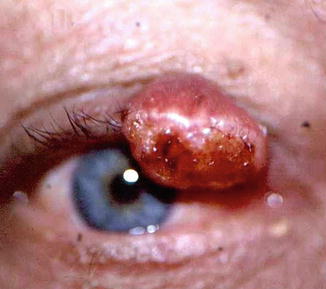
Fig. 4.1
Nodular BCC of the lower lid margin, presenting as an irregular, pearly dome-shaped tumor
4.6.2 Pigmented
The pigmented BCC is usually nodular or nodulo-ulcerative, ranging in color from light tan to deep brown.
4.6.3 Cystic
4.6.4 Infiltrating
The infiltrating BCC presents as an indurated, yellowish to tan patch or plaque with occasional focal ulceration and poorly defined margins (Fig. 4.3). Patchy crusts, papules, and nodules are scattered throughout some morpheaform tumors. Infiltration within the eyelid can cause deformities and malpositioning of the lid margin.

Fig. 4.3
Infiltrating BCC presenting as an indurated, yellowish to tan patch or plaque with focal ulceration and poorly defined margins
4.7 Histopathologic Features
BCC is characterized by a proliferation of cells with oval nuclei and scant cytoplasm that form infiltrative nests or strands (Fig. 4.4). The neoplastic cells are relatively uniform in appearance and seldom display significant anaplasia or mitotic figures. At the periphery of the nests, they are usually arranged in a radial pattern called “palisading” (Fig. 4.5): although this is not diagnostic, in its absence the diagnosis of BCC should be questioned. The nests of tumor cells characteristically retract from the stroma, creating a gap (Fig. 4.5). Initially thought to be a processing artifact, this gap reflects defects in the production of adhesion-like substances by tumor cells. Necrosis is a common finding in BCC, and the necrotic debris eventually calcifies or is replaced by fibrous scar tissue. BCC also demonstrates an inflammatory infiltrate of variable intensity around the nests of tumor cells that consists predominantly of lymphocytes. The junction between the stroma of the neoplasm and normal connective tissue is ill defined [1].
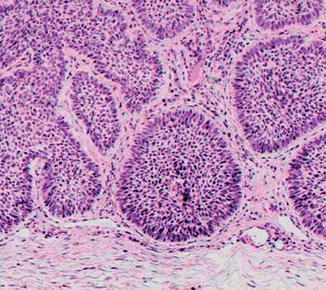
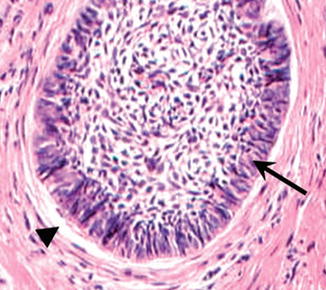
Fig. 4.4
Histopathologically, BCC is characterized by a proliferation of cells with oval nuclei and scant cytoplasm that form infiltrative nests or strands
Fig. 4.5
At the periphery of the nests, the tumor cells are usually arranged in a radial pattern called “palisading” (arrow), and these are characteristically retracted from the stroma, creating a gap (arrowhead)
There is no universally accepted histopathologic subclassification of BCC according to patterns of growth and cellular differentiation. The two most important growth patterns are the circumscribed and the infiltrative. Circumscribed BCC is characterized by nests and sheets of tumor cells and usually corresponds clinically to a nodular tumor. In contrast, an infiltrative BCC is composed mainly of elongated strands of tumor cells that are several cell layers thick, with no peripheral cellular palisading (Fig. 4.6), and usually corresponds to a morphemic variety. However, in many cases different growth patterns occur in the same tumor (Fig. 4.7). There is a third important histologic pattern, the superficial BCC, which is presumed to be of multicentric origin and with horizontal spread. Superficial BCC is described mainly on the trunk and extremities [1]. More than 20 types of cellular differentiation or histologic patterns have been described in BCC as signs of sebaceous, apocrine, or eccrine gland, as well as pillar differentiation in an otherwise typical BCC [1, 6]. However, only the metatypical (basosquamous) carcinomas have an impact on prognosis. Basosquamous carcinoma displays various degrees of squamous differentiation and has been suggested to occupy a conceptual intermediate ground between squamous cell carcinoma and BCC (Box 4.1) [1].
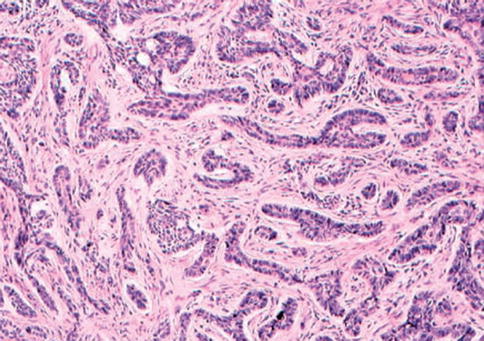
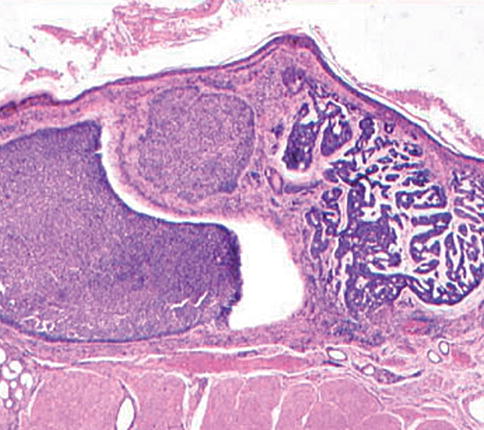
Fig. 4.6
An infiltrative BCC is composed mainly of elongated strands of tumor cells that are several cell layers thick, with no peripheral cellular palisading
Fig. 4.7
In many cases different growth patterns of BCC occur in the same tumor
Box 4.1: Salient Diagnostic Findings
Painless, firm, nodular, or flat skin lesion with smooth, pearly epithelium, and subepithelial telangiectatic vessels, accompanied by loss of adnexa
Microscopic findings of infiltrative nests, sheets, or strands of cells with oval nuclei and scant cytoplasm, which are arranged at the periphery of the nests in a radial “palisading” pattern
Presence of a gap between the nests of tumor cells and the stroma
4.8 Diagnostic Evaluation
4.8.1 Histopathologic Examination of Excisional or Incisional Biopsy
The most important diagnostic evaluation of BCC is histopathologic examination of the excised tissue. Incisional biopsy should be taken only in cases where the clinical diagnosis is highly questionable, otherwise excisional biopsy should be performed.
4.8.2 Exfoliative Cytology
Exfoliative cytology has been shown to have a high diagnostic accuracy for BCC but may be considered only occasionally, when the plan is to treat the tumor nonsurgically [7].
4.8.3 Imaging
When orbital or intraocular invasion is suspected, imaging is used to evaluate it. T1 contrast-enhanced fat-suppressed MRI scans are the modality of choice for demonstrating a soft tissue mass or infiltration. Computed tomographic (CT) bone windows with axial and coronal views of the orbit are best for demonstrating bony destruction – which, however, is uncommon in BCC patients [8].
4.8.4 Other Noninvasive Methods
Pulsed ultrasound at 20 MHz has been used for the noninvasive measurement of BCC thickness in order to plan photodynamic therapy (PDT) and to evaluate the rate of tumor regression after treatment. It was found that such measurements can distinguish between skin, fibrosis, and tumor and can even trace recurrences of BCC prior to clinical findings [9].
4.9 Differential Diagnosis
The clinical and histopathologic differential diagnosis is broad. Challenging examples are trichoepithelioma and desmoplastic trichoepithelioma, metastatic carcinoma, sebaceous carcinoma, squamous cell carcinoma, and keratoacanthoma. However, as BCC is by far the most common malignant lesion of the periocular skin, most periocular nodular or cystic skin lesions should be treated as suspicious.
4.10 Treatment
The main treatment modality for BCC is surgical excision of the lesion with microscopic monitoring of its margins or Mohs’ microsurgery [1, 10]. The other surgical and nonsurgical modalities include curettage and electrodessication, cryosurgery, radiotherapy, chemotherapy, photodynamic therapy, and immunotherapy. Selection of the appropriate therapy depends on the patient’s age, anticipated life expectancy, and the location, size, and pattern of growth characteristics of the tumor. However, therapies that are not surgical and do not include microscopic monitoring should be avoided for BCCs when they are not very small, when they are located in the medial canthus, or when the margins are clinically ill defined. The importance of preventing sun exposure needs to be stressed to children and young adults in order to reduce the incidence of BCC in the future [1].
4.10.1 Surgical Excision
Only by surgical excision of the tumor with safe margins it is possible to assess the adequacy of extirpation. However, in cases with deep infiltration into the orbit or in proximity to the eyeball tissues, excision with safe margins is not possible and exenteration is inevitable. A variety of ways are used to examine the surgical margins, and good results have been reported when frozen-section control is used. Mohs’ micrographic surgery has been considered to be the most reliable method for tumor extirpation or as reliable as excision with frozen-section or permanent-section control, with the lowest recurrence rate and best cure rate [1, 12, 13]. As significant extra difficulty, time, and expense of Mohs’ surgery may not be justified in all BCCs of the eyelid, and thus it is usually reserved for deeply infiltrative tumors with a high risk of recurrence [1]. An intermediate technique that incorporates Mohs’ surgery using formalin-fixed, paraffin-embedded sections (slow Mohs) may offer a histologically superior and cheaper alternative to standard Mohs’ surgery [14].
The carbon dioxide laser has a few advantages over the conventional scalpel in the excision of BCC, including the possibility of bloodless excision of tissue in thin layers for histological examination of the margins and the possibility of obviating electrocautery, which is important for patients taking anticoagulants or who have a cardiac pacemaker [1].
Special reconstructive techniques are used to maintain the functions of the eyelid and to achieve the best cosmetic results after surgical excision of periocular BCC (Chap. 10).
4.10.2 Curettage and Electrodesiccation
Curettage and electrodesiccation and, lately, vaporization of the tumor by CO2 laser are commonly used techniques to treat small BCC in areas remote from the eye. As the adequacy of margins is not determined, there is always the risk that residual tumor will escape destruction, especially near embryonic fusion planes. Also, the amount of secondary scarring and contracture with electrodesiccation may be cosmetically unacceptable in the periocular area [1].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


