Antiparasitic Drugs in Ophthalmology
Kirk R. Wilhelmus
Antiparasitic drugs arose from research on the treatment of malaria. Work on azo dyes and mould extracts was further stimulated by other parasitic diseases affecting the military during World War II.1 A recent incentive was the control of parasites affecting farm animals and pets.
Toxoplasmosis was the first ocular parasitic disease for which antimicrobial control was experimentally and clinically evaluated. The need for other drugs became apparent as protozoal and helminthic diseases of the eye were increasingly recognized.2 Several agents are now available for the major parasitic diseases of the eye (Table 66.1).3 Many are considered investigational or “off label” for treating ocular disease.4 Specially formulated solutions are feasible for corneal and external infections. Guidelines for preparing ophthalmic pharmaceuticals and for adding preservatives to extemporaneous eye drops should be followed.5
TABLE 66.1. Major Parasitic Infections of the Eye | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Antiprotozoals for Acanthamoebiasis
Acanthamoeba exists in two forms, double-walled cysts and motile trophozoites. Amebic cysts are more refractory to elimination than trophozoites.6 No single antiamebic agent is uniformly amebicidal and able to penetrate into the infected cornea without toxicity.7,8 The role of many compounds, including plant extracts,9 antiseptics,10 and antineoplastics11 remains speculative. Cumulative clinical experience has led to multidrug regimens for Acanthamoeba keratitis (Table 66.2).12,13,14
TABLE 66.2. Antiprotozoal Drugs for Acanthamebic Keratitis | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Aminoglycosides: Neomycin and Paromomycin
Historical Development
The term antibiotic was first defined in 1945 to describe chemical substances of microbial origin that inhibit the growth or metabolism of micro-organisms. Streptomycin was discovered by screening soil actinomycetes, for which Waksman received the 1952 Nobel Prize. In 1949, one strain (Streptomyces fradiae) was found to produce a group of antibacterial compounds collectively called neomycin.15
Neomycin-containing products are composed largely of neomycin B. Oral neomycin is poorly absorbed and was formerly used to suppress intestinal flora before bowel surgery. Ototoxic and renal side effects limit neomycin’s use to topical dermatologic and ophthalmologic preparations.16 Neomycin has amebicidal and cysticidal activity17 and was used to treat some of the first reported cases of Acanthamoeba keratitis.18,19
Paromomycin (“closely resembling neomycin”) was isolated from Streptomyces rimosus20 and S. chrestomyceticus. This oral aminoglycoside was first used in the treatment of intestinal amebiasis and tapeworm infestation and more recently for cryptosporidiosis. Paromomycin (called “aminosidine” in the United Kingdom) inhibits Acanthamoeba21 and is possibly more active than neomycin.22 Paromomycin 1% solution was used in the first patient treated for Acanthamoeba keratitis.23 The amebicidal role of other aminoglycosides has not been explored.
Chemistry and Preparations
Neomycin is a highly polar cation that is very stable at room temperature. Neomycin B contains three amino sugars linked to an aminocyclitol ring (Fig. 66.1). Neomycin sulfate is available in several ophthalmic eyedrops and ointments, often in combination with other antibiotics and/or corticosteroids. Neomycin-containing eyedrops are commercially available in concentrations of 1.75 mg/mL with polymyxin B and gramicidin (Neosporin and others), 3.5 mg/mL with polymyxin B (Statrol), 3.5 mg/mL with polymyxin B and a corticosteroid (Cortisporin, Maxitrol, Poly-Pred, and others), and 3.5 mg/mL with a corticosteroid (NeoDecadron). The solid drug (available as 500 mg tablets) or a concentrated solution (available in ampules for urinary bladder irrigation at a concentration of 40 mg/mL in combination with polymyxin B) can be diluted in buffered saline or artificial tears to a concentration of 5 to 10 mg/mL for topical use.
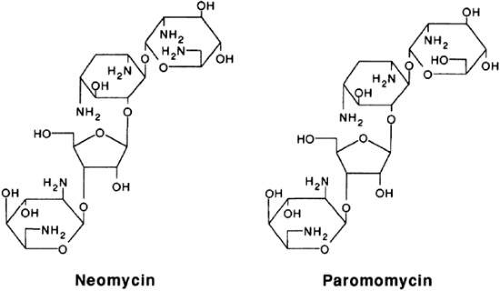 Figure 66.1. Aminoglycosides with antiprotozoal activity. |
Paromomycin I is made up of three amino sugars attached by a glycosidic linkage to a hexose nucleus (Fig. 66.1). The drug is water-soluble, and a topical preparation can be prepared by dissolving the powder of the 250-mg oral capsule (Humatin) in isotonic saline or artificial tears to yield a concentration of 10 mg/mL.
Pharmacologic Actions
Aminoglycosides exert antibacterial effects by binding to ribosomes, thereby inhibiting protein synthesis, and perhaps by a direct action on the cell membrane. The mechanism of action against Acanthamoeba has not been adequately studied. Neomycin and paromomycin have good amebicidal activity against trophozoites but limited cysticidal effects (Table 66.3).
TABLE 66.3. Susceptibility of Most Acanthamoeba Corneal Isolates | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Neomycin passes through the cytoplasmic membrane of trophozoites, probably by an active aerobic process. Amebicidal and cysticidal concentrations are typically much higher than corresponding minimal inhibitory concentrations.24 By itself, neomycin has a limited effect against cysts. The addition of an agent that disrupts the cyst wall may facilitate a cysticidal or cystistatic effect of neomycin.
Paromomycin interferes with ribosomal protein synthesis in several microorganisms, but its action on Acanthamoeba is not clear. Cysticidal activity may be related to an effect on membrane permeability.
Dosage and Pharmacokinetics
Aminoglycosides are applied topically for treating acanthamebic keratitis. One drop every 1 to 2 hours is usually begun during initial therapy. Corneal levels achieved by topical neomycin or paromomycin during inflammation have not been measured.
Adverse Effects
Topical neomycin produces contact hypersensitivity in 5% to 10% of patients. Eyelid edema, conjunctivitis, and punctate corneal erosions may be due to allergic and toxic effects of topical neomycin. Although the corneal epithelium is minimally affected by low doses of topical neomycin,25,26,27 cytotoxicity occurs at concentrations >5 mg/mL.28 Corneal sensation can be dampened by high levels of neomycin eyedrops.29
The effect of topical paromomycin on the ocular surface has not been adequately studied. Frequent dosing and prolonged administration may contribute to conjunctival hyperemia, punctate corneal erosions, and slow wound healing.
Clinical Experience
Neomycin or paromomycin has been a part of the medical regimen in several cases of Acanthamoeba keratitis,30,31,32 but it is difficult to ascertain their clinical value. Permanent quiescence has occurred with combination therapy that includes one of these topical aminoglycosides, but other cases have progressed. The role of neomycin and other antibacterial agents in eradicating or preventing concomitant bacterial coinfection that might complicate Acanthamoeba keratitis has not been determined.
Diamidines: Propamidine and Hexamidine
Historical Development
Diamidines were discovered after trypanosomes were observed to move and to multiply when glucose levels were high. Hypoglycemic drugs were then studied for antiparasitic activity, but researchers soon realized that trypanosomicidal activity of these guanidine compounds did not rely on their glucose-lowering effect. Other diamidines were then synthesized and screened.33 The finding that hydroxystilbamidine was effective in vitro against strains of Acanthamoeba led to the idea that other diamidine congeners might be clinically useful.
Pentamidine (pent[ane] + amidine) was developed in the 1930s. Propamidine (prop[ane] + amidine) was synthesized in 1941 and reported to have antimicrobial properties in 1951. Pentamidine, propamidine, and hexamidine (hex[ane] + amidine) were later found to have antiamebic properties.34 The addition of propamidine or hexamidine to the medical regimen for Acanthamoeba keratitis seemed to increase the likelihood of successful treatment.35,36,37,38
Chemistry and Preparations
Propamidine (4,4′-[trimethylenedioxy] dibenzamidine) and hexamidine (4,4′-[hexamethylenedioxy]-dibenzamidine) are available as di-isethionate salts in 0.1% ophthalmic solutions that are licensed as ocular disinfectants for nonprescription sale as Brolene (Rhône-Poulenc) in the United Kingdom and as Désomédine (Chauvin) in France, respectively (Fig. 66.2). Dibromopropamidine ointment (Brolene) is also marketed for human and veterinary use. Pentamidine (1,5-di[4-amidinophenoxy]pentane) is available as an isethionate salt (Pentacarinat, Pentam 300).
 Figure 66.2. Diamidines with antiamebic activity include propamidine (n = 3), pentamidine (n = 5), and hexamidine (n = 6). |
Pharmacologic Actions
Protonated amidine groups interact with the plasma membrane of trophozoites, resulting in cytoplasmic leakage. In vitro studies show variable cysticidal activity.39,40 Amebicidal and cysticidal effects partially depend on the lipophilic property of the drug, but the molecule must pass through the cyst’s double wall of hydrophilic chitin.
Diamidines produce an inhibitory effect upon gaining entry into the cell, where the drug blocks molecular linkages and dissociates nucleic acids from proteins. Diamidines bind to DNA sequences composed of at least four consecutive adenine-thymidine base pairs, although the relationship between nucleotide binding and amebicidal activity is uncertain.41 Aromatic diamidines also inhibit amebic adenosylmethionine decarboxylase42 and RNA polymerase43 and interfere with polyamine and glucose metabolism.44
Dosage and Pharmacokinetics
Adverse Effects
Topical diamidines can produce stinging and burning immediately after application. Conjunctival hyperemia and punctate corneal erosions have been attributed to its use.47 Mast-cell degranulation with histamine release can be triggered by propamidine. Systemic sensitization is rare, but contact hypersensitivity and urticaria have been described.
Clinical Experience
Single-drug therapy may be inadequate,48 so a multidrug regimen is commonly used in the treatment of Acanthamoeba keratitis.49,50 The use of a diamidine such as propamidine can lead to successful resolution of infection,40 but in vitro susceptibility does not necessarily predict clinical efficacy and outcome.51,52 Resistant cases have been encountered,53 and propamidine resistance can emerge during therapy.54
Biguanides: Polyhexanide and Chlorhexidine
Historical Development
Biguanides were first synthesized in the 1940s in the search for antimalarial agents. Chlorguanide and other guanidine derivatives (e.g., guanethidine) have minimal or inconsistent antiamebic activity, but their discovery led to biguanide compounds with broader antimicrobial properties.
Chlorhexidine was developed in the 1950s.55 When the bis-biguanides, such as chlorhexidine, were found to be more microbicidal than monomeric biguanides, polymeric biguanides were synthesized. Polyhexamethylene biguanide (polyhexanide, PHMB) was formulated during the 1960s in several molecular weights. Both compounds were developed as broad-spectrum biocides.
As a result of public concern about amebic meningoencephalitis, especially in Australia and New Zealand during the 1970s, an agent was sought to kill free-living amebae in swimming pools and hot tubs. PHMB was found to be amebicidal,56 and this cationic agent was developed for water sanitation. The proposal that biguanide biocides might play a role in the treatment of Acanthamoeba keratitis was based on in vitro studies at Bath, England. Choosing an empiric concentration of 0.02% (200 μg/mL) that would be expected to give corneal levels greater than the minimum cysticidal concentration, this diluted swimming pool disinfectant was first successfully used to treat patients responding poorly to conventional antiamebic therapy.57 Further experience confirmed its role in primary treatment.58,59
Chlorhexidine was shown to have in vitro efficacy against pathogenic amebae in the 1970s.60 Further laboratory testing corroborated that PHMB, chlorhexidine, and other biguanides (e.g., alexidine) were effective against Acanthamoeba.61 Biguanides emerged as clinically useful agents for treating Acanthamoeba keratitis during the 1990s.
Chemistry and Preparations
Polyhexamethylene biguanide is not commercially marketed as a human medication but is available in a number of nontherapeutic products under different trade names (Baquacil, Cosmocil, Vantocil). These heterodisperse mixtures contain differing average molecular weights of PHMB. The optimal antiamebic concentration for ocular use has not been determined. Some contact lens chemical disinfectants contain polymeric derivatives similar to PHMB but can vary in their inhibitory effects against trophozoites and cysts62,63,64,65,66,67,68,69,69a and in their epithelial cytotoxicity.69b
Serial dilution of a swimming pool disinfectant containing 20% Baquacil to a final concentration of 0.02% has been successfully used for Acanthamoeba keratitis. Concentrations of more than 0.5% are toxic to the ocular surface. Commercial preparations of PHMB may be composed of a mixture of various lengths of polymer chains (Fig. 66.3). Although several hundred repeating sequences are feasible, most products contain polymers of 5 to 15 hexamethylene units. The degree of polymerization may relate to microbicidal activity,70 and there may be therapeutic differences between Baquacil, Cosmocil, and other polyhexanide preparations.
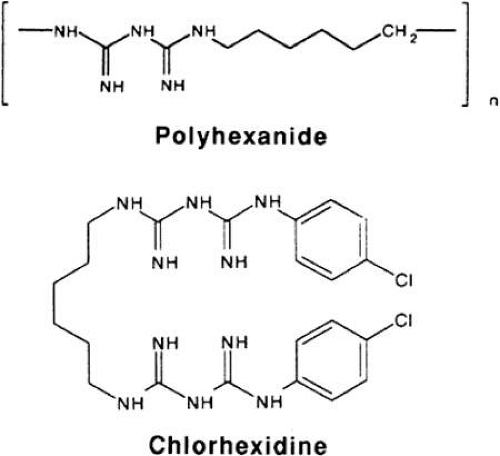 Figure 66.3. Biguanides with antiamebic activity. The number of repeating units (n) in commercial sources of polyhexanide (polyhexamethylene biguanide) ranges from 2 to 40. |
Chlorhexidine (1,6-di]4-chlorophenyl-diguanidino]hexane) digluconate is marketed as a skin disinfectant (Hibitane) in a detergent or alcohol base (e.g., Hibiclens and Hibistat) and for use as a mucosal rinse (e.g., Peridex).71 A concentration of 0.02% purified chlorhexidine in isotonic saline or artificial tears has been successfully used in treating Acanthamoeba keratitis.72
Pharmacologic Actions
Polyhexanide and chlorhexidine are taken up by amebic cysts and trophozoites.73 Cysts are more resistant than trophozoites,74 and encystation may account for the apparent development of resistance during therapy.75 Antiprotozoal effects depend on the concentration and duration of these biocides.76
Cationic biguanides adsorb to phospholipids of the trophozoite plasma membrane, leading to blebbing and cytoplasmic leakage.77,78 Biguanides also alter the permeability of amebic cysts. Polyhexanide results in shrinkage of intracystic amebae with separation of the plasma membrane from the endocystic wall,79 while chlorhexidine induces cyst swelling. By affecting the integrity of the cyst’s ostiole, biguanides might enhance the penetration of other antiparasitic agents.
Biguanides also deform cytoplasmic organelles, cause nuclear chromatin to aggregate, and disrupt protozoal DNA function by complexing with intracellular phosphated molecules such as adenosine triphosphate and nucleic acids. Several methods are available to assess the lethal effects of biguanides in the laboratory,80 but in vitro susceptibility may not predict the clinical effectiveness of biguanide therapy.81 Whether resistance can be induced experimentally or by selective environmental exposure has not been determined. Biguanide resistance may be due to reduced uptake.
Dosage and Pharmacokinetics
A 0.02% concentration of polyhexanide or chlorhexidine is typically used at a frequency of every 1 to 2 hours during initial treatment. The safety of a higher concentration is not clear.81a Corneal pharmacokinetics follows a two-compartment system, and corneal levels are achievable that are higher than the minimum trophozoiticidal concentration.81b These compounds increase the corneal penetration of other substances, presumably by affecting epithelial integrity.82 Biguanides can bind to plastic, glass, and chloride anions in saline, but the clinical importance of these interactions has not been determined.
Adverse Effects
Dilute preparations <0.05% are safe for ocular application, although stinging or burning may be noticed immediately after instillation. Conjunctival injection and punctate corneal epithelial erosions can occur. Low concentrations of polyhexanide83 or chlorhexidine84,85 have minimal epithelial toxicity, but high concentrations cause toxic keratoconjunctivitis.86,87 Stromal ulceration has occurred with chlorhexidine.88 Cataract and iris atrophy have developed during therapy.89,89a
Clinical Experience
Some patients respond to a single agent,90 but others fail monotherapy.91 Because biguanides and diamidines may be additive or synergistic,91a a biguanide is usually used in combination with another topical drug such as propamidine or hexamidine.92,93 The addition of a topical biguanide for patients unresponsive to other agents has led to clinical improvement.94 The use of both biguanides together has not been adequately assessed, and the role of other antiseptic biocides (e.g., povidone-iodine) is unclear.10,95
Azoles: Clotrimazole, Miconazole, Ketoconazole, and Itraconazole
Historical Development
Azoles were synthesized in the 1960s. Thiabendazole was found to have in vitro antifungal activity in 1965, and this discovery led to the development of other imidazoles. The first compound studied for human fungal infections was clotrimazole.96 In vitro studies subsequently showed that clotrimazole and miconazole were effective agents against Acanthamoeba.97,98 Clotrimazole and ketoconazole were used in some of the first reported cases of Acanthamoeba keratitis.23,99 Since then, imidazoles such as clotrimazole, miconazole, and ketoconazole or triazoles such as itraconazole, fluconazole, and voriconazole have been used as adjunctive agents in the treatment of Acanthamoeba keratitis. The role of metronidazole and related azoles is unclear.100,101 Other antifungals, such as natamycin and caspofungin, may have antiamoebic activity.7,101a
Chemistry and Preparations
Several imidazole and triazole compounds are commercially available (Fig. 66.4). Clotrimazole is available in dermatologic (Lotrimin and others) and vaginal (Mycelex and others) preparations, but these are irritating to the ocular surface. Topical clotrimazole 1% can be prepared by making a suspension in artificial tears,102 formulated from the micronized powder used for antifungal sensitivity testing. The suspension should be shaken before each use and may need to be reformulated every few weeks. Ophthalmic application of dermatologic azole creams can lead to a marked burning sensation.
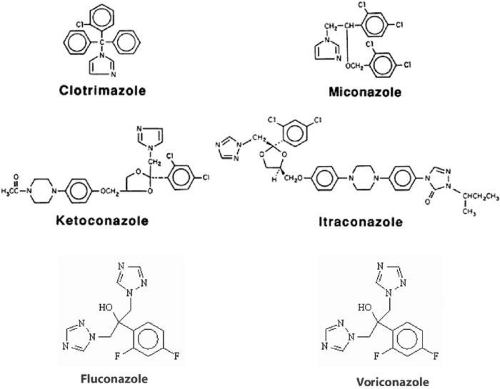 Figure 66.4. Azole antiparasitic agents. |
A topical preparation can be made by grinding tablets and suspending the powder in buffered solution to yield a 1% or 2% concentration, although most azoles are poorly soluble in water at neutral pH. Intravenous preparations of miconazole and voriconazole, available as either a solution containing parabens or as a powder, have been dispensed in 1% or 2% dilutions in eyedropper bottles for topical use.
Several azole compounds are marketed for oral use. Ketoconazole is available as 200-mg scored tablets. Itraconazole is available as 100-mg capsules. Voriconazole is available in 50-mg and 200-mg tablets and as an oral suspension.
Pharmacologic Actions
Azoles disrupt permeability of the fungal cell membrane. Their mechanism of action on amebic trophozoites and cysts has not been adequately studied but presumably results in leakage of cytoplasmic molecules by interacting with the hydrophobic portion of the phospholipid cell membrane. Azoles inhibit trophozoites,102a but cysts are more resistant.
Dosage and Pharmacokinetics
Oral absorption depends on gastric acidity, and bioavailability is reduced by antacids and H2-blockers such as ranitidine (Zantac) and famotidine (Pepcid). Absorption in patients with achlorhydria can be enhanced by swallowing the drug with an acidic cola or juice. The usual dose of ketoconazole is 400 mg daily, given as one or two doses. The oral drug is metabolized by the liver. By competing for hepatic microsomal enzymes, ketoconazole can increase the toxicity of other drugs, such as the nephrotoxicity of cyclosporine and the anticoagulant effect of warfarin. Oral ketoconazole results in a corneal level of approximately 50 μg/g that persists for at least a day.103
The usual adult oral regimen of itraconazole is 200 mg daily, taken as one or two doses, and of voriconazole is 200 mg twice daily. Absorption of itraconazole is greater when taken with food. Hepatic metabolism of the triazoles is slower than that of the imidazoles. Adequate levels are achieved in the aqueous humor after oral administration.103a
Topical ophthalmic preparations of imidazoles are not commercially available but can be made with an appropriate diluent. Oil and cyclodextrin vehicles have been used to prepare these compounds,104 although the lipid solubility of many azole compounds limits their corneal penetration. Combined oral and topical administration gives higher levels in the aqueous humor than topical alone.104a
Adverse Effects
Nausea is the most common side effect of ketoconazole and itraconazole after oral dosing and can be reduced by taking tablets with meals. Itching and skin rash can occur. Inhibition of steroid biosynthesis can result in menstrual irregularities, male gynecomastia, and fluid retention. Drug-induced hepatitis is rare, but patients with anorexia, malaise, nausea, or abdominal pain should probably have liver function testing. Ketoconazole is generally avoided in pregnant or nursing women. Compared with ketoconazole, systemic triazoles have less effect on human sterol metabolism.
Oral antihistamines such as astemizole (Hismanal) are avoided because of the risk of cardiac dysrhythmia. The dosages of digoxin and oral hypoglycemic agents may need to be adjusted. Cholesterol-lowering statins (e.g., lovastatin) may need to be discontinued during itraconazole therapy to avoid rhabdomyolysis.
Topical dermatologic and vaginal preparations of clotrimazole or miconazole may be too irritating for ophthalmic use. A 1% formulation of clotrimazole, miconazole, ketoconazole, or itraconazole produces minimal epithelial toxicity.105,106 Topical preparations can precipitate on the eyelid margins and within a corneal epithelial defect.
Clinical Experience
Topical clotrimazole107 and topical miconazole108,109,110 have been successfully used in combination with other agents. Adverse effects on the ocular surface limit their use in some patients. The benefit of an oral azole in medical treatment is difficult to assess. Some ophthalmologists use an oral agent, taken with meals, as a supplement during the first few weeks of topical treatment with other agents.111
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


