Arterial Obstructive Disease of the Eye
George E. Sanborn
Larry E. Magargal
Arterial obstructive disease of the eye is frequently encountered in clinical practice. It usually occurs suddenly and presents dramatically but there is also a chronic form of presentation that is less frequently seen. In this chapter, we first discuss the acute presentations of arterial obstructive disease and then the chronic forms; usually, the chronic forms are due to some manifestation of carotid artery disease.
ACUTE ARTERIAL OBSTRUCTIVE DISEASE
CENTRAL RETINAL ARTERY OBSTRUCTION
Central retinal artery obstruction is one of the most sudden and dramatic events seen by ophthalmologists and was described as early as 1859.1 Although there have been numerous clinical and experimental studies of the pathophysiology of central retinal artery obstruction and although these studies have been augmented by the introduction of intravenous fluorescein angiography in the 1960s, the disease still has a relatively poor visual prognosis.
The clinical picture is typically striking. Patients present with a sudden painless loss of vision. The appearance of a cherry-red spot in the fundus is characteristic (Fig. 1).2 The cherry-red spot appears because soon after obstruction of the blood flow to the inner retina, the normally transparent retina becomes opaque and blocks the brownish-red color from the underlying choroid, which is still supplied by blood. Because the retina overlying the foveola is relatively thin, however, the normal color of the choroid is still visible in this area.3,4 Although characteristic, the cherry-red spot is not pathognomonic for central retina artery obstruction.5 Sometimes the characteristic cherry-red spot does not develop; there may be only a slight accentuation of the brownish-red color in the foveola.4 It is not known how long it takes this cherry-red spot to appear, but in a primate model, it has appeared as early as 30 minutes after obstruction.6 An afferent pupil defect is usually present.2
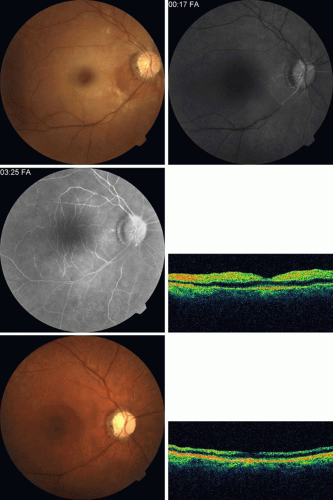 FIG. 1. A: Acute central retinal artery obstruction with a cherry-red spot. B and C: Intravenous fluorescein angiography. There is a delay of dye appearance in the central retinal artery, and when it does appear, it does not fill the arteries completely. D: Ocular coherence tomography (OCT) at the time of occlusion showing the increase in retinal thickness and reflectivity of the inner layers of the retina. E: Seven months later there is significant optic atrophy(G), and the OCT (F) shown now has marked thinning of the retina. |
With obstruction, virtually all eyes have narrowing and irregularity in the arteries and there is frequently an irregularity in the caliber of the retinal veins.2,4,6,7 Segmentation (boxcarring) of the blood column frequently develops; this segmentation is particularly noticeable in the veins and can be seen as a to-and-fro movement of the blood elements.3,4 Retinal hemorrhages, however, are not characteristic of central retinal artery obstruction.7
With time, the retinal opacity diminishes, generally leaving an optic nerve that is atrophic (Fig. 1). Frequently, thinned retinal arteries and veins also remain.7,8 No foveolar light reflex is evident, and a finely pigmented appearance of the macula is typical.7 In some cases, arterial collaterals develop at the optic disc.9,10,11 Rarely, anatomoses that exist between the central retinal artery and the ciliary arteries become visible as preretinal loops (Nettleship collaterals) after an occlusion at the edge of the disc.12,13,378 In approximately 20% of patients, an embolus is evident somewhere in the arterial system.14 Emboli are discussed later.
Intravenous fluorescein angiography is useful in showing the details of the abnormal circulation of a central retinal artery obstruction (Fig. 1). The principal abnormality is the delay in the appearance of the dye in the central retinal artery and its branches.2 Rather than the central retinal artery and its branches filling rapidly, considerable time may elapse before the entire arterial system is filled.15 The filling of the retinal arteries is often abnormal, with the fluorescein partially filling an artery (a dye front) or hugging the vessel wall, as in normal venous filling.15
Segmentation of the blood column is often well defined on fluorescein angiography.15 Venous filling is usually slowed and occasionally the dye does not progress beyond laminar flow during the study.14 In approximately 10% of eyes that have central retinal artery obstruction, there are abnormal choroidal filling defects, reflecting posterior circulation obstruction. These defects can occur even in patients who appear to have a typical central retinal artery obstruction.14 Leakage of dye from the vessel walls is not normally seen except at the site where an embolus lodges within a retinal artery.16 With time, the flow within the artery and its branches is reestablished and the appearance of the intravenous fluorescein angiogram may return to normal.
The electroretinogram (ERG) is usually abnormal in central retinal artery obstruction. The b-wave is reduced, indicating a marked abnormality in the circulation of the inner retina.17,18 The a-wave, indicating normal photoreceptor function, is preserved or accentuated. There does not appear to be a good correlation, however, between the extent of b-wave abnormality and the degree of retinal function,3 although Yotsukura and Adachi-Usami420 reported that the b-wave amplitude increased with visual improvement. The photopic negative response (PhNR) shows severe depression in this condition reflecting the significant loss of the ganglion cells and their axons.377 The electrooculogram may be either normal or abnormal. Visual field defects are usually profound but either occasionally a small portion of the temporal peripheral visual field remains or the patient has a large central scotoma.3 The onset of obstruction occurs most often between the hours of midnight and 6 AM, with the second most common period being between 6 AM and noon.2
Most patients with central retinal artery obstruction complain of a sudden loss of visual acuity in the affected eye; most of these patients present with visual acuity ranging from finger-counting to light perception.14 Only about 5% of patients have visual acuity of no light perception and most of these have involvement of the posterior ciliary circulation, which can be seen on either intravenous fluorescein angiography or electrophysiology.14 Without a partial central retinal artery obstruction or a spared cilioretinal artery (to be discussed), it is unlikely that any patient will have initial visual acuity better than finger-counting.14 With or without treatment, most eyes retain visual acuity of finger-counting to light perception. Patients with a spared cilioretinal artery do not seem to have a follow-up visual acuity that is significantly different from those without a spared cilioretinal artery.14
Central retinal artery obstruction is caused by the disruption or cessation of blood flow to the central retinal artery, its branches, and the retinal layers supplied by those vessels. The inner two thirds of the retina derives its blood supply from the central retinal artery and its branches; the outer third of the retina is supplied from the choroidal circulation.19,20,21 The central retinal artery and its branches function as an end artery, and with the exception of a few anastomotic connections between the retina and the ciliary circulation at the optic disc, there are no other anastomoses.19 No intrinsic retinal vessels are present in the fovea because the inner retinal layers are not present in this area.19
Histopathologically, when a central retinal artery obstruction occurs, the retina initially becomes edematous. With time, all the retinal layers supplied by the central retinal artery and the artery’s branches, including the nerve fiber layer, ganglion cells, inner plexiform layers, and the inner portion of the inner nuclear layer, are lost.20 In trypsin digest preparations after obstruction of the central retinal artery, the greatest change is in the capillary bed,22 where extensive ischemic changes take place. Usually, little attempt is made to repair the retina with gliosis or neovascularization.20 The most common site of obstruction of the central retinal artery is at the level of the lamina cribrosa.20
Clinically, it is possible to examine the blood flow velocity in the central retinal artery in a noninvasive manner, using a variety of techniques.21 The most useful appears to be color Doppler imaging, providing simultaneous Doppler and B-scan ultrasound images of the optic nerve head, which primarily represents flow in the central retinal artery.23 Studies using this technique demonstrate a marked reduction of or no blood flow in the central retinal artery with an acute central retinal artery occlusion that returns to normal with time.24
Characteristics of the retinal blood flow can be measured clinically with retinal Doppler velocimetry.385 This is an instrument that can measure the blood column diameter, the centerline blood velocity, and the blood flow in major retinal vessels. However, when evaluating the blood flow in the optic nerve, choroidal, and retina, the Doppler laser flowmetry is more sensitive to the blood flow in the superficial layers than in the deeper layers.410
Masaoka and colleagues384 studied the hemodynamic changes in the retinal circulation with a scanning laser ophthalmoscope and intravenous fluorescein angiography. This technique allows the assessment of erythrocyte velocities and movement with high resolution continuous images and is a useful technique for the evaluation of hemodynamic changes in vascular occlusions.
Analysis of the retinal nerve fiber layer by one of the confocal laser scanning tomography techniques can provide information about a central retinal artery occlusion. Foroozan and co-workers383 studied patients with a central retinal artery occlusion within 1 week of occlusion with a scanning laser polarimeter. Diffuse attenuation of the retardation of the nerve fiber layer surrounding the optic nerve was seen in all eyes studied. Four patients were scanned in follow-up at intervals ranging from 1 week to 6 weeks; all had unchanged studies.383
Optic coherence tomography (OCT) of an acute central retinal artery occlusion shows a slight increase in the thickening of the retina and reflectivity of the inner layers of the retina that correspond to the opacity seen clinically (Fig. 1).409 With time, the disc becomes atrophic and the retina thinner.
Experimental studies of central retinal artery obstruction in the cat25 and the rhesus monkey26,27,28 have increased our understanding of arterial obstruction. The most clinically relevant finding is that there is a period in which a total lack of blood flow (ischemia) to the inner retina can be tolerated; that is, if the blood flow is not obstructed longer than this period, visual function may return to normal. This critical time in the cat eye is 90 minutes,25 and in the young, healthy rhesus monkey it is 100 minutes26,27,28—any longer than this and the histologic changes are irreversible and the animal has permanent visual loss. Hayreh and co-workers379,380 have repeated this experiment to determine how long the retina can survive central retinal artery occlusion in middle-aged and elderly rhesus monkeys, a situation that might be more applicable to the human situation where most occlusions occur in older patients. That study showed that an occlusion of less than approximately 100 minutes produced no permanent damage and that an occlusion of longer than 240 minutes produced massive and irreversible retinal damage. It is not known why the older monkeys had a longer retinal survival time with occlusion of the central retinal artery than younger monkeys.
Because there is no evidence that the monkey and the human have different retinas,379 the studies by Hayreh and co-workers have implications for studies that attempt to treat central retinal artery occlusion. Any treatment of this condition will almost certainly have to be initiated within 100 to 240 minutes, assuming the occlusion is total, or the patient will likely have permanent damage to the retina, regardless of treatment.
On average, central retinal artery obstruction occurs in patients who are in the fifth or sixth decades of life, with the age range varying from 17 to 84 years. Fewer than 10% of patients are younger than 30 years of age.14,29,30
In some cases, the cause of central retinal artery obstruction is relatively clear, such as when due to a visible embolus. In other cases, however, especially when found in association with a systemic disorder such as diabetes, the association is less clear. Table 1 lists some of the conditions associated with central retinal artery occlusion. Arteriosclerosis is probably the most commonly associated systemic condition. With the progressive buildup of subendothelial atheromatous material, the lumen of the central retinal artery becomes narrowed over time and eventually may become occluded.20 This association is inferred because most patients with central retinal artery obstruction are in the fifth to sixth decades of life, when atherosclerotic changes are expected.
Table 1. Conditions Associated With Retinal Arterial Obstructions | ||||
|---|---|---|---|---|
|
The next most common systemic condition associated with central retinal artery obstruction is arterial hypertension; it can be found in as many as two thirds of all patients with central retinal artery obstruction.14,30,31 Carotid artery disease has been found in about 45% of patients who have central retinal artery obstruction,30 and hemodynamically significant stenosis occurs in approximately 20%.32 O’Farrell and Fitzgerald33 found ipsilateral carotid artery disease in 88% of patients presenting with retinal ischemia but neither study defined retinal ischemia nor indicated the ages or method of selection for patients studied. No difference was demonstrated between stenosis in the ipsilateral and the contralateral carotid artery33; this suggests that the cause of retinal artery occlusions may not be carotid artery stenosis—it may be simply associated with these occlusions or whatever process causes the carotid artery disease. Merchut and co-workers34 found no relation between the types of arterial occlusion—branch or central—and the type of underlying carotid artery disease. Wijman and colleagues35 found a high-grade internal carotid stenosis of 70% or more in 73% of patients with retinal ischemia that included transient ischemic attacks (TIAs) and arterial occlusions, both acute and chronic.
Diabetes mellitus14,28 and valvular heart disease28 are probably the next two most common associated conditions.
A variety of hematology parameters have been associated with central retinal artery occlusive disease.291,292,293 Walsh and co-workers291 found significant elevation of platelet coagulant activities (associated with the early stages of intrinsic coagulation) were elevated in patients with a central or branch retinal artery occlusion compared to controls. Kiesewetter and co-workers292 studied blood parameters in six patients with a central retinal artery occlusion before treatment was instituted. They found that compared to controls, the plasma viscosity, the extent of erythrocyte aggregation, and the plasma fibrinogen was significantly increased, while the erythrocyte deformation was reduced.
Sagripanti and associates389 found elevation of the prothrombin fragment (F1+2), the formation of thrombin-antithrombin III complex, and D-dimer (a stable degradation product of cross-linked fibrin) in acute central and branch retinal artery occlusions compared to controls. On follow-up examinations, the elevated F1+2 and the thrombin-antithrombin III complex significantly decreased while the D-dimer did not. The investigators conclude that increased thrombin generation may have a role in artery occlusions. However, the patients studied were treated with intravenous heparin and methylprednisolone, and the manuscript does not indicate whether their blood samples were taken prior to treatment or whether treatment could have affected the studies performed.
Greiner and co-workers388 studied 13 patients with a central retinal artery occlusion and 7 patients with a branch retinal vein occlusion for deficiencies in the protein C pathway. They concluded that the incidence of protein C deficiency in the artery occlusions they studied was not statistically significant from their control group.
Two research groups have shown a higher plasma level of homocyst(e)ine in patients with a central retinal artery occlusion, but not branch retinal artery occlusion.390,391 Wenzler and co-workers392 found hyperhomocyst(e)inemia in 2 patients: 1 patient with a central retinal artery occlusion in one eye and a branch retinal artery occlusion in the opposite eye, and 1 patient with bilateral branch retinal artery occlusions. However, the studies in the literature in regard to plasma homocyst(e)ine do not provide an answer as to whether elevated plasma homocyst(e)ine levels are an independent risk factor for retinal artery occlusive disease or are related to other vascular risk factors. Hyperhomocyst(e)inemia is an independent risk factor for atherosclerosis and atherothrombosis.416
The difference in the etiology of central retinal artery obstruction depends on the age of patients presenting with an obstruction. Central retinal artery obstruction in patients 30 years of age or younger tends to be associated with migraine, coagulant disorders, intraocular abnormalities, and trauma.29 Systemic diseases such as systemic arterial hypertension, atherosclerotic disease, and diabetes mellitus are not found in this younger age group.28,29 Some patients in the younger age group do not have a known cause for the obstruction; this was the case in as many as 12% of patients in one large series29 and in 40% of patients in a smaller series.30
Greven and associates31 studied 27 eyes in 21 patients with a retinal artery occlusion; all patients were younger than 40 years of age; emboli were identified in only 7 patients (33%) who had cardiac valvular disease, the most common cause in 4 patients (19%). The authors were able to identify various associated factors leading to a hypercoagulable state or embolic condition in 19 patients (91%).31 Despite their findings, the authors believe that the percentage of patients with ophthalmoscopically visible emboli is not indicative of the percentage of patients whose etiology for obstruction is embolic, and that most central retinal artery occlusions are embolic in origin.36
Two hundred fifty-six consecutive patients with acute unilateral retinal artery obstruction were studied using carotid Doppler ultrasonography; 18.8% had more than 60% stenosis of the internal carotid artery.37 Of those who had significant carotid stenosis, only 19 (40%) had visible retinal emboli. Thus, if ultrasound testing had been based only on visible retinal emboli, almost 60% of significant carotid artery stenotic lesions would have been missed.37 All patients at risk for extracranial carotid artery disease with acute retinal artery occlusion—not only those with visible emboli—should undergo duplex carotid Doppler ultrasonography.37
Evaluation of a patient with an arterial obstruction should be tailored somewhat to the age of the patient. A patient 20 years of age likely does not have extra-cranial carotid artery disease, whereas a 70-year-old patient clearly should be evaluated for such disease. Likewise, a 70-year-old patient with central retinal artery obstruction may have temporal arteritis, whereas this diagnosis in a 30-year-old patient is not likely.
There is probably little value, however, in determining the type of emboli if one is observed in the fundus. Sharma and co-workers38 found poor intraobserver and interobserver agreement on the quantitative assessment of retinal emboli when assessing them into groups of cholesterol, calcific, or both. Sharma and co-workers386 performed a retrospective multicenter chart review of 104 patients with both embolic and nonembolic acute retinal artery occlusion on whom transthoracic echocardiography was performed to determine the accuracy of visible retina emboli as a diagnostic test for anticoagulation or cardiac surgery. In this study, 41 patients had visible retinal emboli. The presence of a visible embolus in this review had no effect on whether a patient received anticoagulation or cardiac surgery, based on transthoracic echocardiography.
In some patients, the source of emboli from the heart can be determined with transthoracic echocardiography.39,40,412 When transthoracic echocardiography does not demonstrate the source of emboli, transesophageal echocardiography may be of more diagnostic value.41,42,43,381,412 Kramer and co-workers381,382 studied 18 patients with a retinal artery occlusion with transthoracic and transesophageal echocardiography. Seven of these patients had a central retinal artery occlusion. Sixty-one percent of the patients studied had at least one cardiac or aortic source of emboli detected by transesophageal echocardiography that was missed by transthoracic echocardiography. The authors recommend performing transthoracic echocardiography first, and then if the findings suggest cardiac or aortic conditions, performing the study via the esophagus: these findings include mitral valve disease, other valvular calcifications, enlargement of the left atrium, and severe left ventricular dysfunction.386
For all patients with a central retinal artery occlusion, the authors recommend an evaluation by a primary care physician or internist, to rule out systemic disease, and suggest as part of the evaluation, a Doppler study of the extracranial carotid arteries as well as a transthoracic echocardiogram. For patients with a visible embolus who have a negative carotid Doppler and normal transthoracic echocardiogram the authors generally suggest a transesophageal echocardiogram (depending on the patient’s age as this is an invasive procedure). In older patients (however that is defined) with a central retinal artery occlusion we obtain a Westergren sedimentation rate and C-reactive protein to help eliminate the possibility that a patient may have temporal arteritis. Because elevated homocyst(e)ine has been associated with this disease and is an independent risk factor for atherosclerosis,416 the authors recommend testing the plasma homocyst(e)ine. Bilateral simultaneous central retinal artery occlusions413 are extremely rare and should prompt a careful search for a cause.
Thew authors’ approach is more aggressive with younger patients. If a careful physical examination and search for emboli (including transesophageal echocardiography) are unrevealing and no obvious systemic cause exists for the obstruction, it may be useful to screen for hemotologic abnormalities; the most common finding is protein S deficiency.44,45 Whether this abnormality is responsible for or simply associated with retinal occlusions is unknown.
Treatment of either central retinal artery obstruction or branch retinal artery obstruction is unsatisfactory. No method has been proved to be more effective than the natural course of the disease.393,394 Although anecdotal cases abound of dramatic improvement in vision after some therapeutic intervention, no evidence is available that such intervention changes the natural course of the disease. The authors have seen one patient who presented on two different occasions with typical central retinal artery obstruction and severely decreased vision, who regained normal vision with no therapeutic intervention. Other clinicians have seen similar spontaneous recovery.399
The theoretical goal of treatment is to restore the retinal blood flow as soon as possible. Lowering intraocular pressure is one of the principal methods of treatment because the pressure load may perfuse the retina or dislodge an embolus.6,47 Paracentesis may be the fastest way to accomplish this.48,49 There is no documented evidence, however, that it is possible to improve arterial circulation with paracentesis or that paracentesis dislodges emboli in humans. Experimental studies in animals failed to show that paracentesis results in a significant increase in retinal perfusion.50,51,52 At least one case has been reported of endophthalmitis after paracentesis for central retinal artery obstruction.53 Reduction of intraocular pressure can also be accomplished with intravenous acetazolamide47 or topical glaucoma medications. Some investigators advocate continuation of acetazolamide for up to 2 weeks.54
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


