Anatomy of the Trachea
The adult trachea measures approximately 12 cm but varies anywhere from 10 to 13 cm depending on height and sex. As there is some variability in the length, the anterior portion of the trachea is not subject to tremendous change, for the most part is composed of cartilage, and is C-shaped. The rings maybe complete or bifid. The posterior part of the trachea is also called the membranous portion and is the part of the airway that moves with breathing (Figure 37–1A).
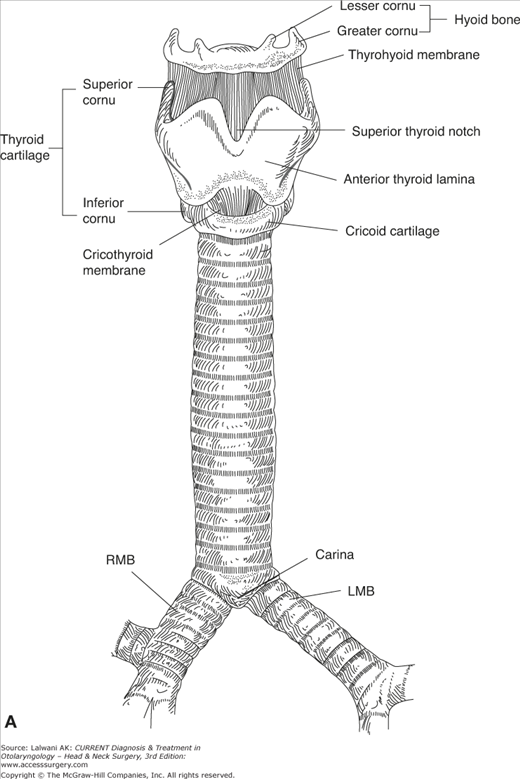
The diameter of the trachea varies among men and women. For the most part, the adult male tracheal diameter is 1.8–2.3 cm compared to the female airway, which is 1.4–2.0 cm. Each tracheal ring is about 4-mm high and there are approximately two rings per centimeter of trachea.
The cross section of the trachea may vary according to age or may be affected by an underlying disease process. For example, the juvenile trachea is more circular and more triangular in patients with chronic obstructive pulmonary disease.
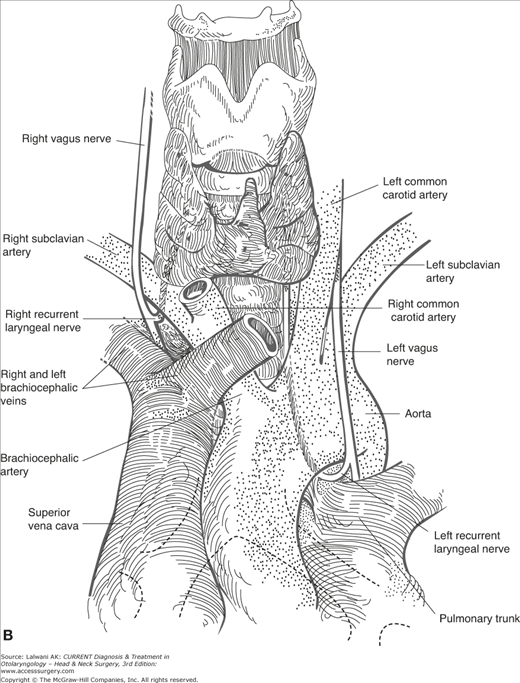
The trachea is positioned midline in the mediastinum and is surrounded by many vital structures. In the neck, the esophagus lies just left of the airway and then at the level of the clavicles is directly posterior and adherent to it down to the level of the carina (Figure 37–1B). This gives us a better understanding of why tracheoesophageal fistulas occur.
Anteriorly and laterally, the thyroid is situated in front of the trachea from the cricoid bone to the level of the 2nd to 3rd rings. The isthmus is at the midline and the lobes extend laterally onto the trachea. These two organs have common blood supply from the inferior thyroid artery.
The course of the recurrent nerves is very important for the tracheal surgeon. On the right, it comes off the vagus nerve and wraps around the subclavian and traverses superiorly to enter the larynx between the thyroid and cricoid cartilages in order to innervate the intrinsic muscles of the larynx. On the left it comes off the vagus beneath the aortic arch and runs in the tracheoesophageal groove.
In the compact space of the mediastinum, the trachea is also surrounded by the arteries and veins that come off the heart and the aortic arch. The innominate or bracheocephalic artery comes off the aortic arch and crosses the tracheal midline at and slightly below the level of the sternal notch. This is often the first blood vessel encountered during the pretracheal dissection during mobilization of the airway and also due to its proximity it is very important for the understanding of how certain complications like tracheoinnominate fistula arise. The carotids course the trachea and the thyroid laterally in the neck. The bracheocephalic vein runs in front of the innominate artery and well anterior to the pretracheal plane.
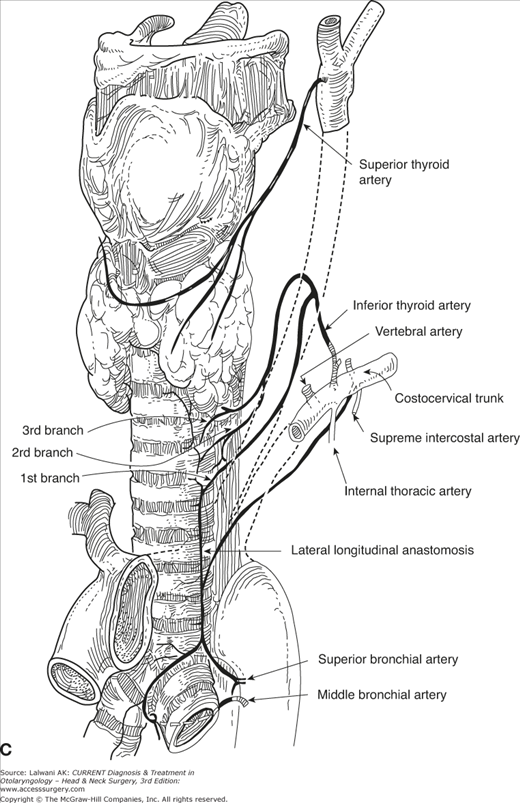
The blood supply of the trachea enters through its lateral pedicles. This is an important point with regard to tracheal resection in that dissection lateral to trachea can only be limited to 1–2 cm in order to prevent devascularization and anastomotic dehiscence (Figure 37–1C).
Upper half receives its blood supply from the inferior thyroid artery, which has three branches (first branch supplies the lower cervical trachea, second branch the middle section, and third branch the upper section).
Lower half and carina are supplied by the bronchial arteries (superior, middle, and inferior).
Superior bronchial artery comes off the right side of the aorta.
Middle bronchial artery connects with the superior bronchial to supply carina.
Inferior bronchial left bronchial tree.
The superior and middle bronchial arteries connect to the inferior thyroid artery through the lateral longitudinal anastomosis.
Tracheal Injuries
- History of trauma to head, neck, or chest
- Subcutaneous emphysema, pain, dyspnea, hemoptysis, cough, stridor
- Pneumomediastinum, pneumothorax despite chest tube drainage.
Although relatively rare, injuries to the trachea may arise in patients with penetrating or blunt force cervical trauma.
Blunt trauma. This is commonly caused by deceleration injuries at the laryngotracheal junction or at a branch point in the tracheobronchial tree—the two major points of tracheal fixation. Tearing or separation of the trachea can occur. This can also happen as a result of hyperextension of the neck or direct blow, often in the case of automobile accidents. Other than deceleration injuries, the trachea can also experience membranous wall ruptures or tears due to increased intratracheal pressure caused by compression of the chest wall.
Penetrating trauma. The extent of penetrating injuries to the trachea is determined by caliber and size of the weapon or projectile; although case-specific, bullet projectiles tend to result in more injury to adjacent tissues, such as blood vessels and/or the esophagus, as opposed to stab wounds.
First and foremost, establish a stable airway by intubation via fiberoptic bronchoscope. Bronchoscopy is the method of choice for detection and evaluation of any airway trauma. Computed topography (CT) scan can help identify manifestations of tracheal trauma such as pneumomediastinum, pneumothorax, and air within the tissue planes of the neck. Angiography can also be utilized to assess adjacent vasculature in the stable patient. Although varying opinions currently exist regarding intraoperative exploration of tracheal injury, the decision may be made to explore the neck or chest, particularly for inspection of the intrathoracic trachea, esophagus, and related vasculature based on penetration of the platysma for a neck wound and individual findings in the chest (ie, bronchopleural fistula with pneumothorax, hemothorax, or evidence of ongoing bleeding in the chest).
In stable patients with minor injuries, intubation, antibiotic treatment, and close observation may suffice. The endotracheal cuff should be placed below the injury to avoid mediastinal or subcutaneous air.
This depends on the location and severity of wound and associated injuries; however basic principles of tracheal surgery still apply. A low-collar incision provides almost complete exposure. The best approach to the distal trachea is through a right thoracotomy. This allows access to trachea, carina, right and left main bronchi, and intrathoracic esophagus. Simple lacerations may be repaired via debridement and repair with suture. More complex injuries may require circumferential tracheal resection and or reconstruction as well as end-to-end anastomosis.
Prognosis depends on the overall condition of the patient and other concurrent injuries.
Although relatively rare, iatrogenic tracheal injury can occur with prolonged endotracheal intubation. Complications include tracheoinnominate fistula, tracheoesophageal fistula, tracheomalacia, and various lesser injuries that, however infrequent, can be life-threatening and require immediate diagnosis and intervention.
- Prolonged intubation with cuff erosion into innominate artery
- Massive hemorrhage or hemoptysis
- Premonitory or “herald bleed.”
Tracheoinnominate fistula is a rare but often fatal complication of tracheal intubation. This is often the result of cuff over inflation or from a poorly positioned tracheostomy tube.
Direct bronchoscopy is the most effective diagnostic tool available, although the excessive bleeding is indicative of a likely arterial injury.
Proper technique in performing tracheostomies, as well as limited intubation time (>2 weeks), should be followed to avoid TIF injury. Placement of the tracheostomy between the second and third tracheal rings will dramatically reduce the likelihood of TIF injury. Avoidance of sharply angled, rigid tracheostomy tubes and appropriate alignment of the tube is critical as well.
The initial maneuver in managing this potentially fatal complication is to overinflate the tracheostomy cuff. In the majority of cases, this will control the bleeding and the patient can be moved to the operating room. In the event that cuff over inflation fails, manual compression of the artery against the sternum can also control bleeding after the trach is removed and the patient is intubated from above. In the operating room, flexible and rigid bronchoscopy, as well as a sternal saw, should be readily available. The authors recommend sternotomy for exposure with ligation of the artery above and below the fistula. The segment of damaged trachea is excised along with the damaged vessel and reconstructed with primary end to end anastomosis. Strap muscle should then be interposed between the airway and the artery (Figure 37–2).
Figure 37–2.
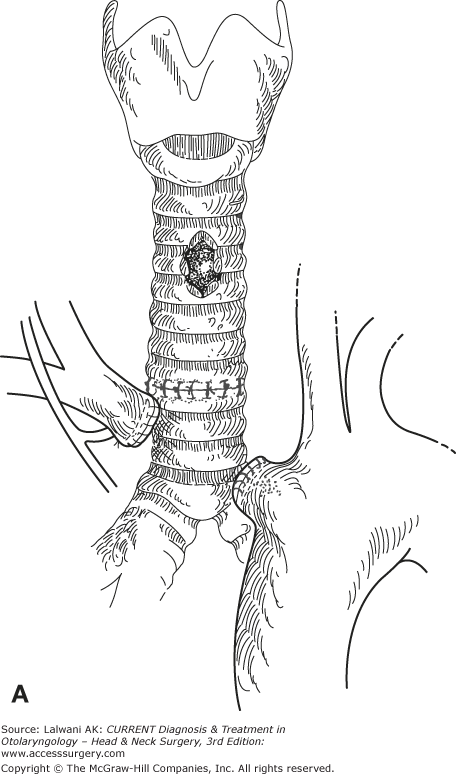
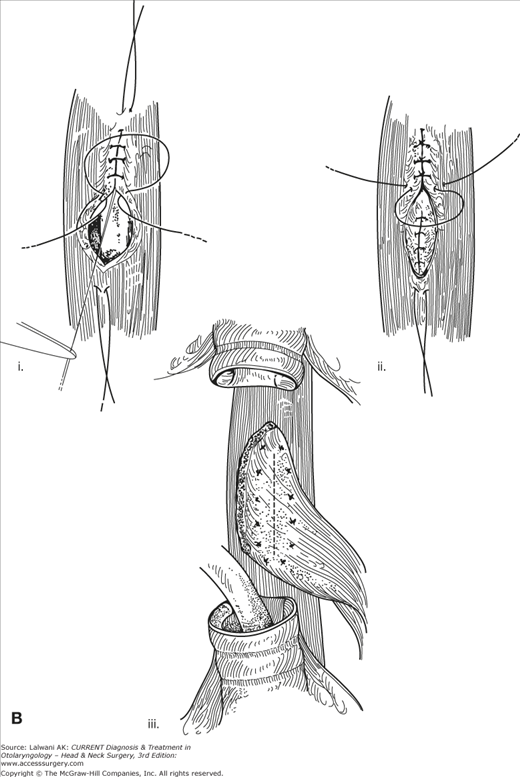
Surgical repair of tracheoinnominate fistula. (A) Resection of involved trachea and artery. (B) Tracheo-esophageal fistula repair with (i, ii)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


