Basics of Soft Contact Lens Fitting
Peter R. Kastl
Corey Dickson
David W. Lamberts
When one considers whether to fit a rigid contact lens or a soft contact lens on a particular patient, the main difference (as far as the patient is concerned) is comfort. A soft lens, by its very nature of being soft, is unlikely to cause corneal compression, corneal abrasions, or irritated eyelids. Soft lenses are larger than rigid lenses and have thin edges, so that the upper edge of the soft lens fits under the upper eyelid. On blinking the lid glides over the soft lens, rather than first “bumping over” the edge, the way a lid does with a rigid lens.
The eye adapts rapidly to soft lenses.1 Soft lenses are often well tolerated from the initial insertion, and most patients report that their soft lenses are comfortable within 30 minutes.
Other advantages of soft lenses include the following:
Lack of spectacle blur. This phenomenon is noted usually from rigid lenses, where corneal molding or edema produces visual blur upon removing the lenses and attempting to see with spectacles. Any corneal edema with soft lens wear tends to be diffuse; in addition, corneal molding is rare with soft lenses.1
Possibility of intermittent wear. Soft lenses may be worn sporadically for occasional social or athletic events. Unlike rigid lenses, corneal tolerance does not require wearing soft lenses every day.
Reduced incidence of lens decentration. Soft lenses are larger than rigid lenses and adhere more tightly to the cornea. Thus they are dislodged much less frequently.
Reduced incidence of overwear. Overwear of rigid lenses can lead to extreme pain. This phenomenon is much less likely to occur with soft lenses, and if it does occur, it is much less severe. Some soft lenses are designated as “extended wear,” and patients can sleep in them.
Lack of glare, photophobia, and flare. These symptoms are common problems during rigid lens adaptation but are rarely seen with soft lenses.
Easier to replace lenses from inventory relative to rigid lenses.
Disposable modality is available.
Soft lenses come in many colors and tints.
There are disadvantages to soft lens wear. These include the following:
Astigmatism is not corrected with standard lenses. Standard spherical soft lenses do not correct astigmatism as rigid lenses do. A patient who has astigmatism yet desires soft contact lenses has to be fit with toric soft lenses.
Vision can be variable. Depending on multiple factors such as dry eye, dry environment, and lens age, vision with soft contact lenses can vary from day to day or even during the course of a day.2
Fragility. Soft lenses are fragile and easily torn. Clumsy patients or those who otherwise “don’t have good hands” will find soft contact lenses difficult to wear.
Deposit formation. Because nearly all soft lenses have water content, deposit formation is more common than with rigid lenses.3 In addition, rigid lens deposits can be polished off the lens, whereas soft lens deposits may require replacing the lens.
CONTRAINDICATIONS TO SOFT CONTACT LENS WEAR
Because soft contact lenses are composed in part of water, they can harbor pathogens, toxins, and allergens. They can dry out. They can absorb various agents from the environment. Therefore, there are various contraindications, some absolute, some relative, of which the practitioner must be aware:
Monocular patient. One must balance the risk of soft lens wear against the improved vision. Is it worth the risk to a remaining eye simply to do away with the use of spectacles?
Low refractive error. Soft lens care requires continuous vigilance; is it worth it to fit a low myope?
Abnormal lid function. If the lids do not close properly or do not “wipe” the lens surface properly, then the lens will dry out or experience increased deposit formation.
Presence of a filtering bleb. Unless one fits an extremely large soft lens over a bleb, the edge of the lens can irritate the bleb, possibly causing it to fail or become infected.
Dusty environment. Airborne particles can attach themselves to a soft lens or get under it.
Dry eye. Hydration of a soft lens is dependent on availability of aqueous tear. Without enough tear, the lens will dry out and cause irritation or possibly become infected.7,8
Anesthetic cornea. If the patient cannot feel that there is a problem with a soft lens, then any complication will be magnified. Anesthetic corneas probably should not be fit with soft contact lenses.9
Blepharitis. Nearly all humans have blepharitis to some degree. The practitioner must decide whether a particular case is bad enough to warrant not fitting with soft lenses.10
Pregnancy. Corneas tend to steepen during pregnancy. The practitioner would be well-advised to defer soft lens fitting until after delivery.11,12
Spectacle prisms. Soft contact lenses cannot compensate for spectacle prisms.13
Large astigmatism. While specially made toric contact lenses may work with high astigmatism, such eyes probably are best fit with rigid lenses.14
Volatile chemicals. If a patient is chronically exposed to volatile chemicals, these may dissolve in soft contact lenses and cause ocular irritation.15 Such patients should be advised to remove their lenses before being exposed.
SPECIAL CONSIDERATION: ACCOMMODATION AND CONVERGENCE
When a myopic correction is moved from the spectacle plane to the corneal plane (and corrected for vertex distance), the eye must accommodate more. Young patients will notice nothing untoward. Prepresbyopic patients nearing the age of 40 will find themselves at a loss, however, and may require reading assistance (reading glasses) earlier than if they had remained in spectacles.
In addition, this increased accommodation will cause increased convergence, causing patients with convergence insufficiency to experience asthenopia when reading with their contact lenses.
For both of these phenomena, hyperopes experience the opposite: they enjoy less accommodative and convergence requirements.
CLASSIFICATION BY WATER CONTENT
The corneal epithelium receives its oxygen from the air, and soft contact lenses block that oxygen transmission, to a greater or lesser degree, depending on their water content. Atmospheric oxygen dissolves in the water of soft lenses and diffuses to the cornea. Thus, it is useful to classify soft contact lenses based on their water content:
Low: 37.5% to 46% water, used for daily wear only
Medium: 46% to 58% water, used for both daily and extended wear
High: 59% to 76%, used for extended wear
The new silicone-hydrogel soft lenses do not fit into this classification, as the silicone added to the polymer matrix vastly increases oxygen transmission, even though the water content is low. These lenses can be used for extended wear.
CLASSIFICATION BY WEARING TIME
It also is useful to classify soft contact lenses by the length of time they can be worn: daily wear, conventional extended wear (up to 7 days), continuous wear (up to 30 days), and 1-day disposable, which are discarded on a daily basis.
SAGITTAL DEPTH (SAGITTAL HEIGHT)
Sagittal depth or height is the distance that any contact lens “stands off” from a flat surface, as seen in Figure 55.1. The larger the sagittal depth, the tighter the lens. Conversely, the smaller the sagittal depth, the looser the lens. Sagittal depth is affected by diameter and base curve. Figure 55.2 shows the change in sagittal depth as the diameter of a contact lens changes. Figure 55.3 shows how sagittal depth changes with different base curves. By altering diameter and/or base curve, one can make a contact lens looser or tighter.16,17,18 Think of the sagittal depth effect as a “suction cup effect”: the deeper the suction cup, the tighter it is; the shallower the suction cup, the looser it is.
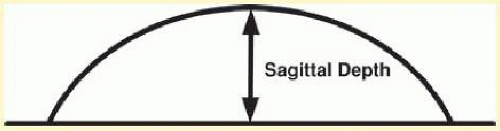 FIG. 55.1 Sagittal depth is demonstrated as the distance from the apex of the contact lens to the flat surface upon which it rests. |
SOFT CONTACT LENS FITTING
The following method assumes that the lens fitter has taken keratometry readings and has refracted the patient.
Lens Selection
The first step to fitting a soft lens is to choose the diameter. The horizontal visible iris diameter (HVID) should be measured and a diagnostic lens 0.5 to 2.0 mm larger should be chosen. The second step is to choose the base curve. One method of base curve selection is to choose the steeper lens for keratometry readings larger than 44.00 D; choose the flatter base curve for keratometry readings less than 44.00 D. Another method is to select a lens 3 to 5 D flatter than the flattest keratometry readings. It is important to make this adjustment because the large chord diameter of the soft lens will yield a tight fitting relationship if a base curve is selected to closely match the flat keratometry reading.
The third step is to refract over (“overrefraction”) the diagnostic lens.
Evaluation of Fit
When the patient looks up, the lens should lag by 1.0 mm. In addition, gentle pressure on the lower lid by the examiner’s index finger should cause the lens to move upward. Vision should be clear before and after blinking.
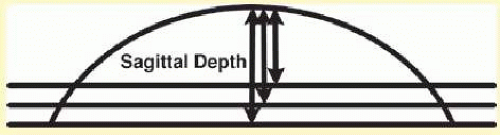 FIG. 55.2 As the diameter of a contact lens changes, so does the sagittal depth. |
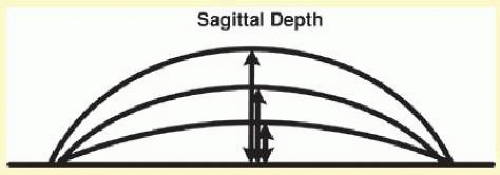 FIG. 55.3 As the base curve of a contact lens changes, so does the sagittal depth. |
If the lens is too loose, then it will have excessive movement, resulting in increased patient awareness, decentration, and variable vision. One can correct a loose lens by increasing the sagittal depth-use to a steeper base curve or a larger diameter lens. If the lens is too tight, there will be little or no movement, variable vision, decreased comfort over time, and a burning sensation upon removal. One can correct a tight lens by decreasing the sagittal depth-use to a flatter base curve or a smaller diameter lens.
It is important to remember that a soft lens should extend beyond the limbus, ideally 0.5 or more. Some patients will have stability of vision, good lens movement and lag, but complain of discomfort. If this occurs, one must rule out a rip or tear in the lens, and manufacturing defects. Another potential issue could be a lens that is too small with edges resting in the limbus. Patients will typically complain of increased lens awareness and will not tolerate the fit.
Follow-up examinations
One should examine a newly fit contact lens patient in the first several days after fitting, or at least no later than 1 week after fitting. There should be another examination at 1 month after fitting, and then annually.
SOFT TORIC LENS FITTING
Some patients will have moderate degrees of astigmatism (1 to 2 D) and will want optimal comfort. Soft toric lenses are the lenses of choice.19,20 In other cases, patients will have refractive astigmatism but have a spherical cornea; these patients have lenticular or residual astigmatism. Such patients can be fit with soft toric lenses.
These lenses are fit similarly to rigid front toric lenses, in that a special diagnostic lens is placed onto the eye and its rotation is observed. Soft toric lenses are held in position by either prism ballast or by truncation, where the inferior portion of the lens looks as if it were “chopped off.”
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


