Benign Vocal Fold Lesions and Phonomicrosurgery
John W. Ingle
Clark A. Rosen
Benign vocal fold lesions are a common cause of dysphonia. Their diagnosis and subsequent care can be a complex and important quality-of-life issue to individuals who suffer from this set of disorders. The ability to communicate without dysphonia is important to the population at large for both occupational and social reasons. A growing percentage of the occupations in the world are voice and communication dependent as opposed to labor dependent; thus, it is vital to have the ability to use the voice throughout the day in a clear, efficient manner without voice loss or without causing undue negative attention because of dysphonia (1).
The overriding treatment principle for caring for patients with benign vocal fold lesions is the assessment and improvement of the patient’s functional status regarding an ability to communicate with the voice. Many ways exist to improve the functional status of the voice, including treatment of associated medical conditions, voice therapy (see Chapter 71), and surgery. This chapter is designed to discuss a variety of benign vocal fold lesions that commonly cause dysphonia from the categories of epithelial lesions, lamina propria pathology, and vascular pathology. A large portion of benign vocal fold lesions and subsequent dysphonia arise from lesions of the lamina propria due to presumed greater sensitivity to trauma associated with inflammation, coughing, voice misuse, and/or voice overuse. Over the last several decades, a specialized form of laryngeal microsurgery—phonomicrosurgery—has evolved. The principles and concepts of this type of surgery are presented below.
BENIGN EPITHELIAL LESIONS OF THE VOCAL FOLD
Epithelial abnormalities of the vocal folds are caused by infectious processes (fungal), keratosis of the epithelium, papillomatous growth of the epithelium, or malignant degeneration of the epithelium. Infections, papillomatosis, and cancers of the epithelium of the vocal fold are covered in other chapters of this book (Chapters 66, 67, 94, and 123). Nonmalignant epithelial abnormalities can be grouped under the category of keratosis. Keratosis includes both white (leukoplakia) and red (erythroplakia) lesions of the vocal folds. The terms “leukoplakia” and “erythroplakia” are descriptive only and have no prognostic or diagnostic value. The primary concern of keratotic lesions of the vocal folds is the potential for these lesions to transform from a benign process to a malignant process. The clear etiologic factors for the formation of these lesions and potential for their subsequent transformation is not clear. Irritation from tobacco smoke has been implicated. In addition, vocal misuse and overuse and irritation from refluxed gastric contents (laryngopharyngeal reflux disease) have also been scrutinized and associated with the development of keratotic lesions of the vocal folds.
The diagnosis and treatment of keratotic lesions include a careful diagnostic evaluation including microlaryngoscopy with high-power magnification and excisional biopsy to rule out a malignant process. This is done best using the principles and approaches of phonomicrosurgery, specifically microflap surgery, to remove the keratotic lesion of the vocal fold in a controlled, conservative, subepithelial, and oriented fashion (see below). After a definitive diagnosis has been made, management includes removal of the most common etiologic agents, tobacco smoke exposure, laryngopharyngeal reflux disease, and vocal abuse (see Chapters 21, 66, and 71).
Vocal misuse and overuse can be related to the patient’s phonatory pattern, environment, and overall demands. In addition, a theory of excessive vocal fold collision and impact forces created to attempt to compensate for glottal insufficiency leading to keratosis is held by some. The glottal insufficiency can be caused by vocal fold atrophy, paralysis, paresis, or scarring. Until the underlying glottal
insufficiency is addressed with an augmentation procedure (medialization laryngoplasty or vocal fold injection augmentation), the keratotic activity will persist and recur following excision. Often the glottal insufficiency is not recognized and it results in recurrent keratosis following surgical excision. This theory has never been validated but should be considered in the most recalcitrant cases of keratosis.
insufficiency is addressed with an augmentation procedure (medialization laryngoplasty or vocal fold injection augmentation), the keratotic activity will persist and recur following excision. Often the glottal insufficiency is not recognized and it results in recurrent keratosis following surgical excision. This theory has never been validated but should be considered in the most recalcitrant cases of keratosis.
Close observation and photo documentation of keratotic lesions are essential for long-term care and treatment of patients with this disease. Once infectious and malignant processes have been ruled out, patients can be observed in the office with serial examinations and especially helped with the aid of photo documentation to monitor for any specific change in the nature of the keratotic lesion(s). If the patient does not have significant functional limitation from the keratosis and the lesion is stable, repeated surgical removal is not indicated. Any discrete change in the nature, size, or location of the keratosis should prompt a surgical excision of the keratotic lesion(s) for pathologic review (2).
BENIGN LESIONS OF THE VOCAL FOLD LAMINA PROPRIA
Midmembranous Vocal Fold Lesions
The lamina propria of the vocal fold is a key component to vocal fold vibration and, thus, voice quality depends on the elastic properties of the lamina propria. The lamina propria is frequently injured by direct trauma, such as surgery, radiation therapy, or repeated collisional impact associated with phonation (vocal abuse). Most benign, midmembranous vocal fold lesions caused by trauma occur from repeated injury to the vocal fold lamina propria. Most of these lesions occur in the subepithelial space but also can be found near the vocal ligament. These lesions, which typically occur in the midmembranous vocal fold, are often bilateral. This region of the vocal fold has been termed “the striking zone,” because of the theoretical concept of maximal vocal fold collision or impact forces resulting in their formation (3).
Benign, midvocal fold lesions cannot be defined by morphology and stroboscopy alone. Great difficulty in discussion and management of these lesions stems from the lack of accepted nomenclature for defining the lesions. This has resulted in great confusion and lack of clarity regarding etiology, diagnosis, and treatment. Without being able to clearly define distinct lesions within the larger group of benign vocal fold lesions of the lamina propria, it has been impossible to assess treatment methods and efficacy. To this end, a recent move has been made to implement a rigorous and clearly defined vocal fold lesion nomenclature paradigm (4). This classification scheme defines nine distinct benign midvocal fold lesions: (a) vocal fold nodules; (b) vocal fold polyp; (c) vocal fold cyst-subepithelial; (d) vocal fold cyst-ligament; (e) fibrous mass-subepithelial; (f) fibrous mass-ligament; (g) reactive vocal fold lesion; (h) nonspecific vocal fold lesion; and (i) pseudocyst. Outlined below is a brief description of each of these vocal fold lesions based on their morphologic appearance, stroboscopic pattern, response to voice therapy, and intraoperative findings. Please refer to Figures 68.1, 68.2, 68.3, 68.4, 68.5, 68.6, 68.7, 68.8, 68.9, 68.10, 68.11, 68.12 for some examples of these lesions.
1. Vocal fold nodules are always bilateral and fairly symmetric. Their stroboscopic pattern shows normal or minimal reduction of the mucosal wave activity during stroboscopy. These lesions reduce in size or disappear in response to behavioral modification of voice use (voice therapy). Note any lesions that do not improve with behavioral modification are not vocal fold nodules. Refer to Figure 68.1 for an example of vocal fold nodules.
2. Vocal fold polyps can be unilateral or bilateral lesions and are typically exophytic lesions that are often clear in appearance or associated with a vocal fold hemorrhage and heme colored (hemorrhagic polyp). These lesions have minimal reduction of the mucosal wave vibratory activity on stroboscopy and typically do not change in size in response to voice therapy. Intraoperatively, these lesions are composed of gelatinous unorganized material in the subepithelial space. Refer to Figures 68.2 and 68.3 for examples of vocal fold polyps.
3. Vocal fold cysts can be unilateral or bilateral and located either near the ligament or in the subepithelial space. Practically, the subepithelial space is defined as the region immediately underneath the vocal fold epithelium. When the vocal fold pathology (cyst, polyp, or fibrous mass) is adherent to the undersurface of the microflap as it is elevated, it is located in the subepithelial space. When the pathology is located “deep” to the microflap following cordotomy, the pathology (cyst or fibrous mass) is classified as a ligamentous lesion. A vocal fold cyst does not respond to voice therapy and,
depending on the location (subepithelial or ligament) and size, the stroboscopy pattern is either minimally impaired or significantly impaired (usually ligamentous). The intraoperative finding for a vocal fold cyst is the presence of a lesion with a distinct capsule in either of the above-described locations. Refer to Figures 68.4, 68.5, 68.6 for examples of vocal fold cysts.
depending on the location (subepithelial or ligament) and size, the stroboscopy pattern is either minimally impaired or significantly impaired (usually ligamentous). The intraoperative finding for a vocal fold cyst is the presence of a lesion with a distinct capsule in either of the above-described locations. Refer to Figures 68.4, 68.5, 68.6 for examples of vocal fold cysts.
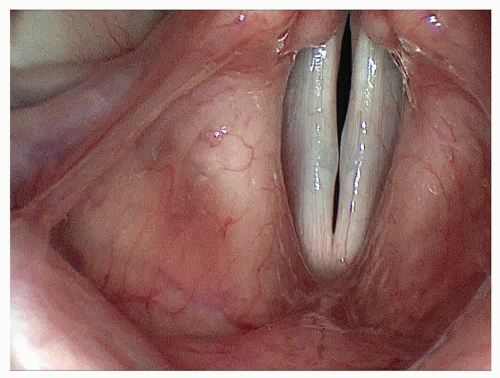 Figure 68.1 Vocal fold nodules. |
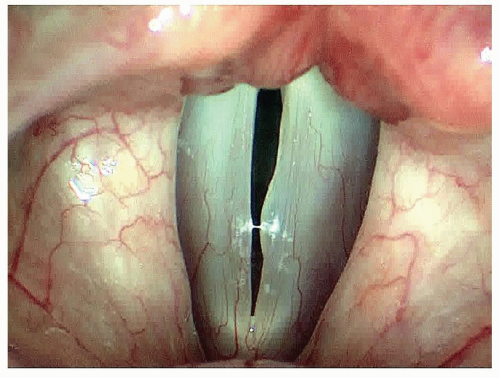 Figure 68.2 Vocal fold polyp. |
4. Fibrous mass of the vocal fold is a lesion that can be unilateral or bilateral and can be located in the subepithelial or ligamentous area. These lesions do not respond to voice therapy and often induce a significant impairment in the mucosal wave activity during stroboscopy. Intraoperatively, the lesion is seen as a fibrous gray, unorganized, unencapsulated lesion in the midmembranous vocal fold in either the subepithelial or ligamentous region. Refer to Figures 68.7, 68.8, 68.9. These lesions often have thin extensions of the “fibrous material,” extending anteriorly or posteriorly toward the anterior commissure or vocal process, respectively.
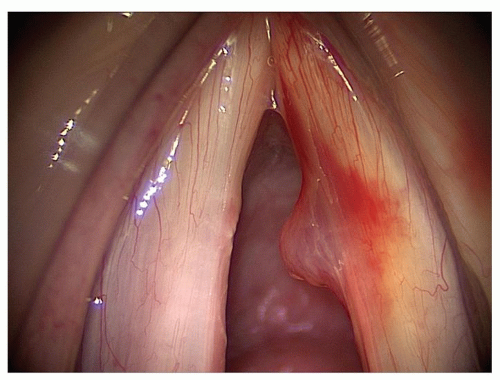 Figure 68.3 Vocal fold polyp (with associated hemorrhage). |
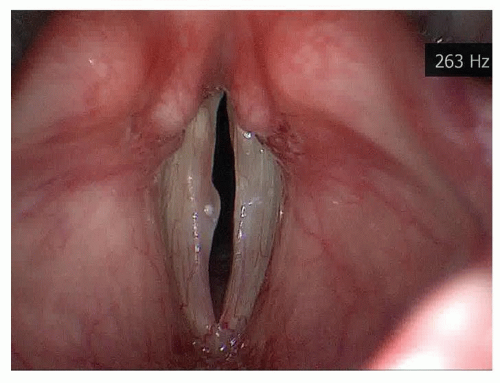 Figure 68.4 Vocal fold cyst-subepithelial. |
5. Reactive Vocal Fold Lesion
A reactive vocal fold lesion has good vibratory characteristics seen on stroboscopy and always occurs in response to a contralateral lesion (vocal fold polyp, vocal fold fibrous mass, vocal fold cyst). Commonly, the reactive lesion has an indentation where the contralateral lesion has created a concavity on the free edge of the lesion due to repeated trauma during vocal fold vibration. This appearance of the two lesions interdigitating with each other during vocal fold closure and vibration is often called a “cup and saucer” deformity. This lesion often will reduce in size with behavioral therapy. Refer to Figure 68.10 for an example of a left true vocal fold reactive lesion associated with a right true vocal fold polyp.
6. Nonspecific vocal fold lesion
Nonspecific vocal fold lesion can be unilateral or bilateral, and is denoted by either subepithelial or ligamentous pathology that is not responsive to nonsurgical interventions (voice rest, medical therapy of comorbidities, and voice therapy) but does not impair function sufficiently to necessitate phonomicrosurgical removal. Thus, when a lesion is classified as a nonspecific vocal fold lesion, the clinician immediately knows that the patient has persistent vocal fold pathology in the face of significant functional improvement and a high functioning level after maximal medical therapy (nonsurgical). Refer to Figure 68.11 to see the vocal folds of a patient who met the clinical criteria for bilateral nonspecific vocal fold lesions.
7. Pseudocyst
Pseudoscyt is a superficial subepithelial pathology that, by definition, corresponds to glottal incompetence most often associated with vocal fold scar but can also be associated with a vocal fold paresis or paralysis. The clinical nature of this lesion includes a very superficial, almost “water blister” appearance of the lesion, with a very thin epithelial covering to the
lesion without any evidence of encapsulation nor negative impact to the mucosal wave of the affected vocal fold. If this lesion is removed surgically without the glottal incompetence being addressed, it has a high likelihood of recidivism. Refer to Figure 68.12 to see an example of a left true vocal fold pseudocyst with associated right true vocal fold scar.
lesion without any evidence of encapsulation nor negative impact to the mucosal wave of the affected vocal fold. If this lesion is removed surgically without the glottal incompetence being addressed, it has a high likelihood of recidivism. Refer to Figure 68.12 to see an example of a left true vocal fold pseudocyst with associated right true vocal fold scar.
 Figure 68.5 Vocal fold cyst-ligament. |
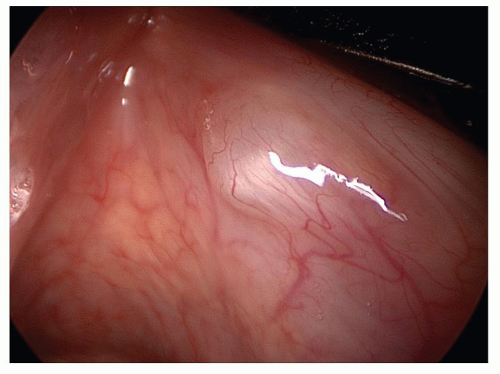 Figure 68.6 Vocal fold cyst-ligament (30-degree telescopic view of same lesion as Fig. 68.5). |
 Figure 68.7 Fibrous mass-subepithelial and bilateral. |
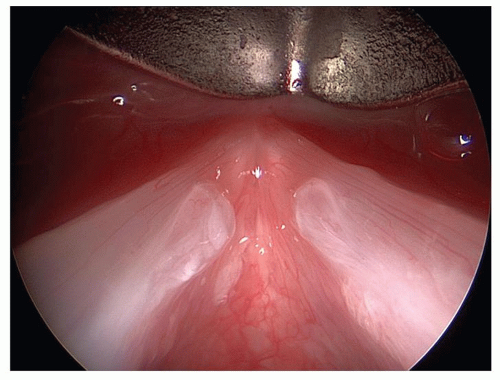 Figure 68.8 Fibrous mass-subepithelial and bilateral (70-degree telescopic view of same lesions as Fig. 68.7). |
The definitive diagnosis of most midmembranous benign lesions of the lamina propria requires evaluation following resolution of any acute inflammatory processes, stroboscopy, voice therapy treatment, and possibly intraoperative findings. The treatment approach for these lesions is fairly standardized, given that most patients should receive nonsurgical treatment for these lesions, which consists of medical therapy for comorbid medical conditions (e.g., allergies, reflux) and voice therapy (see Chapter 71). At the initial evaluation session and after maximal nonsurgical medical therapy, assessment of the patient should include
functional measures and stroboscopy (see Chapter 65). The decision to proceed with surgery, which is highly individualized, should be based on the patient’s voice quality, functional needs, and demands following maximal nonsurgical treatment modalities. After conservative nonsurgical therapy has been implemented, the patient should be asked “can you do what you need to do with your voice at the present time?” If the patient still has significant functional limitations with the voice, then a discussion regarding surgical treatment of the vocal fold lesion(s) is reasonable.
functional measures and stroboscopy (see Chapter 65). The decision to proceed with surgery, which is highly individualized, should be based on the patient’s voice quality, functional needs, and demands following maximal nonsurgical treatment modalities. After conservative nonsurgical therapy has been implemented, the patient should be asked “can you do what you need to do with your voice at the present time?” If the patient still has significant functional limitations with the voice, then a discussion regarding surgical treatment of the vocal fold lesion(s) is reasonable.
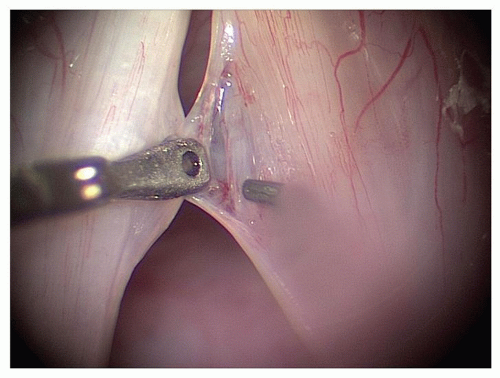 |
 Figure 68.10 Reactive vocal fold lesion of left true vocal fold. |
Another advantage of the above-described vocal fold nomenclature system is that these lesions have different prognostic implications and can be helpful in counseling the patient regarding expected clinical course and treatment outcome. In general, patients with subepithelial pathology have a greater likelihood of excellent vocal fold recovery than do patients with disease within the ligament and, similarly, patients with vocal fold nodules, reactive lesion, and vocal fold polyp have a better prognosis for a high degree of vocal recovery after treatment than do those with a vocal fold cyst and fibrous mass (5).
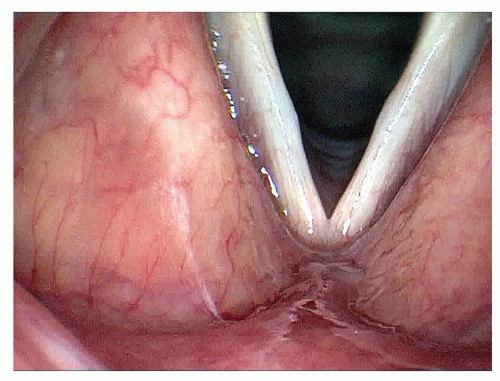 Figure 68.11 Nonspecific vocal fold lesion, bilateral. |
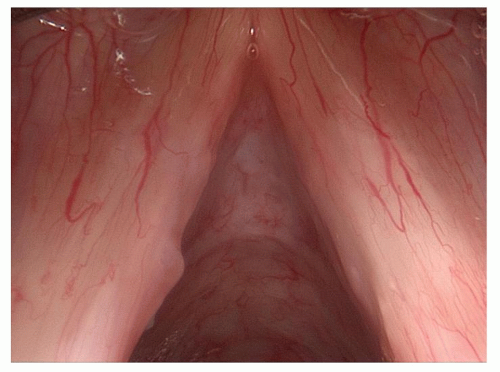 Figure 68.12 Pseudocyst of the left true vocal fold and associated right vocal fold scar defect. |
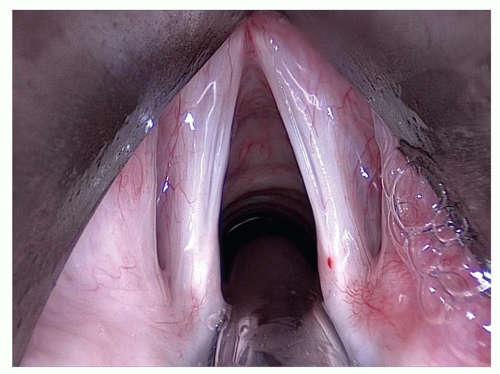
Vocal Fold Scar and Sulcus Vocalis
Vocal fold scar and sulcus vocalis are abnormalities of the lamina propria of the vocal fold that result in poor vocal fold vibratory function (loss of viscoelasticity) and often glottal insufficiency. The former is a hallmark of vocal fold scar and sulcus vocalis, and the latter is dependent on the nature of the vocal fold pathology. For reasons that are unclear, some patients with vocal fold scar develop a “deposition” form of the vocal fold pathology where the normal lamina propria of the vocal fold is substantively taken over (replaced) by thick, fibrous scar tissue that can match the normal size of the lamina propria or can even slightly expand the size of the vocal fold as the vocal fold epithelium becomes adherent to the vocal ligament. The theory behind this form of vocal fold scar involves repeated hemorrhage into the vocal fold, resulting in serial deposition of scar tissue, which eventually replaces and even expands the lamina propria. Other patients with vocal fold scar and all patients with sulcus vocalis have an opposite effect: the lamina propria is reduced or lost during the formation of the disease process without any subsequent replacement at all. This results in a loss of vibratory function and a change in the size and dimension of the vocal fold. These pathologic occurrences cause glottal insufficiency. Limited research has looked at the etiology of vocal fold scar and sulcus vocalis. Clinical reports, however, indicate that most of the patients with these disorders have a history of repeated vocal abuse (phonotrauma). Refer to Figures 68.13 and 68.14 to view the vocal folds of a patient with bilateral sulcus vocalis. There is also a belief that sulcus vocalis can occur as a congenital deformity. These patients have an abnormal sounding cry and abnormal phonation from birth forward and, typically, have a very severe form of sulcus vocalis. The varying degrees and types of deformation that sulcus vocalis can present have been described as either a type I, type II, or type III sulcus vocalis deformity (6).