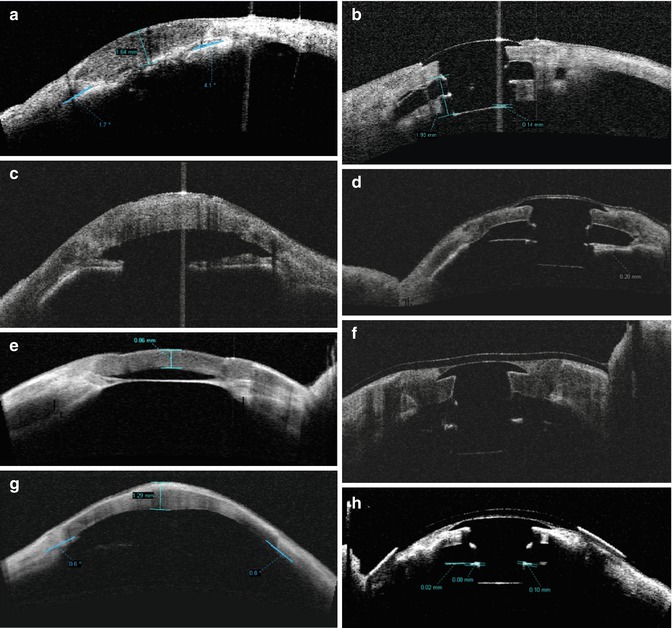
Fig. 4.1
Anterior segment OCT images. (a) Preoperative exam of a phakic eye [anterior chamber depth (ACD) = 2.71 mm; angle opening = 20°] with leukoma and corneal thickening. (b) Postoperative OCT of an aphakic Boston Type 1 KPro implanted after lensectomy. (c) Preoperative exam of an aphakic eye with a central corneal thickness of 1.080 μm
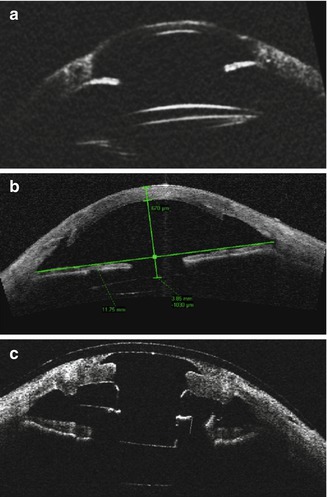
Fig. 4.2
(a) Anterior segment ultrasound (UBM) image of a pseudophakic eye with peripheral anterior synechiae. (b) Anterior segment OCT of a pseudophakic eye with corneal opacity after penetrating and endothelial keratoplasty. (c) Anterior segment OCT of a Boston Type 1 KPro implanted in a pseudophakic eye. The pseudophakic intraocular lens is noted as a linear hyper-reflective line located parallel and posterior to the posterior surface of the KPro optic
4.2.2 Functional Anterior Chamber Depth and Selection of Keratoprosthesis Model
Although the anterior chamber depth is measured from the iris plane to the inner surface of the cornea, the functional anterior chamber depth is smaller and measured from the iris plane to the keratoprosthesis back plate [3]. This is an important distinction because the functional anterior chamber depth must be taken into account when considering a secondary procedure such as implantation of an anterior chamber glaucoma drainage device. A narrow functional anterior chamber depth increases the risk of contact between the keratoprosthesis back plate and any other anterior chamber hardware, such as a drainage tube or intraocular lens. This can in turn lead to chronic inflammation and even cystoid macular edema [3]. In pseudophakic eyes that nonetheless have a shallow functional anterior chamber depth, removal of the intraocular lens with implantation of an aphakic model keratoprosthesis may be considered.
Preoperative axial length measurement is also a critical component of preoperative biometry, because the aphakic model of the Boston Type I KPro is available in different dioptric powers. The appropriate dioptric power is selected to match the axial length of a given aphakic eye [2]. The pseudophakic Boston KPro model comes in a single-standard dioptric power based on the assumption that the pseudophakic eye is approximately emmetropic [2].
4.2.3 Glaucoma Drainage Implants
Figure 4.3 shows an eye with a previously implanted glaucoma drainage implant (GDI) in the anterior chamber. In an eye with a narrow preoperative anterior chamber depth with a preexisting anterior chamber GDI, there is a high risk of contact between the tube and keratoprosthesis postoperatively [3]. In these cases, it may be prudent to reposition the tube either by placing it in the ciliary sulcus or by performing a pars plana vitrectomy with tube placement in the pars plana. Tube placement in the ciliary sulcus or pars plana is also a good option in planned combined keratoprosthesis/GDI procedures in eyes with a high risk of developing glaucoma [4]. Figure 4.4 shows an eye with a GDI and shallow preoperative anterior chamber depth, followed by keratoprosthesis implantation, vitrectomy, and repositioning of the tube into the pars plana.
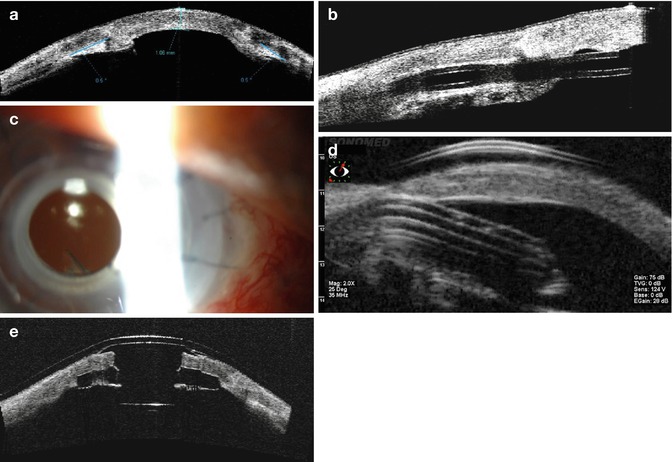
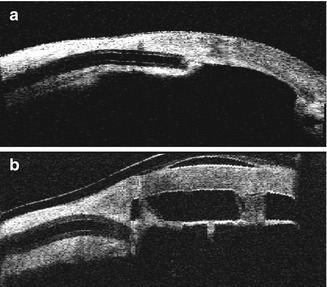
Fig. 4.3
(a) Preoperative anterior segment OCT of a patient with multiple prior corneal transplants (note anterior synechiae) and a previously placed glaucoma drainage implant (b). OCT aided in determining the position of the tube according to the meridian and its proximity to the endothelium. (c) Slit lamp photo of the same patient (note inferior placement of tube). (d) UBM demonstrating the glaucoma drainage implant in relation to the edematous cornea. (e) Anterior segment OCT after Boston Type 1 KPro implantation
Fig. 4.4
(a) Preoperative anterior segment OCT of an eye with corneal opacity and anterior chamber tube. The anterior chamber is extremely shallow with angle closure and apposition of the iris and cornea. The tube orifice is occluded by the iris. (b) Postoperative OCT of the same patient after keratoprosthesis implantation, pars plana vitrectomy, and repositioning of the tube into the pars plana
4.2.4 Other Synechial Changes of the Anterior Chamber
Other pathologic conditions that are important to identify preoperatively include synechial angle closure and iris-cornea touch (Fig. 4.5), which may necessitate intraoperative synechiolysis or concurrent glaucoma drainage device implantation.