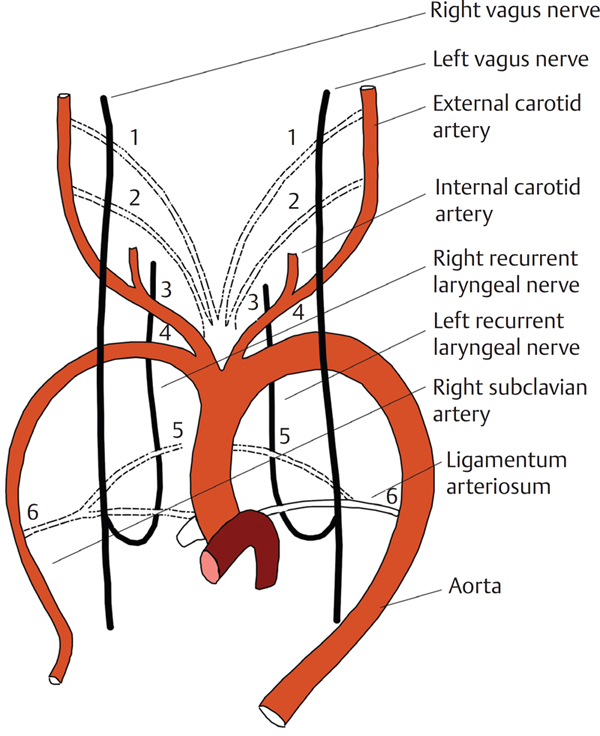
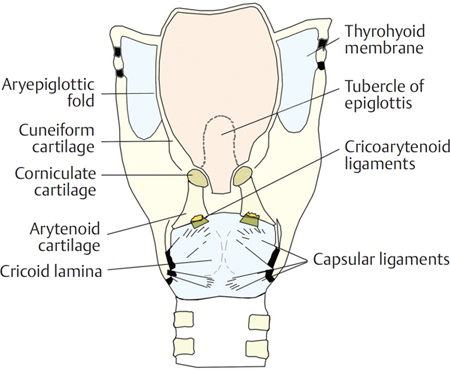
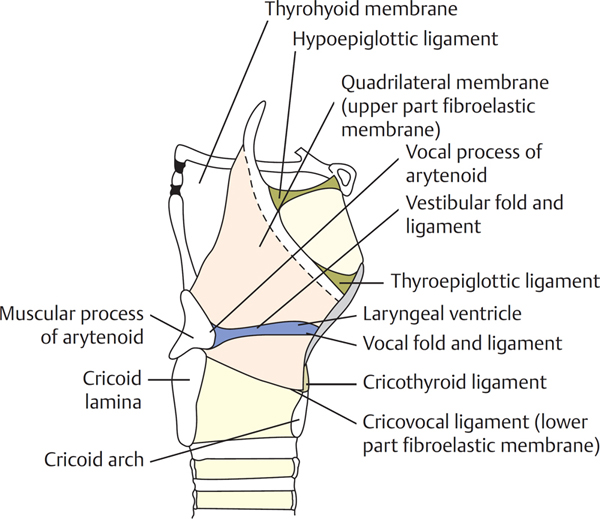
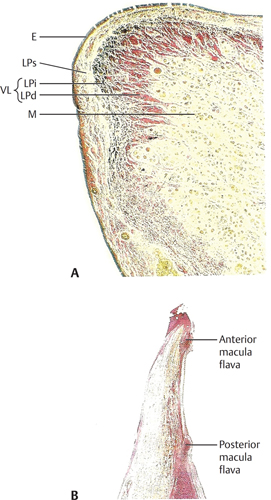
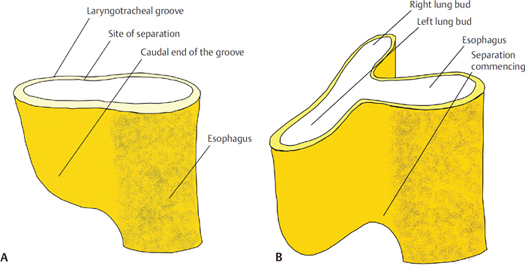
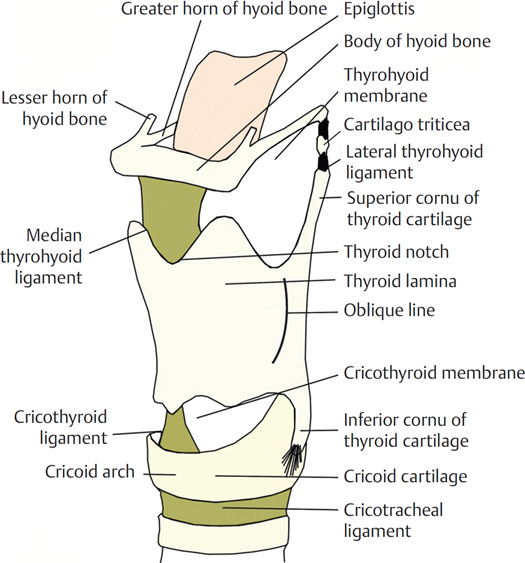
2 Anatomy of the Larynx By the end of the 17th century, knowledge of the gross anatomy of the larynx was complete. The remaining detail of the nerve supply and structure of the epithelial lining emerged during the 18th and early 19th centuries well before the discovery of the laryngoscope by Manuel Garcia in 1854.1 During the 4th week of embryonic development, the rudiment of the respiratory tree appears as a median laryngotracheal groove in the ventral wall of the pharynx (Fig. 2.1A, B). The groove subsequently deepens, and its edges fuse to form a septum, thus converting the groove into a splanchnopleuric laryngotracheal tube. This process of fusion commences caudally and extends cranially but does not involve the cranial end where the edges remain separate, bounding a slit-like aperture through which the tube opens into the pharynx. The tube is lined with endoderm from which the epithelial lining of the respiratory tract is developed. The cranial end of the tube forms the larynx and the trachea, and the caudal end produces two lateral outgrowths from which the bronchi and right and left lung buds develop. These grow into the pleural coelomas and are thus covered with splanchnic mesenchyme from which the connective tissue, cartilage and nonstriated muscles, and the vasculature of the bronchi and lungs are developed. The primitive larynx is the cranial end of the laryngotracheal groove, bounded vertically by the caudal part of the hypobranchial eminence and laterally by the ventral folds of the sixth branchial arches. The arytenoid swellings appear on both sides of the groove, and as they enlarge they become approximated to each other and to the caudal part of the hypobranchial eminence from which the epiglottis develops. The opening into the laryngeal cavity is at first a vertical slit or cleft, which becomes T-shaped with the appearance of the arytenoids. However, the epithelial walls of the cleft soon adhere to each other, and the aperture of the larynx is thus occluded until the 3rd month when its lumen is restored. The arytenoid swellings grow upward and deepen to produce the primitive aryepiglottic folds. This, in turn, produces a further aperture above the level of the primitive aperture that itself becomes the glottis. During the 2nd month of fetal life, the arytenoid swellings differentiate into the arytenoid and corniculate cartilages (derivatives of the sixth arch), and the folds joining them to the epiglottis become the aryepiglottic folds in which the cuneiform cartilages are developed as derivatives of the epiglottis. The thyroid cartilage develops from the ventral ends of the cartilages of the fourth branchial arch, appearing as two lateral plates, each with two chondrification centers. The cricoid cartilage and cartilages of the trachea develop from the sixth branchial arch during the 6th week. The trachea increases rapidly in length from the 5th week onward. Figure 2.1 (A) The closure of the laryngotracheal groove and (B) its separation from the esophagus in the latter part of the 4th week. The branchial nerves of the fourth and sixth arches, namely the superior laryngeal and recurrent laryngeal nerves, supply the larynx (Fig. 2.2). Each visceral arch is traversed by an artery (aortic arch). Each aortic arch connects the ventral and dorsal aortae of its own visceral arch. The primitive recurrent laryngeal nerve enters the sixth visceral arch, on each side, caudal to the sixth aortic arch. On the left side, the arch retains its position as the ductus arteriosus and the nerve is found caudal to the ligamentum arteriosum after birth. On the right side, the dorsal part of the sixth aortic arch and the whole of the fifth arch disappear. The nerve is, therefore, found on the caudal aspect of the fourth aortic arch, which becomes the subclavian artery. Piersol2 described the “complete persistence of the distal portion of the right aortic arch associated with the disappearance of its proximal part.” Here, the right subclavian artery originates from the descending aorta and passes right behind the esophagus. In the absence of the proximal portion of the right fourth aortic arch, no structure remains in contact with the right recurrent nerve. Instead of being pulled down into its usual position, the nerve passes directly from the main vagal trunk to enter the larynx.3 In this context, the nerve is called the nonrecurrent laryngeal nerve. The incidence is variously reported to be between 0.3 and 1.0%. For a left nonrecurrent nerve to exist, there would have to be either a loss of the ductus arteriosus in fetal life or a right-sided aorta. A case of the latter situation was reported by Berlin.4 Figure 2.2 The branchial arteries and recurrent laryngeal nerves. For further reading on the development of the trachea and lungs, consult O’Rahilly and Boyden5 and Reid.6 The prime reason for the existence of the larynx is not to make phonation possible, but to provide a protective sphincter at the inlet of the air passages. This can be seen in a lung fish, where the larynx takes the form of a simple muscular sphincter surrounding the opening of the air passage in the floor of the pharynx. In birds, the rima glottidis in the floor of the mouth shuts to close the air inlet, but it makes no sound; phonation is produced from a dilatation, the syrinx, at the lower end of the trachea just above its bifurcation. The first breathers of air, the amphibia, do, however, phonate. They achieve this by “swallowing air” that, as there is no separate nasal cavity, is drawn in through valvular “nostrils” that open anteriorly into the roof of the mouth. In mammals, a nasal cavity develops with the appearance of a palate. The separation of a respiratory and olfactory chamber from the mouth has considerable advantages: predatory mammals can still breathe while the mouth is obstructed by prey, and herbivorous prey can still sense warning odors while feeding. In aquatic vertebrates, such as crocodiles, dolphins, and whales, an intranarial larynx has been developed where the inlet of the larynx is suspended within the nasopharynx and clasped by the sphincter of the nasopharyngeal inlet (the palatopharyngeus). Thus, respiration and olfaction can continue at the water surface even with the mouth submerged, open, and ready for prey. The larynx of humans is still an essential sphincter, preventing the entry of swallowed food and other foreign bodies and providing a blockade to build up pressure for coughing or for aiding extreme muscular efforts. However, humans differ from other mammals in the ability to produce speech by the highest integrations of the nervous and locomotive systems. The larynx is situated at the upper end of the trachea; it lies opposite the third to sixth cervical vertebrae in men, while being somewhat higher in women and children. The average length, transverse diameter, and anteroposterior diameter are 44, 43, and 36 mm, respectively, in men and 36, 41, and 26 mm, respectively, in women. There is little difference in the size of the larynx in boys and girls until after puberty when the anteroposterior diameter in men almost doubles. The skeletal framework of the larynx (Figs. 2.3 and 2.4) is formed of cartilages, which are connected by ligaments and membranes and are moved in relation to one another by both intrinsic and extrinsic muscles. It is lined with mucous membrane that is continuous above and behind with that of the pharynx and below with that of the trachea. Figure 2.4 Ligaments, membranes, and cartilages of the larynx seen from behind. The infantile larynx is both absolutely and relatively smaller than the larynx of the adult. The lumen is therefore disproportionately narrower. It is more funnel-shaped and its narrowest part is at the junction of the subglottic larynx with the trachea. A very slight swelling of the lax mucosa in this area may thus produce a very serious obstruction to breathing. The laryngeal cartilages are much softer in the infant and therefore collapse more easily in forced inspiratory efforts. The infantile larynx starts high up under the tongue and with development assumes an increasingly lower position. The shield-like cartilage (see Figs. 2.3 and 2.4) is the longest of the laryngeal cartilages and consists of two laminae that meet in the midline inferiorly, leaving an easily palpable notch, the thyroid notch, between them above. The angle of fusion of the laminae is approximately 90 degrees in men and 120 degrees in women. In men, the fused anterior borders form a projection, again easily palpable, which is the laryngeal prominence or Adam’s apple. A small narrow strip of cartilage, the intrathyroid cartilage, separates the two laminae anteriorly in childhood. Posteriorly, the laminae diverge and the posterior border of each is prolonged as two slender processes, the superior and the inferior cornua. The superior cornu is long and narrow and curves upward, backward, and medially, ending in a conical extremity to which the lateral thyroid ligament is attached. The inferior cornu is shorter and thicker and curves downward and medially. On the medial surface of its lower end, there is a small oval facet for articulation with the cricoid cartilage. On the external surface of each lamina, an oblique line curves downward and forward from the superior thyroid tubercle, situated just in front of the root of the superior horn, to the inferior thyroid tubercle on the lower border of the lamina. This line marks the attachments of the thyrohyoid, sternothyroid, and inferior constrictor muscles. The inner aspects of the laminae are smooth and are mainly covered by loosely attached mucous membrane. The thyroepiglottic ligament is attached to the inner aspect of the thyroid notch, and below this, and on each side of the midline, the vestibular and vocal ligaments and the thyroarytenoid, thyroepiglottic, and vocalis muscles are attached. The fusion of the anterior ends of the two vocal ligaments produces the anterior commissure tendon, which is of importance in the spread of carcinoma. The superior border of each lamina gives attachment to the corresponding half of the thyrohyoid ligament. The inferior border of each half is divided into two by the inferior tubercle. The cricothyroid membrane is attached to the inner aspect of the medial portion of the inferior border of the thyroid cartilage. The cricoid cartilage (see Figs. 2.3 and 2.4) is the only complete cartilaginous ring present in the air passages. It forms the inferior part of the anterior and lateral walls and most of the posterior wall of the larynx. Likened to the signet ring, it comprises a deep broad quadrilateral lamina posteriorly and a narrow arch anteriorly. Near the junction of the arch and lamina, an articular facet is present for the inferior cornu of the thyroid cartilage. The lamina has sloping shoulders, which carry articular facets for the arytenoids. These joints are synovial with capsular ligaments. Rotation of the cricoid cartilage on the thyroid cartilage can take place about an axis passing transversely through the joints. A vertical ridge in the midline of the lamina gives attachment to the longitudinal muscle of the esophagus and produces a shallow concavity on each side for the origin of the posterior cricoarytenoid muscle. The entire surface of the cricoid cartilage is lined with mucous membrane. The two arytenoid cartilages (see Fig. 2.4) are placed close together on the upper and lateral borders of the cricoid lamina. Each is an irregular three-sided pyramid with a forward projection, the vocal process, attached to the vocal folds and also a lateral projection, the muscular process, to which the posterior cricoarytenoid and lateral cricoarytenoid muscles are attached. Between these two processes is the anterolateral surface that is irregular and divided into two fossae by a crest running from the apex. The upper triangular fossa gives attachment to the vestibular ligament and the lower to the vocalis and lateral cricoarytenoid muscles. The apex is curved backward and medially and is flattened for articulation with the corniculate cartilage to which the aryepiglottic folds are attached. The medial surfaces are covered with mucous membrane and form the lateral boundary of the intercartilaginous part of the rima glottidis. The posterior surface is covered entirely by the transverse arytenoid muscle. The base is concave and presents a smooth surface for articulation, with the sloping shoulder on the upper border of the cricoid lamina. The capsular ligament of this synovial joint is lax, allowing both rotatory and medial and lateral gliding movements. In humans, the cylindrical articulating surfaces permit a greater range of gliding movement than of rotatory movement, and the shape of the open human glottis resembles a “V.” A firm posterior cricoarytenoid ligament prevents forward movement of the arytenoid cartilage. The corniculate cartilages (see Fig. 2.4) are two small conical nodules of elastic fibrocartilage that articulate as a synovial joint, or which are sometimes fused, with the apices of the arytenoid cartilages. They are situated in the posterior parts of the aryepiglottic folds of the mucous membrane. The cuneiform cartilages are small, paired, elongated flakes of elastic fibrocartilages placed in each margin of the aryepiglottic fold. The epiglottis is a thin, leaf-like sheet of elastic cartilage that projects upward behind the tongue and the body of the hyoid bone (see Figs. 2.3 and 2.4). The narrow stalk is attached by the thyroepiglottic ligament to the angle between the thyroid laminae, below the thyroid notch. The upper broad part is directed upward and backward, and its superior margin is free. The sides of the epiglottis are attached to the arytenoid cartilages by the aryepiglottic folds of the mucous membrane that, together with the free edge of the epiglottis, form the anterior boundary to the inlet of the larynx. The posterior surface of the epiglottis is concave and smooth but a small central projection, the tubercle, is present in the lower part. The bare cartilage is indented by a number of small pits into which mucous glands project. The anterior surface of the epiglottis is free and is covered with mucous membrane that is reflected on to the pharyngeal part of the tongue and the lateral wall of the pharynx, forming a median glossoepiglottic fold and two lateral glossoepiglottic folds. The depression formed on each side of the median glossoepiglottic fold is the vallecula. An elastic ligament, the hypoepiglottic ligament, connects the lower part of the epiglottis to the hyoid bone in front. The space between the epiglottis and the thyrohyoid membrane is filled with fatty tissue and is named the preepiglottic space. The epiglottis is not functionally developed in humans in that respiration, deglutition, and phonation can take place almost normally even if it has been destroyed. In neonates and infants, however, the epiglottis is omega-shaped. This long, deeply grooved, “floppy” epiglottis more closely resembles that of aquatic mammals and is more suited to its function of protecting the nasotracheal air passage during suckling. The corniculate and cuneiform cartilages, the epiglottis, and the apices of the arytenoids consist of elastic fibrocartilage, which shows little tendency to calcify. The thyroid, cricoid, and greater part of the arytenoids consist of hyaline cartilage, which begins to calcify in a person’s late teens or early twenties. Calcification of the thyroid cartilage starts in the region of the inferior cornu and proceeds anteriorly and superiorly until the entire rim is involved. A central translucent window persists into old age. Calcification of the posterior part of the lamina of the cricoid and of the posterior part of the arytenoid may be confused at radiology with a foreign body (see also section “Applied Anatomy of the Larynx” later in the chapter). Calcification of the body and muscular process of the arytenoid takes place later in the 4th decade, but the vocal process tends not to ossify. The extrinsic ligaments (Fig. 2.5; see also Figs. 2.3 and 2.4) connect the cartilage to the hyoid bone and trachea. The thyrohyoid membrane stretches between the upper border of the thyroid and the upper border of the posterior surfaces of the body and greater cornu of the hyoid bone. The membrane is composed of fibroelastic tissue and is strengthened anteriorly by condensed fibrous tissue called the median thyrohyoid ligament. The posterior margin is also stretched to form the lateral thyrohyoid ligament that connects the tips of the superior cornu of the thyroid cartilage to the posterior ends of the greater cornu of the hyoid bone. The ligaments often contain a small nodule, the cartilago triticea. The membrane is pierced by the internal branch of the superior laryngeal nerve and by the superior laryngeal vessels. The cricotracheal ligament unites the lower border of the cricoid cartilage with the first tracheal ring. The hypoepiglottic ligament connects the epiglottis to the back of the body of the hyoid bone. The intrinsic ligaments (see Fig. 2.5) connect the cartilages themselves, and together they strengthen the capsule of the intercartilaginous joints and form the broad sheet of fibroelastic tissue, the fibroelastic membrane, which lies beneath the mucous membrane of the larynx and creates an internal framework. The fibroelastic membrane is divided into an upper and lower part by the laryngeal ventricle. The upper quadrilateral membrane extends between the border of the epiglottis and the arytenoid cartilage. The upper margin forms the frame of the aryepiglottic inlet; the lower margin is thickened to form the vestibular ligament that underlies the vestibular fold or false cord. The lower part is altogether a thicker membrane, containing many elastic fibers. It is commonly called the cricovocal ligament, cricothyroid ligament, or, by a more loose term, the conus elasticus. It is attached below to the upper border of the cricoid cartilage and above is stretched between the midpoint of the laryngeal prominence of the thyroid cartilage anteriorly and the vocal process of the arytenoid behind. The free upper border of the membrane constitutes the vocal ligament and the framework of the vocal fold or true cord. Anteriorly, there is a thickening of the membrane, the cricothyroid ligament, which links the cricoid and the thyroid cartilage in the midline. (For cricothyrotomy, see section “Applied Anatomy of the Larynx” later in the chapter.) Figure 2.5 Ligaments and membranes of the larynx seen laterally. The cavity of the larynx extends from the pharynx at the laryngeal inlet to the beginning of the lumen of the trachea at the lower border of the cricoid cartilage and is divided by the vestibular and vocal folds into three compartments. The superior vestibule is above the vestibular folds, the ventricle or sinus of the larynx lies between the vestibular and vocal folds, and the subglottic space extends from the vocal folds to the lower border of the cricoid cartilage (see Fig. 2.5). The fissure between the vestibular folds is called the rima vestibuli and that between the vocal folds is the rima glottidis or glottis. The paraglottic and preepiglottic spaces, which are of importance in the spread of tumors, lie within the larynx. The laryngeal inlet is bound superiorly by the free edge of the epiglottis and on each side by the aryepiglottic folds. Posteriorly, the inlet is completed by the mucous membrane between the two arytenoid cartilages. This region of the larynx was formerly termed the posterior commissure but is now correctly called the posterior glottis.7 There is a plentiful supply of mucous glands in the margins of the aryepiglottic folds. The superior vestibule lies between the inlet of the larynx and the level of the vestibular folds. It narrows as it extends downward, and the anterior wall, which is the posterior surface of the epiglottis, is much deeper than the posterior wall, which is formed by mucous membrane covering the anterior surface of the arytenoid cartilages. The lateral walls are formed by the inner aspect of the aryepiglottic folds. The pre-epiglottic space is a wedge-shaped space lying in front of the epiglottis and is bound anteriorly by the thyrohyoid ligament and the hyoid bone. Above a deep layer of fascia, the hypoepiglottic ligament connects the epiglottis to the hyoid bone. It is continuous laterally with the paraglottic space that is bound by the thyroid cartilage laterally, the conus elasticus and quadrangular membrane medially, and the anterior reflection of the pyriform fossa mucosa posteriorly. It embraces the ventricles and saccules. The middle part of the cavity (and ventricle) lies between the vestibular and vocal folds that cover the ligaments of the same name. On each side, it opens, through a narrow horizontal slit, into an elongated recess, the laryngeal ventricle or sinus. From the anterior part of the ventricle, a pouch, the saccule of the larynx, ascends between the vestibular folds and the inner surface of the thyroid cartilage. It may extend as far as the upper border of the cartilage; indeed, in some monkeys and apes, it extends even further into the neck, as far as the axilla. In humans, the saccule occasionally protrudes through the thyrohyoid membrane. The mucous membrane lining the saccule contains numerous mucous glands, lodged in submucous alveolar tissue. Fibrous tissue surrounds the saccule and a limited number of muscle fibers pass from the apex of the arytenoid cartilage across the medial aspect of the saccule to the aryepiglottic fold. The muscle is presumed to compress the saccule and to express the secretion of its mucous glands over the surface of the vocal folds. The vestibular folds are two thick, pink folds of mucous membrane, each enclosing a narrow band of fibrous tissue, the vestibular ligament, which is fixed in front to the angle of the thyroid cartilage, just below the attachment of the epiglottic cartilage, and behind to the anterolateral surface of the arytenoid cartilage, just above the vocal process. The vocal folds are defined as two fold-like structures that extend from the middle of the angle of the thyroid cartilage to the vocal processes of the arytenoid cartilages. Each fold is a layered structure. The vocal fold consists of mucosa and muscle. The mucosa is subdivided into the epithelium, which is of the stratified squamous type, and the lamina propria, which consists of superficial, intermediate, and deep layers (Fig. 2.6A). The superficial layer of the lamina propria, referred to as Reinke space, is made of loose fibrous substance that can be likened to a mass of soft gelatin. It is this layer that vibrates most significantly during phonation. If it becomes stiff due to some pathological state, such as inflammation, tumor, or scar tissue, its vibrations are disturbed and voice problems result. The intermediate layer, consisting mainly of elastic fibers, and the deep layer, consisting of collagenous fibers rich in fibroblasts, together form the vocal ligament, deep to which is the vocalis muscle that constitutes the main body of the vocal fold. Around the edge of the vocal fold, the elastic and collagenous fibers in the lamina propria and the muscle fibers of the vocalis muscle run parallel to the edge. The layered structure is not uniform along the length of the vocal fold (refer to Figs. 2.6B and 2.7). At the anterior end, there is a mass of collagenous fibers that appear to be connected to the inner perichondrium of the thyroid cartilage anteriorly and to the deep layer of the lamina propria posteriorly. Posterior to this mass of collagenous fibers, there is another mass of elastic fibers, continuous with the intermediate layer of lamina propria, called the anterior macula flava. A similar picture is seen at the posterior end of the membranous part of the vocal fold. These structures at both ends of the membranous vocal folds appear to serve as cushions to protect the ends from mechanical damage caused by vocal fold vibration. Figure 2.6 (A) Coronal section of the vocal fold at the midmembranous part. (B) Horizontal section of the anterior and posterior ends of the membranous part of the vocal fold. E, epithelium; LP, lamina propria; LPd, deep; LPi, intermediate; LPs, superficial layers; VL, vocal ligament; M, vocal muscle.
Development of the Larynx, Trachea, Bronchi, and Lungs
Larynx and Trachea
Larynx
Comparative Anatomy and Modification of Olfaction and Deglutition
Descriptive Anatomy
Laryngeal Cartilages
Thyroid Cartilage
Cricoid Cartilage
Arytenoid Cartilages
Corniculate and Cuneiform Cartilages
Cartilage of the Epiglottis
Calcification of Laryngeal Cartilages
Ligaments
Extrinsic Ligaments
Intrinsic Ligaments
Interior of the Larynx
Laryngeal Ventricle and the Vestibular Folds
Vocal Folds
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


