Blepharoplasty
Robert M. Dryden
Craig M. Davis
Blepharoplasty is a surgical procedure performed on the upper or lower lids that may excise skin, muscle, or fat. It can be cosmetic, to afford a more youthful appearance to the eyes, or functional, to improve visual function. It is always advisable to follow general guidelines for preoperative evaluation and surgical technique, individualizing each case to achieve a pleasing aesthetic outcome and to decrease the risk of developing complications such as ectropion, entropion, lid retraction, and exposure keratopathy.
Preoperative Considerations
The blepharoplasty candidate has certain expectations for the results of surgery. The patient and surgeon must have a common goal and understanding in this regard. The patient must realize that cosmetic blepharoplasty is not a panacea for other social problems and that the final outcome may be subtle or dramatic depending on how much “excess baggage” there is. Ideally, an emotionally sound patient desires surgery to enhance an already positive self-esteem and overall healthy body image. On the other hand, a functional blepharoplasty candidate hopes to alleviate dimmed vision or an impaired visual field. In either case, the patient should not consider the surgery to be minor, and the surgeon must not de-emphasize associated risks and potential complications. A well-documented informed consent written in lay terms should include not only the worse possible, albeit rare, outcomes of death, blindness, and severe exposure but also the relatively more common outcomes of residual excess skin or fat, bruising, ectropion, asymmetry, scarring, transient lagophthalmos, eyelid retraction, and enhanced scleral show. Before surgery, a complete medical history should be obtained with emphasis on cardiac, pulmonary, renal, metabolic, allergic, and thyroid status. Any abnormal bleeding tendencies are evaluated, and the patient is instructed to stop taking all antiprostaglandin agents 2 weeks before surgery.1 In an effort to enhance the healing process, it is also advisable for patients to stop smoking.2 Preoperative ancillary tests are guided by the patient’s age and medical history with medical clearance obtained before surgery if indicated.
Preoperative Evaluation
The preoperative assessment should entail an evaluation of all factors that might influence the desired outcome. A visual acuity must be documented regardless of the surgeon’s subspecialty. Visual field testing should be used to document a visual field defect in the patient undergoing a functional blepharoplasty. The visual field defect should improve by excising the excess skin, since similar field defects may result from other causes, such as glaucoma or ischemic optic neuropathy. The patient must relax the brow during testing because a compensating overacting frontalis may artifactually enlarge the field. The method we prefer to use is the tangent screen, which utilizes standardized wands at specified distances, since this can be done quickly and easily in the office.
The entire face is examined with particular attention paid to involutional periorbital changes. Subjective quantification of dermatochalasis and steatoblepharon and the presence of blepharochalasis should be determined. Dermatochalasis is redundant, baggy eyelid skin (Fig. 1). Steatoblepharon is orbital fat that bulges or prolapses through a thinned orbital septum (Fig. 2). Although more common in older patients, dermatochalasis can also occur in younger people, particularly if a familial predisposition exists. Dermatochalasis of the upper eyelids is often associated with an indistinct or higher than normal eyelid crease. It also may be associated with true ptosis of the upper eyelids. A coexistent brow ptosis should be recognized. Additional procedures such as blepharoptosis repair or elevation of the brow may be required at the time of surgery. It may be difficult to convince a patient that a postoperative ptosis was indeed present before surgery unless the patient was evaluated specifically for, and informed preoperatively of, this condition. Likewise, a patient will be disappointed if a functional loss persists after blepharoplasty because a ptotic brow or aponeurotic dehiscence was the true culprit. Significant dermatochalasis of the upper lids leads to complaints of a heavy feeling around the eyes, brow ache, complaint of eyelashes in the visual axis, and, eventually, reduction in the superior visual field. This is often made worse by associated brow ptosis, especially if patients do not use their frontalis muscle to elevate the brows to relieve visual obscuration by the excess skin. Although blepharochalasis is not an involutional change, it is included in this discussion because it can simulate, and must be differentiated from, dermatochalasis. Blepharochalasis is a rare familial variant of angioneurotic edema occurring in younger persons that is characterized by idiopathic episodes of inflammatory edema of the eyelids. Because of the recurrent bouts of inflammation and edema, the eyelid skin of a patient with blepharochalasis becomes thin and wrinkled, simulating the appearance of dermatochalasis. In addition, true ptosis, herniation of the orbital lobe of the lacrimal gland, atrophy of the orbital fat pads, and prominent eyelid vascularity may be associated with blepharochalasis secondary to the repeated attacks of edema.3 This condition occurs most commonly in young females. Surgical repair of the eyelid skin changes and ptosis that result from blepharochalasis may be complicated by repeated episodes of inflammation and edema, causing recurrence of the ptosis and other eyelid changes. Lower eyelid dermatochalasis is considered a cosmetic issue unless the excess skin and prolapsed fat is so severe that the patient cannot be fit with corrective lenses.
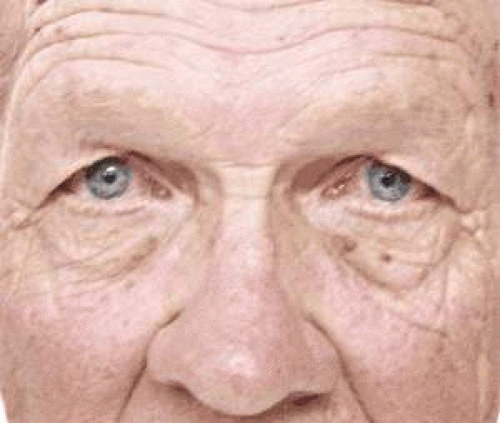 Fig. 1. Dermatochalasis of upper eyelids. |
 Fig. 2. Steatoblepharon of upper and lower eyelids. The patient also has coexistent dermatochalasis and upper eyelid ptosis. |
There are two primary fat pockets in the upper lid, the nasal and the central, with the nasal, Bourrelet senilis, being the more prominent. Clinically, nasal compartment fat is paler in color and has a firmer consistency than central compartment fat. The central pocket consists of preaponeurotic fat and overlies the levator aponeurosis. Nasal fat contains a higher proportion of collagen and elastin, with increasing density of both closer to the trochlea. Preaponeurotic fat of the central pocket displays less collagen and elastin anterior to the Whitnall ligament.4 A higher lutein and beta-carotene content in preaponeurotic fat contributes to the color discrepancy between the compartments.5 The lower lid contains two anterior compartments as well, with the medial being the more prominent.
The examination should then focus on specific findings that might increase the risk of complications, such as ectropion, entropion, or exposure keratopathy (Fig. 3). One should evaluate for increased horizontal lid laxity or dehiscence of the lower lid retractors.6 The latter is confirmed when the tarsus remains vertical instead of turning out when the lower lid is pulled down and is associated with an abnormal white line in the fornix. If necessary, a horizontal tightening procedure, with or without retractor repair, may be incorporated at the time of lower lid blepharoplasty. Any history of dry eyes or clinical finding of lagophthalmos, lid retraction, altered blink, or punctate corneal staining may necessitate further evaluation of the tear breakup time and tear output, since additional exposure may be detrimental to an already compromised cornea. Preoperative and postoperative photographs are an integral part of the patient’s medical record (Fig. 4). They serve as a learning instrument to the surgeon and are paramount in documentation for medicolegal and insurance purposes. By making certain that the patient’s brow is relaxed and the excess skin is illustrated, photographs will reinforce findings on clinical examination and visual field testing. Preoperative digital images or 35-mm photographs are taken and repeated 1 to 2 months after surgery. A Polaroid photograph taken before surgery is useful during surgery and for immediate use.
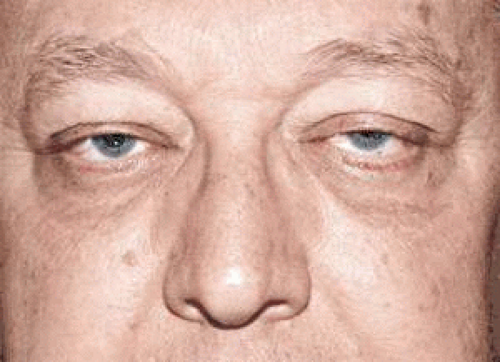 Fig. 3. Preoperative examination revealed left lower eyelid retraction (increased scleral show) and upper eyelid ptosis in this patient. These findings should be documented and discussed with the patient prior to surgery. |
 Fig. 4. Preoperative (top) and postoperative (bottom) photographs are an integral part of the patient’s record. |
Technique for Upper Lid Blepharoplasty
The patient is prepped and draped so that the lids are in their natural position, avoiding undue tension and distortion of the surrounding skin. The patient is asked to look up and down to accentuate the upper lid creases. If the creases are symmetric and in a normal position, they may be used to mark the proposed lower portion of the incision. If they are absent, asymmetric, or high, as may be found with an aponeurotic defect, a new lid crease will need to be created. The height of the new crease may be guided by surgeon or patient preference, a normal contralateral crease, or race. The usual crease in the non-Asian is 10 mm from the lid margin at the midpupillary line. A preincisional marking is then extended toward the medial and lateral canthi as a gently sloping curve matching the configuration of the natural lid crease. A vertical distance of 4 to 6 mm should separate the line from both canthi. At the lateral canthus the line turns slightly upward to continue in a pre-existing crease (Fig. 5). The distance the mark extends laterally is guided by the amount of excess skin and the crease that it forms. The amount of skin to be excised is then determined by placing one tip of a Castroviejo forceps on the lid crease mark in the midpupillary line while the other tip rests more superiorly on the lid. The teeth are gently brought together while another forcep is used to grasp and pull excess skin up between the jaws of the other forceps (Fig. 6a and b). The endpoint is that amount of skin that can be grasped just before the upper lid margin everts. A mark is placed at that point and is extended in both directions to join the lower line, complementing any nasal or lateral upward slope (Fig. 7a and b). The patient is then asked to look up, and, if marked correctly, the lines of the proposed upper and lower incisions should nearly touch. A limiting distance of 1 cm from the lower border of the brow is used for the upper incision to avoid the unpleasant effect of approximating the brow too close to the lid margin. If one brow is carried higher, a compensatory drop of the superior incision line is appropriate. Next, infiltrative anesthesia is given with gentle pressure applied to aid in diffusion. If the patient is receiving monitored anesthesia care, propofol (Diprivan) or methohexital (Brevital) is given while 0.5% bupivacaine with epinephrine 1:200,000 is injected. However, if the patient is receiving little or no sedation, two injections are given. Buffered 1% lidocaine precedes the bupivacaine and epinephrine mixture. The added bicarbonate not only accentuates onset but also decreases pain, while the extended duration of action of bupivacaine alleviates discomfort in the immediate postoperative period.7,8,9 While gentle traction is applied, a single continuous skin incision is made along the lower and then the upper marks using a no. 15 Bard-Parker blade placed perpendicular to the skin. The skin is then excised either with a combination of sharp and blunt dissection using appropriate scissors or with the electrocautery unit using a fine-tipped cutting needle (Fig. 8a and b). We prefer the control of the Colorado Microneedle (Sryker Leibinger, Kalamazoo, Mich), which is insulated except for the tip and provides an excellent combination of precise cutting of delicate tissues and hemostasis. The skin is placed on the instrument stand over the patient’s chest, and as fat is excised, it too will be arranged in a manner to signify the pocket from which it came so that symmetry of excision may be compared between sides (Fig. 9). Meticulous hemostasis should be achieved during this and every stage of the procedure. A horizontal incision through the orbicularis to the level of submuscular fascia is made just superior to the lower skin incision (Fig. 10a and b). If fat is to be excised, the orbital septum is incised along the most nasal extent of the incision, exposing the underlying fat. The medial upper eyelid fat pad is typically the most prolapsed and can be readily identified by its paler color and firmer texture. It lies between the medial rectus and superior oblique muscles and is separated from the central fat pad by fascial connections continuous with the trochlea. The nasal fat capsule is incised and the fat is gently teased forward and excised with cautery, scissors, or laser (Fig. 11a and b). When performed, resection of the upper lid adipose is carried no deeper than the boundary created by the superior orbital rim. Removal of fat deeper than the rim may result in a hollow superior sulcus. Care must be exercised as the superior oblique muscle may be drawn outward and injured as the fat is teased through the orbital septum. Caution is necessary to avoid significant bleeding in this area, as the medial palpebral blood vessels overlie the medial upper eyelid fat pads.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


