49 Benign Thyroid Disease • Multinodular, simple (smoothly enlarged), retrosternal goitres • Increased where iodine is deficient • Long-standing may develop clinical or subclinical thyrotoxicosis • Symptoms • Ethnicity • Incidence • Sex • Age • Aetiology – Acute suppurative—bacterial – Chronic—mycobacteria, fungal, and parasitic • Physiological • Pathological—iodine deficiency • Medical treatments – Up to 50% reduction in goitre volume – Risks include: hypothyroidism, Graves – Contraindicated in pregnant women or women wanting to get pregnant within 1 year of treatment – Thyroxine administration decreases TSH leading to a reduction in volume – Risks include: thyrotoxicosis, cardiac arrythmias, thyroid increases to pretreatment size on cessation of thyroxine, osteopenia in long-term thyroxine use – Indicated for thyrotoxic patients, e.g., propylthiouracil (side effects: rash and agranulocytosis) – 50% relapse rate • Retrosternal goitre – Inability to palpate below it – Dullness to percussion over sternum – May only be a small cervical component – Pemberton sign: facial flushing after raising both arms in the air due to compression of jugular veins by thyroid – CT scan good for demonstrating retrosternal extent ± tracheal compression – Spirometry – Conservative (if medically unfit) – Surgery: most can be removed via cervical route (unless below aortic arch) may need cardiothoracic input ± sternotomy – Increasing role of radioactive iodine in euthyroid retrosternal goitre safe to use down to a tracheal diameter of 1 cm • Graves disease – Thyrotoxicosis – Goitre – Eye signs: lid lag, exophthalmos, chemosis – Skin signs: acropachy, pretibial myxedema – Radioactive iodine – Antithyroid drugs, e.g., carbimazole or propylthiouracil – Block and replace: antithyroid drugs full dose + thyroxine to replace thyroid function – Surgery • Solitary toxic nodule • Long-standing MNGs (Plummer disease) • 50% of patients relapse on carbimazole/propylthiouracil—may request thyroidectomy • When considering surgery need to achieve euthyroid state preop with antithyroid medication, β-blockade and Lugol iodine (up to 2 weeks preop)
49.1 Clinical Features
 Neck swelling
Neck swelling
 Dyspnea
Dyspnea
 Dysphagia
Dysphagia
 Choking
Choking
 Stridor
Stridor
49.2 Epidemiology
 No racial predilection exists
No racial predilection exists
 Multinodular goitres is one of the common endocrine conditions, affecting 500 million people worldwide
Multinodular goitres is one of the common endocrine conditions, affecting 500 million people worldwide
 F:M 5:1
F:M 5:1
 In the Wickham study, 26% of women had a goitre compared with 7% of men
In the Wickham study, 26% of women had a goitre compared with 7% of men
 Thyroid nodules are less frequent in men than in women, but when found, they are more likely to be malignant
Thyroid nodules are less frequent in men than in women, but when found, they are more likely to be malignant
 The frequency of goitres decreases with advancing age
The frequency of goitres decreases with advancing age
 The decrease in frequency differs from the incidence of thyroid nodules, which increases with advancing age
The decrease in frequency differs from the incidence of thyroid nodules, which increases with advancing age
 Iodine deficiency
Iodine deficiency
 Autoimmune thyroiditis—Hashimoto or postpartum thyroiditis
Autoimmune thyroiditis—Hashimoto or postpartum thyroiditis
 Excess iodine (Wolff–Chaikoff effect) or lithium ingestion, which decrease release of thyroid hormone
Excess iodine (Wolff–Chaikoff effect) or lithium ingestion, which decrease release of thyroid hormone
 Goitrogens, e.g., propylthiouracil, lithium, carbamazepine
Goitrogens, e.g., propylthiouracil, lithium, carbamazepine
 Stimulation of thyroid stimulating hormone (TSH) receptors by TSH from pituitary tumours, pituitary thyroid hormone resistance, gonadotropins, and/or thyroid-stimulating immunoglobulins
Stimulation of thyroid stimulating hormone (TSH) receptors by TSH from pituitary tumours, pituitary thyroid hormone resistance, gonadotropins, and/or thyroid-stimulating immunoglobulins
 Inborn errors of metabolism causing defects in biosynthesis of thyroid hormones
Inborn errors of metabolism causing defects in biosynthesis of thyroid hormones
 Exposure to radiation
Exposure to radiation
 Deposition diseases
Deposition diseases
 Thyroid hormone resistance
Thyroid hormone resistance
 Subacute thyroiditis (de Quervain thyroiditis)
Subacute thyroiditis (de Quervain thyroiditis)
 Silent thyroiditis
Silent thyroiditis
 Riedel thyroiditis
Riedel thyroiditis
 Infectious agents
Infectious agents
 Granulomatous disease
Granulomatous disease
 Thyroid malignancy
Thyroid malignancy
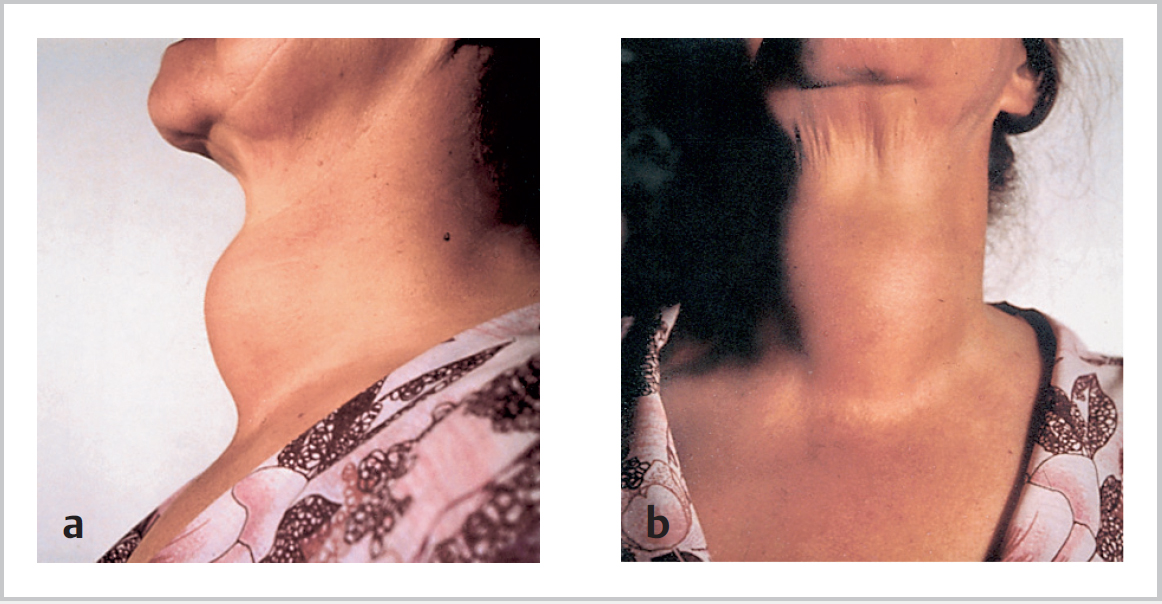
49.3 Simple Goitres (Fig. 49.1)
 Puberty
Puberty
 Pregnancy
Pregnancy
 oral contraceptive pill (OCP)
oral contraceptive pill (OCP)
 Radioactive iodine:
Radioactive iodine:
 Suppression therapy:
Suppression therapy:
 Antithyroid medication:
Antithyroid medication:
 May present with dyspnea, stridor that is positional/nocturnal, or coincidentally on chest X-ray with shadowing in upper mediastinum
May present with dyspnea, stridor that is positional/nocturnal, or coincidentally on chest X-ray with shadowing in upper mediastinum
 Investigations:
Investigations:
 Treatment:
Treatment:
49.3.1 Toxic Goitres
49.3.2 Clinical Features
 Most common
Most common
 One or more:
One or more:
 Autoimmune with thyroid antibodies
Autoimmune with thyroid antibodies
 15% family history
15% family history
 F>M 5:1; middle ages
F>M 5:1; middle ages
 Treatments:
Treatments:
49.3.3 Treatment
![]()
Stay updated, free articles. Join our Telegram channel
 Clinically:
Clinically:
Full access? Get Clinical Tree


