56 Benign Neck Disease • Pathophysiology • Types • Locations • Clinical features – 60% birth – 75% by 1 year – 90% by 2 years • Management • Characteristic features • Epidermoid cyst • True dermoid cyst • Teratoid cyst • Embryology • Presentation • Investigation • Treatment • Suspect if cyst hard or irregular • 4th decade in women, 6th decade in men • Local excision and thyroxine suppression • Adjuvant thyroidectomy and radioiodine may be needed • Embryology • Pathology – Dorsal—runs medial to conchal cartilage extending posteriorly to retroauricular scalp – Ventral—presents as sinus/cleft/fistula inferior to cartilaginous EAM • Clinical features – Middle/lower neck – Parotid – Pharynx – Posterior triangle
56.1 Congenital Neck Masses
56.1.1 Lymphangiomas
 Normally 2 jugular sacs, 2 posterior sciatic sacs, and 1 retroperitoneal sac develop endothelial outbuddings and extend centrifugally to form lymphatic system
Normally 2 jugular sacs, 2 posterior sciatic sacs, and 1 retroperitoneal sac develop endothelial outbuddings and extend centrifugally to form lymphatic system
 Endothelial fibrillar membranes sprout from walls of sacs, penetrate surrounding tissue, canalize it, and produce more cysts
Endothelial fibrillar membranes sprout from walls of sacs, penetrate surrounding tissue, canalize it, and produce more cysts
 Pressure of cysts forces tumour along lines of least resistance into planes or spaces between large muscles or vessels
Pressure of cysts forces tumour along lines of least resistance into planes or spaces between large muscles or vessels
 Simple—thin-walled capillary sized (40%)
Simple—thin-walled capillary sized (40%)
 Cavernous—dilated spaces (35%)
Cavernous—dilated spaces (35%)
 Cystic hygroma—various sizes (25%)
Cystic hygroma—various sizes (25%)
 Oral 35%
Oral 35%
 Cervical 50 to 75%
Cervical 50 to 75%
 Axillary 15%
Axillary 15%
 Equal sex distribution
Equal sex distribution
 No preponderance to one side
No preponderance to one side
 Age at presentation:
Age at presentation:
 Stridor with tracheal displacement
Stridor with tracheal displacement
 Brachial plexus compression with pain and hyperesthesia
Brachial plexus compression with pain and hyperesthesia
 Sudden increase in size due to haemorrhage may be fatal
Sudden increase in size due to haemorrhage may be fatal
 Cryotherapy and sclerosant injection met with limited success
Cryotherapy and sclerosant injection met with limited success
 Excision required
Excision required
 Preop CT to exclude mediastinal involvement
Preop CT to exclude mediastinal involvement
 Use nerve stimulator to avoid CNs VII, XI, and XII
Use nerve stimulator to avoid CNs VII, XI, and XII
 Excise excess skin
Excise excess skin
 Multiple excisions may be needed
Multiple excisions may be needed
 External approach for intraoral lesions
External approach for intraoral lesions
 Recurrence rate is 10 to 15%; cavernous type most likely to recur
Recurrence rate is 10 to 15%; cavernous type most likely to recur
56.1.2 Midline Dermoids
 Always midline in neck
Always midline in neck
 Equal sex distribution
Equal sex distribution
 Most common
Most common
 No adnexal structures
No adnexal structures
 Contains cheesy keratinous material
Contains cheesy keratinous material
 Contains skin appendages—hair follicles, etc.
Contains skin appendages—hair follicles, etc.
 Can be acquired through implantation of epidermis in a puncture wound
Can be acquired through implantation of epidermis in a puncture wound
 Most occur in the floor of mouth with ¼ involving neck
Most occur in the floor of mouth with ¼ involving neck
 Present as slow-growing lesions
Present as slow-growing lesions
 Management is surgical excision
Management is surgical excision
 Rare
Rare
 May be lined by respiratory epithelium
May be lined by respiratory epithelium
 Contains elements from ectoderm, endoderm, and mesoderm
Contains elements from ectoderm, endoderm, and mesoderm
56.1.3 Thyroglossal Cysts
 Thyroid arises from floor of primitive pharynx between 1st and 2nd pouches
Thyroid arises from floor of primitive pharynx between 1st and 2nd pouches
 Median thyroid anlage loses lumen at 5 weeks and breaks into fragments—lower end divides into 2 portions that become lobes
Median thyroid anlage loses lumen at 5 weeks and breaks into fragments—lower end divides into 2 portions that become lobes
 Stalk should atrophy at 6 weeks; if not, it becomes a duct
Stalk should atrophy at 6 weeks; if not, it becomes a duct
 Cysts form when epithelial cells cease to remain inactive
Cysts form when epithelial cells cease to remain inactive
 Duct runs through hyoid to foramen cecum
Duct runs through hyoid to foramen cecum
 Fistula results from inadequate treatment
Fistula results from inadequate treatment
 Equal sex distribution
Equal sex distribution
 Mean age 5 (range 4 months–70 years)
Mean age 5 (range 4 months–70 years)
 Midline (90%), lateral (left) 10%
Midline (90%), lateral (left) 10%
 3× more common than branchial cysts
3× more common than branchial cysts
 65% infrahyoid, 20% suprahyoid, 15% juxtahyoid
65% infrahyoid, 20% suprahyoid, 15% juxtahyoid
 Also described intralingual, suprasternal, and intralaryngeal
Also described intralingual, suprasternal, and intralaryngeal
 5% present with infection; 15% present with fistulas
5% present with infection; 15% present with fistulas
 Rare familial variants
Rare familial variants
 Usually painless and mobile, characteristically move on swallowing and tongue protrusion due to them lying deep to investing layer of deep cervical fascia and relation to hyoid, respectively
Usually painless and mobile, characteristically move on swallowing and tongue protrusion due to them lying deep to investing layer of deep cervical fascia and relation to hyoid, respectively
 May present acutely with increasing pain, neck swelling, dysphagia, dysphonia, airway obstruction, fistula, and fever
May present acutely with increasing pain, neck swelling, dysphagia, dysphonia, airway obstruction, fistula, and fever
 TFTs
TFTs
 Suprahyoid cysts—technetium scan ± MRI
Suprahyoid cysts—technetium scan ± MRI
 USS
USS
 Sistrunk procedure with removal of central core of hyoid; stay medial to lesser cornua to reduce risk of hypoglossal nerve damage
Sistrunk procedure with removal of central core of hyoid; stay medial to lesser cornua to reduce risk of hypoglossal nerve damage
 7 to 8% recur
7 to 8% recur
 Consider removal of core of central tongue musculature in recurrent cases
Consider removal of core of central tongue musculature in recurrent cases
56.1.4 Thyroglossal Duct Carcinoma
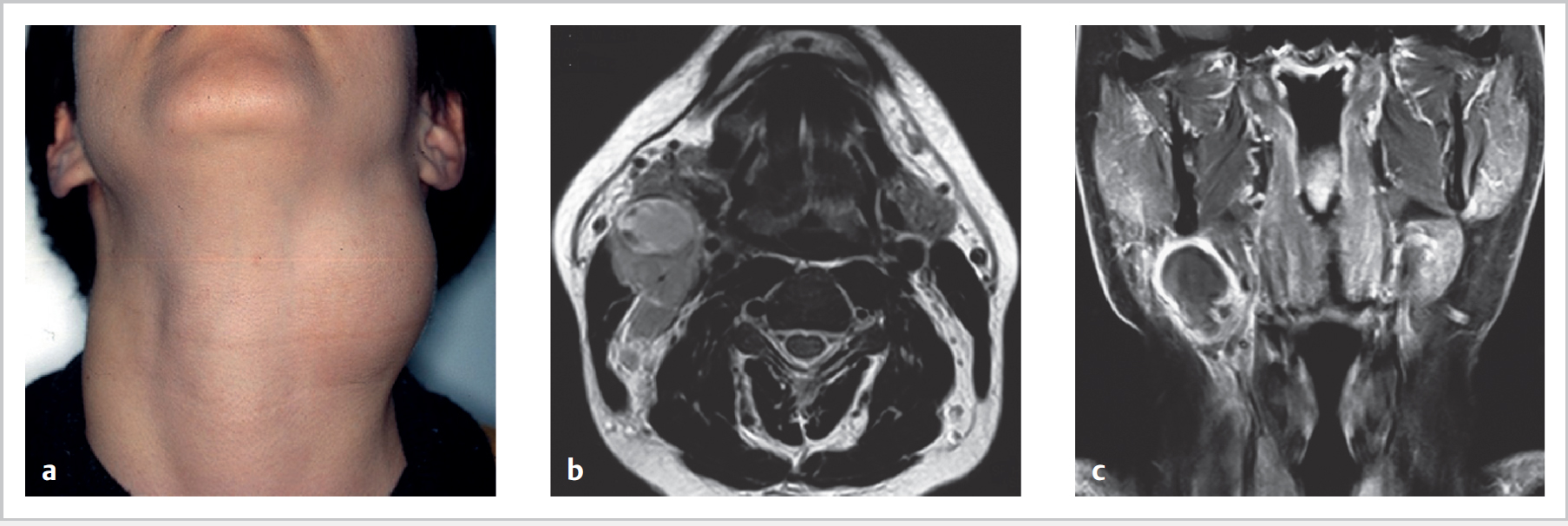
56.1.5 Branchial Cysts (Fig. 56.1)
 Remains of branchial clefts/pharyngeal pouches
Remains of branchial clefts/pharyngeal pouches
 Cervical sinus theory—remains of cervical sinus of His persist
Cervical sinus theory—remains of cervical sinus of His persist
 Thymopharyngeal duct theory—remnants of original connection between thymus and 3rd branchial pouch
Thymopharyngeal duct theory—remnants of original connection between thymus and 3rd branchial pouch
 Inclusion theory—epithelial inclusions in lymph nodes
Inclusion theory—epithelial inclusions in lymph nodes
 1st arch 5 to 25%
1st arch 5 to 25%
 2nd arch 40 to 90%
2nd arch 40 to 90%
 3rd/4th 2 to 8%
3rd/4th 2 to 8%
 Stratified squamous epithelium
Stratified squamous epithelium
 80% have lymphoid tissue in wall
80% have lymphoid tissue in wall
 2 types of 1st-arch anomalies:
2 types of 1st-arch anomalies:
 3 male:2 female
3 male:2 female
 Peak age 3rd decade (range 1–70 years)
Peak age 3rd decade (range 1–70 years)
 ⅔ on left
⅔ on left
 ⅔ anterior to upper ⅓ SCM
⅔ anterior to upper ⅓ SCM
 Other sites (⅓):
Other sites (⅓):
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


