follow-up, 2 Years) | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


