Key points
- •
Sinonasal malignancy is rare in general but with an understanding of anatomy from an endonasal perspective many of these lesions may be dealt with using a totally endoscopic approach.
- •
Preservation of normal nasal structures should be given consideration when possible to restore function to the nose following surgery.
- •
The sphenoid bone is central in the nasal cavity and contains several landmarks of great importance. An understanding of this anatomy is crucial to endonasal surgery.
- •
The clivus may be subdivided into thirds, which extend from the dorsum sella superiorly to the region just deep to the nasopharynx inferiorly.
- •
Knowledge of the anatomic structures surrounding the pterygopalatine space and pterygoid region allows lateral dissection when lesions dictate this approach.
Introduction
Malignancies of the sinonasal region and ventral skull base include a varied group of uncommon tumors that are a challenge to treat. These malignancies, with few exceptions, often present late because of their insidious growth and bland symptomatology. Common symptoms include sinusitis, nasal obstruction, facial pain, epistaxis, and headache. Patients often suffer a protracted course to diagnosis given these inconspicuous symptoms and tend to present with advanced lesions. As with malignancies of other sites, the primary goal in surgical management is complete resection with negative margins. This presents a unique surgical challenge in that these lesions lie within a region of densely populated anatomic real estate where extension of tumors beyond the confines of their site of origin may put highly important structures at great risk. This fact reinforces the importance of complete preoperative work-up and a sound anatomic understanding.
Introduction
Malignancies of the sinonasal region and ventral skull base include a varied group of uncommon tumors that are a challenge to treat. These malignancies, with few exceptions, often present late because of their insidious growth and bland symptomatology. Common symptoms include sinusitis, nasal obstruction, facial pain, epistaxis, and headache. Patients often suffer a protracted course to diagnosis given these inconspicuous symptoms and tend to present with advanced lesions. As with malignancies of other sites, the primary goal in surgical management is complete resection with negative margins. This presents a unique surgical challenge in that these lesions lie within a region of densely populated anatomic real estate where extension of tumors beyond the confines of their site of origin may put highly important structures at great risk. This fact reinforces the importance of complete preoperative work-up and a sound anatomic understanding.
Anterior ventral skull base
Nasal Cavity
The nasal cavity forms the corridor though which sinonasal and ventral skull base malignancies may be approached. This corridor serves many physiologic functions that can be compromised during endonasal surgery of these lesions. The nasal cavity is lined with ciliated respiratory epithelium, which aids in transport of a bilayer mucus blanket designed as a first line of defense against pathogens and irritants. Dysfunction of this mucosal lining may lead to stagnation of mucus, crusting, infection, and secondary osteitis. This mucosa may be used to reconstruct defects created by surgery in the form of local axial flaps. The nasoseptal flap and the inferior turbinate or lateral wall flap are two examples. In the midline the nasal septum is formed as a coalescence of the quadrangular cartilage anteriorly, the vomer inferior and posteriorly, and the perpendicular plate of the ethmoid bone superior and posteriorly. The mucosa covering the septum receives its blood supply from multiple sources, chiefly the labial artery anteriorly, the anterior and posterior ethmoidal arteries, and the posterior septal branch of the sphenopalatine artery at the posterior aspect. The posterior septal branch is preserved and used to form the pedicle for the nasoseptal flap. The high septal mucosa is termed olfactory epithelium because it harbors the olfactory fila transmitted via the cribriform plate. These are preserved if the dissection does not travel high into the nasal vault until the head of the middle turbinate, a rough landmark for the anterior limit of the cribriform, is reached. Along the lateral wall of the nasal cavity lie the turbinates. The inferior turbinate is a process of the maxillary bone and posteriorly the palatine bone. Its role in the nasal cavity seems to be related to aid in the dispersion of airflow throughout the nasal cavity allowing for efficient warming and humidification of air before passing to the lungs. These structures can become enlarged affecting transnasal surgical access; however, caution should be taken when considering removal unless tumor dictates. Complete removal of the inferior turbinate is a risk factor for development of paradoxic congestion despite adequate airway space, often with associated crusting and nasal dryness. “Outfracture” or lateralization of these structures is often sufficient to provide additional space after topical decongestion has been performed. The middle turbinate is a product of the ethmoid bone and is situated in the mid nasal cavity forming the medial aspect of the middle meatus. It has multiple attachment sites, one oriented vertically attaching to the skull base and the other, termed the basal lamella, to the lateral wall. The basal lamella anatomically separates the anterior and posterior ethmoid air cells, and it is just anterior to this structure that the sphenopalatine artery emerges from the pterygopalatine space. The middle turbinate increases the overall surface area of the nasal mucosa and when pneumatized has been postulated to have a protective effect against allergens. When using the nasal cavity as a corridor for tumor extirpation, this structure presents a challenge in terms of access and management. Some argue for preservation of these structures when possible, whereas others advocate removal. For tumors of the anterior ventral skull base the middle turbinate is generally removed early. Studies looking at the effects of turbinate removal have not brought consensus as to the effect of this removal. When approaching the posterior skull base, the middle turbinate may be preserved by lateralization with firm but gentle pressure so as to minimize mucosal trauma and subsequent bleeding. This significantly narrows the middle meatus and the turbinate does not typically recover its normal position. Lateralization has been studied after sinus surgery and it does not seem to correlate with increase in patient symptoms. The group did elucidate that the frontal sinus may be affected by this phenomenon; however, this is likely secondary to scarring after the frontal recess has been dissected for sinus disease.
The Skull Base
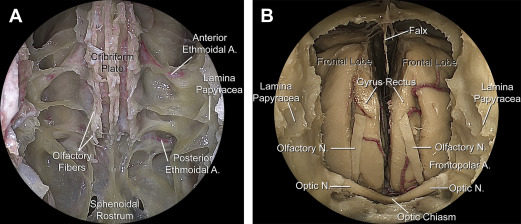
The anterior ventral skull base is comprised chiefly of the ethmoid and frontal bones, with the posterior third being formed by the planum sphenoidale. The components of the ethmoid bone are the cribriform plate and crista gali centrally; the roof or fovea ethmoidalis superiorly; the lamina papyracea laterally; and the perpendicular plate, which joins with the vomer inferiorly. The ethmoidal air cells lie within the bounds of the frontal recess anteriorly to the face of the sphenoid sinus posteriorly. The most anterior ethmoid air cell is termed the agger nasi cell and endoscopically appears as a bulge of the lateral wall at the axilla of the middle turbinate. The agger nasi cell is consistently present in more than 90% of cases. Removal of this cell and its roof or “cap” is a key in the operative unveiling of the frontal sinus outflow pathway. Beyond the frontal outflow, moving posteriorly, lies the supraorbital ethmoid cell. This cell is present in just over 50% of cases and helps one to identify the position of the anterior ethmoidal artery. The anterior ethmoidal artery may persist within a mesentery below the skull base within the posterior wall of this cell, or be found at the anterior ventral skull base just beneath a thin layer of bone. In any case it is reliably found within, or in continuity with, the posterior wall of the supraorbital ethmoid cell. Its trajectory is oblique, moving anteriorly as is courses from the medial orbit across the skull base medially ( Fig. 1 A). This subtle finding is helpful in cases where the artery is not obvious. Proceeding more posterior, the posterior ethmoidal artery is encountered after a distance of 10 to 12 mm from the anterior ethmoidal artery as it exits the orbit. This artery is typically found within the bone of the anterior ventral skull base, taking a more direct course medially as it traverses the skull base. After the ethmoid air cells have been cleared from the skull base and the ethmoidal arteries controlled, completion of a Draf III frontal sinusotomy may be performed. This procedure removes a portion of the high anterior septum just in front of the middle turbinate and unifies the frontal sinuses into a common cavity (horseshoe shaped) allowing access to the anterior portion of the cribriform. Traditionally, the first olfactory fila was identified along the lateral lamella of the cribriform heralding the posterior limit of the dissection at the outside. In recent years this practice has fallen out of vogue with some citing a risk of creating a cerebrospinal fluid leak. In any case these fibers are often seen at some point in the course of the dissection. After completing the Draf III, osteotomies along the fovea ethmoidalis bilaterally are made. The anterior osteotomy should only be made after dissecting the crista gali free from the falx cerebri. After bony removal is completed only the dura separates the surgeon from the fronto-orbital branches of the anterior cerebral artery ( Fig. 1 B). These vessels supply the olfactory bulbs and the cortical surface. Medially the frontopolar vessels run within the interhemispheric fissure. When tumor is present care must be taken as dissection is carried to the superior aspect of the tumor because the fronto-orbital vessels often lie draped over the top. These vessels are intimately associated with the gyrus rectus and olfactory bulbs on each side of the falx.
Olfaction is an important sensory function unique to the nasal cavity and an important part of the human experience. The olfactory bulbs lie within the ventral skull base on the intracranial side of the cribriform plate transmitting sensory fila via tiny perforations in the bone. Overlying these fila is the olfactory epithelium, which exists in specific distributions within the nasal cavity. This lining may be preserved in some cases of malignancy to maximize the chance of olfaction postsurgically. However, this should not influence the decision to obtain negative surgical margins intraoperatively. The anterior ventral skull base is a region often involved in sinonasal malignancy. Intricate knowledge of the vascular anatomy is important because these vessels are often involved as “feeder” vessels to tumors. Appropriate patient counseling regarding expected functional outcomes after surgery with regard to sense of smell is also important because this is often impacted during surgery in this region.
Sphenoid sinus and posterior ventral skull base
Sphenoid Sinus
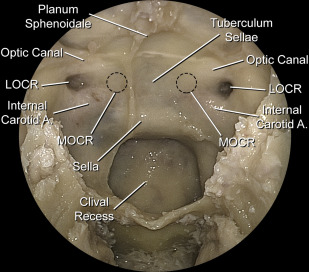
The sphenoid sinus lies at the far posterior aspect of the nasal cavity. The sphenoid ostium lies at the inferomedial aspect of the sphenoethmoidal recess, usually veiled behind the superior turbinate. The superior turbinate also arises from the ethmoid bone, and contains a small fraction of olfactory epithelium. It is a reliable landmark for the sphenoid ostium, which lies inferomedially to it. The superior turbinate is sometimes resected during sphenoid sinus exposure. After removal of the inferior half of the superior turbinate, the ostium usually comes into view. The sinus should be entered in a safe fashion, low and medial, to avoid injury to critical structures that lie beyond. Whether a transethmoidal approach or transnasal approach is taken, the point of entry is the same. In the case of an Onodi cell, the posterior-most ethmoid cell may extend beyond the face of the sphenoid pushing it inferiorly. This is significant because the optic canal often has bony dehiscences, and if the surgeon presumes to be in the sphenoid when actually in an Onodi cell, there is potential for injury to the optic nerve. This finding is easily noted preoperatively by careful examination of the preoperative imaging. Within the sphenoid sinus are several important anatomic landmarks that are easily seen in a well-pneumatized sinus ( Fig. 2 ). These landmarks serve as a roadmap for surgical dissection, but also demonstrate the proximity of the sinus to crucial structures. The sphenoid pneumatization is generally categorized into one of three distinct classifications: (1) conchal, (2) presellar, or (3) sellar (although a postsellar configuration has been described). Identification of landmarks is typically the most challenging in the conchal pattern because of masking by thick bone. Pneumatization of the lateral recess of the sphenoid sinus expands the cavity further in some cases. The sella turcica lies centrally and is situated above the clival recess in a pneumatized sinus. The lateral aspects of the clival recess may at times look like pillars because of the bony covering of the paraclival carotid artery segments. Adjacent to the sella, the carotid prominences may be seen often given away by a telltale pinkish hue appreciated by the keen observer. The carotid prominence, or paraclinoidal carotid segment, is the anterior-most projection of the carotid because it loops back on itself wrapping about a small bony depression. This depression is the middle clinoid, which may be removed in cases where a complete bony ring connecting the anterior and middle is not present. Superolateral to the prominence lies a depression in the bone indicating the lateral opticocarotid recess, and the optic nerve immediately superior. The medial opticocarotid recess lies approximately 5 mm medial to the lateral opticocarotid recess and is also a consistent landmark (see Fig. 2 ). The ophthalmic artery approaches the orbit along a path in the roof of the lateral opticocarotid recess nestled beneath the optic nerve. This becomes crucial during optic decompression because the dura around the optic nerve is always incised superiorly so as not to inadvertently injure this artery.