Fig. 14.1
(a) Posterior segment photograph of peripheral retinal vessels (b) Ocular coherence tomography (OCT) of retinal layers
14.3 Posterior Segment Surgery
Posterior segment surgery is relatively more difficult and requires various modifications of standard techniques to overcome the obstacles these eyes pose to achieving adequate visualization, exposure, and hemostasis. “Open-sky” approaches were initially favored for their obvious advantages of visualization and access; however, closed system techniques have quickly replaced them as the standard of care for surgical intervention. An initial series published in 2002 described successful posterior segment surgical intervention in 22 eyes, including a modified trans-eyelid technique for pars plana vitrectomy (PPV) in patients with Boston type 2 keratoprostheses [6]. Ten years later, after significant advances in vitreoretinal surgery, the same group reported results from an even larger series of retinal surgeries in patients with KPro, highlighting the more common indications for surgery, as well as documenting the success of surgeries using 23- and 25-gauge surgical techniques [7]. Of the 23 procedures, 15 of the vitreoretinal procedures were in the eyes with a preexisting KPro (including 1 KPro removal), 7 were performed at the time of KPro placement, and 1 was an exploratory endoscopy prior to KPro placement. The most common indication was for retro-KPro membrane (RPM); however, other pathologies treated included retinal detachment (RD), epiretinal membrane (ERM), vitreous opacities, endophthalmitis, revision of previous surgeries (subluxated intraocular lenses and glaucoma shunts), and preoperative endoscopic evaluation of the posterior segment.
From their surgical experience, highlighted points included:
A preference for a valved, trocar-based technique, as opposed to open-sky, even when performing vitrectomy at the time of initial KPro placement. The authors cite a reduced theoretical risk of choroidal hemorrhage, as well as the ability to adjust the position of surgical approach (as they used a temporal approach with one patient). Additionally, smaller-gauged instruments help preserve the conjunctiva in these scarred eyes and may be amenable to sutureless, self-sealing techniques.
The possible benefit of prophylactic vitrectomy at the time of initial KPro placement to reduce the risk of RPM formation (see below).
Extensive anterior segment scarring in the majority of eyes treated with KPro necessitates certain adjustments in technique, such as changes in sclerotomy placement (due to lack of clear limbal landmarks), greater care in assuring a strong implant-host junction (to prevent downgrowth), and deeper scleral depression during peripheral examination [3]. Each case dictates its particular variables; however, the core vitreoretinal surgical principles remain. The retina surgeon can, thus, approach the treatment of posterior disease—even surgical treatment—with reasonable confidence. The most common entities to be encountered will be discussed here.
14.4 Retro-KPro Membranes
One of the most common complications addressed by the retinal surgeon in the population of patients with KPros is the retroprosthetic membrane (RPM) (Fig. 14.2), which has been reported to occur in 25–65 % of patients [10]. These membranes form as a result of both epithelial and stromal downgrowth, with occasional comingling of other iris and lenticular elements [10]. Of these RPMs, approximately half have been noted to be sufficiently sight limiting so as to require treatment, most commonly with the application of neodymium:YAG laser to perform a capsulotomy [10]. However, as seen in some series, these membranes can be thick enough to resist YAG capsulotomy or can regrow after initial capsulotomy, thereby necessitating more definitive surgical treatment.
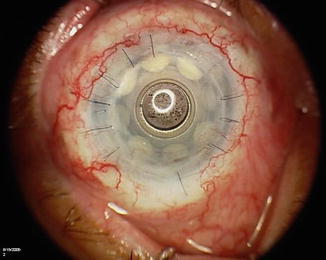
Fig. 14.2
Retroprosthetic membrane behind optic of KPRO Type I
In many cases, complete removal/replacement of the KPro has been used effectively to address RPMs. However, one series—citing the demonstrated risks of RD [3] and intraocular inflammation associated with YAG laser treatment and avoiding the extensive surgery associated with full removal of the KPro—successfully used small-gauge vitrectomy techniques to remove RPMs [7]. In aphakic eyes, this was reportedly performed with relative ease; however, pseudophakic eyes required precise entry into the space between the prosthetic and the lens, risking damage to or displacement of both implants, and greater care should be exercised by the retinal surgeon in these cases.
Interestingly, the same series reported 47 % of their patients with prior KPro developed an RPM, whereas in the population of patients undergoing vitrectomy at the time of initial KPro placement, only 14 % developed RPM [7]. Potentially, removal of proinflammatory materials at the time of initial surgery, including removal of preexisting intraocular lenses (IOL), decreases the incidence of these membranes, and the authors of this series advocate both for their KPro patients. Thus, the question stands as to the possible need for posterior segment intervention in all, or at least a select population of, KPro patients at the time of initial surgery.
14.5 Vitreous Pathology
The vitreous is often neglected in the consideration of KPro complications yet is a common site for subsequent infectious and inflammatory pathology, as well as sight-limiting vitreous opacities. Apart from the feared complication of endophthalmitis, which will be addressed below, patients have been reported to experience episodes of noninfectious vitritis months to years after KPro placement, with acute diminishing of visual acuity in the setting of little to no pain or conjunctival injection [11]. This vitritis usually resolves with medical anti-inflammatory therapy but often requires a vitreous tap to definitively exclude infection; standard vitrectomy techniques can also be used to provide vitreous samples or debulk infectious organisms, as seen in reported cases of endophthalmitis and lymphoma [6, 7, 12]. Vitreous hemorrhage (VH), most often occurring at the time of initial KPro placement, almost always clears spontaneously, although vitrectomy remains an option for non-clearing VH [3] (Fig. 14.3).
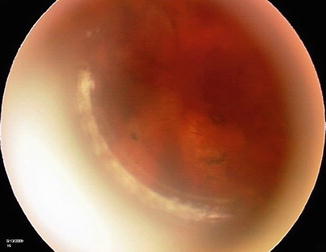
Fig. 14.3
Clearing Vitreous Hemorrhage
Vitrectomy may also be indicated for the removal of sight-limiting vitreous opacities. These opacities can represent proinflammatory materials from the preoperative period, surgical debris, or inflammatory changes, and they can cause significant degradation of the patient’s visual acuity. One series reported six cases of vitreous opacities in the setting of KPro, all treated successfully with small-gauge PPV. Significant improvement of vision was noted in some patients, although final visual acuity was often limited by concomitant retinal pathology [7].
14.6 Retinal Detachments
In one of the largest series of KPro patients published, the most common posterior segment complication was RD (Fig. 14.4), with an incidence of 16.9 % (a number that included rhegmatogenous, tractional, and serous retinal detachments), occurring on average at approximately 10 months after KPro surgery [3]. Rhegmatogenous detachments, specifically, have been reported to occur in 3.5–11.8 % of KPro patients and can be repaired in the majority of cases with good anatomic success. Scleral buckling procedures are likely of minimal benefit, given the presence of extensive anterior segment scarring, so vitrectomy is the preferred method for repair [6]. Tamponade, with silicone oil or PFO, is often warranted [3]. As with all retinal detachment surgery, achievement of anatomic success is limited by the presence of chronic retinal scarring or proliferative vitreoretinopathy (PVR), and visual outcomes tend to be worse in these cases [3, 6, 7].
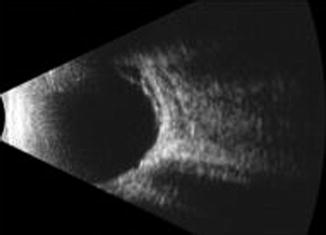
Fig. 14.4
Ultrasound of retinal detachment on KPRO Type I
Patients with KPro require careful examination for retinal tears, especially in the setting of extensive YAG membranotomy [3, 6]. As mentioned above, careful peripheral examination with scleral depression, using somewhat deeper depression, helps to account for anterior segment scarring when examining these patients. However, visualization of the periphery remains difficult in the setting of KPro. In the largest series of patients described, only three retinal tears (of 83 patients) were detected, and all three were detected intraoperatively, with only one patient symptomatically noting “flashing lights” [3].
Choroidal detachments can also develop in eyes with KPro, in as many as 17 % of patients (although more commonly reported rates are approximately 3–5 %), and usually do so in the setting of hypotony [3]. Detection is by indirect ophthalmoscopy or UBM. Earlier choroidal detachments occur in the first postoperative month in hypotonous eyes, often those with a history of concomitant tube shunt placement, and almost always resolve spontaneously. Later choroidal detachments tend to occur in eyes complicated by late corneal necrosis and perforation, with subsequent hypotony [3].
14.7 Hypotony
Chronic hypotony has been reported in eyes with KPro, with an incidence ranging widely from 0 to almost 20 %—precise diagnosis being hindered by its inevitable dependence upon digital palpation and the discovery of associated signs, such as choroidal detachments [13] (Fig. 14.5a, b). It can occur in the setting of tissue necrosis around the prosthetic implant, chronic retinal detachments, and over-filtering glaucoma implants (both valved and non-valved), although the only finding associated with chronic hypotony is the presence of a RPM [13]. The same series to report this association did not find increased risk with age, presence of glaucoma drainage devices, or a history of multiple corneal transplants prior to KPro [13].
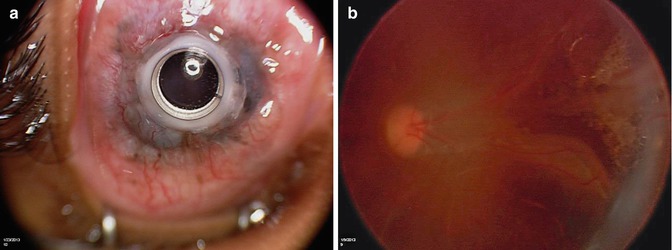
Fig. 14.5
Chronic Hypotony. (a) external photo with of chroroidal detachment viewed through KPRO Type I, (b) Fundus view
Chronic hypotony remains a challenging complication to treat: revision of KPro may be warranted in the setting of anterior segment tissue necrosis and extrusion (Fig. 14.6). Ligation of filtering tubes ab externo can be attempted if over-filtration is suspected; however, this does not always prove successful [13]. Chronic choroidal and exudative retinal detachments can result and are difficult to treat, often only part of an overall progression to phthisis bulbi that is difficult to avert [13]. Pars plana vitrectomy with silicone oil tamponade has been used in conjunction with KPro for hypotonous eyes with some success in preventing progression to phthisis and can be attempted in eyes already having KPro [8, 9].




