Chapter 70 Amblyopia management
Amblyopia is the most common cause of visual impairment in children: it often persists into adulthood. The prevalence in childhood is estimated to be 1−4%. It is considered to be the leading cause of monocular vision loss in the 20- to 70-year-old age group.1 The prevalence of visual loss from amblyopia was 2.9% in one study of adults, indicating the need for improved treatment.2 Amblyopia is defined as a “decrease of visual acuity caused by pattern vision deprivation or abnormal binocular interaction for which no causes can be detected by the physical examination of the eye and which, in appropriate cases, is reversible by therapeutic measures.”3 Amblyopia may be unilateral or less often bilateral.
Most cases are associated with eye misalignment, usually esotropia in infancy or early childhood, others with anisometropia, or a combination of strabismus and anisometropia (Table 70.1).
Table 70.1 Association of amblyopia with strabismus and/or amblyopia
| Woodruff et al.4 | Shaw et al.5 | |
|---|---|---|
| Number of cases | 961 | 1531 |
| Strabismus as the cause | 57% | 45% |
| Anisometropia as the cause | 17% | 17% |
| Combined strabismus and anisometropia | 27% | 35% |
Precise percentages vary depending on how amblyopia is defined.
Visual loss in amblyopia varies from mild to severe. About 25% of cases have visual acuity worse than 6/30 and about 75% 6/30 or better.4,6–8 The extent of the deficit may not be equivalent, but vary by cause. Strabismic amblyopia may represent a more severe physiologic deficit than isolated anisometropic amblyopia and combined strabismic and anisometropic amblyopia is a more serious deficit still.9
Methods of detection
The gold standard for detection is measurement of visual acuity using a crowded or linear letter optotype test. Single optotype presentation and picture optotypes are less sensitive and should be used only when a child is unable to perform a test using surrounded or line optotypes. Tests based on the four letters “H”, “O”, “T”, and “V” in a box or with contour surround bars are the basis of several popular test strategies.10,11 A defined protocol for testing children with single-surround HOTV has been developed by the Pediatric Eye Disease Investigator Group.11 The strategy includes a second chance at threshold determination and a portion designed to get the child back on track with some larger above threshold stimuli. It has good testability, test−retest reliability, and has been automated.12
For children unable to perform with letter optotypes, clinicians have commonly used picture optotypes. However, standard picture optotypes overestimate the visual acuity of amblyopic eyes and are not recommended for screening or diagnosis of amblyopia. Dr. Lea Hyvärinen designed four picture-like optotypes13 to have similarities between optotypes and have contours like the Landolt C making them more difficult to successfully recognize. The objects (apple, circle, house, square) chosen are common in Western children’s experience and eliminate cultural biases in that population. In one study the single-surrounded Lea tests systematically overestimated acuity by 1.9 lines compared to the crowded Landolt C in normal eyes.14 A comparison of the Lea symbols to line optotypes in amblyopic eyes has not been thoroughly studied.
Fixation preference testing may be used for children unable to perform any optotype-based testing. For strabismic children the clinician compares the ability to hold fixation with each eye. The child may alternate, be unable to hold fixation after a blink, or be unable to hold fixation. For a patient with no misalignment, the test is performed by placing a 10 diopter prism base down before one eye, having the child fixate a detailed target at distance or near, and assessing fixation preference. If there is a fixation preference for the eye without the prism, switch the prism to the fellow eye and again assess fixation preference. The prism might cause the other eye to be preferred. If the same eye is preferred under each testing condition, then the fellow eye is assumed to have amblyopia. A patient who fixates with the eye without the prism is alternating. Amblyopia therapy may be prescribed for a definite fixation preference as discussed in the sections on treatment. Comparing fixation preference testing to optotype testing has shown fixation preference testing is unreliable as a means of diagnosing amblyopia, generally leading to an over-diagnosis of amblyopia. Optotype testing confirmed only 17 of 52 patients (33%) diagnosed with amblyopia by fixation preference testing.15 In another study 53 children had two or more lines of difference in visual acuity, yet 45 were graded as normal by fixation preference.
Forced choice preferential looking using Teller acuity cards has been used as an alternative method for infants and non-verbal infants.16 This test is time consuming and requires an experienced tester to assure reliable results. Unfortunately, this test systematically underestimates amblyopia, reducing its clinical utility as a means of screening or detecting a successful treatment endpoint.17
Methods of treatment
There are few data comparing the outcomes of amblyopia treatment to the natural history. Clinicians have noted improvement of acuity when children complied with therapy, but found little improvement when no therapy was actually completed. Simons and Preslan reported that among a case series of amblyopic patients, who were not treated, there was no improvement in visual acuity.18 However, such a demonstration of improvement in acuity of the amblyopic eye without concurrent untreated or natural history controls is not sufficient to prove a benefit of therapy. This deficiency led to a recommendation in the United Kingdom to stop screening for amblyopia as well as treating it because of a lack of a proven benefit.19 A recent retrospective, non-randomized study suggested that there is value. A group of strabismic patients with amblyopia were treated with spectacles alone (n=17) or spectacles plus occlusion therapy (n=69).20 Though both treatments led to improvement, the visual acuity improved more in the patients treated with occlusion.
It is likely that some of the improvement in acuity reported in uncontrolled studies of amblyopia therapy represents a combination of age and learning effects in addition to actual treatment benefit., However, the magnitude of the age and learning effect, which has been reported to be about 0.14 logMAR lines over 6 months in a prospective clinical trial, is far less than the improvement typically reported following treatment of amblyopia.21
A randomized clinical trial (Amblyopia Treatment Trial, UK) was undertaken to compare an untreated control group of anisometropic amblyopia with a group of children treated with glasses and a third group treated with glasses and occlusion. This study found slight improvement with about one line between no treatment and treatment with glasses and occlusion.22 The cause of the visual loss was not known with certainty in each child. In addition, the control group’s visual acuity at baseline and at final measurement was without correction, whereas the treatment group was measured with best spectacle correction.
Refractive correction
When should one start additional therapy such as occlusion? Some clinicians prescribe such therapy immediately, some wait a specified time, others wait until improvement with spectacles alone ceases. Moseley et al. found that 8 of 12 patients prescribed spectacles for the first time improved 3 or more lines in the amblyopic eye.23 The Pediatric Eye Disease Investigator Group (PEDIG) reported that amblyopia improved in previously untreated anisometropic patients (n=84) with optical correction by at least 2 lines in 77% of the patients and resolved in 27%.24 Improvement took up to 30 weeks for stabilization. In a pilot project, subjects with strabismic amblyopia experienced similar improvement.
Occlusion therapy
Occlusion therapy has been the mainstay of treatment for a century despite the lack of meaningful data demonstrating its superiority over other modalities. This therapy commonly employs an adhesive patch placed over the fellow eye so that the amblyopic eye must be used. Opinions vary on the number of hours of patching per day that should be prescribed, ranging from a few hours to all waking hours.1,3,25–28
Flynn et al. found that the success rates were the same for part-time and full-time occlusion therapy based on reported outcomes in 23 studies.29 Cleary reported in a very small study that full-time occlusion produced a greater improvement in visual acuity and reduction in interocular difference than part-time occlusion, when the acuity outcome was measured at 6 months.20
Several authors have reported significant improvement in visual acuity using brief daily periods of occlusion (20 minutes to 1 hour).30,31 Campbell et al. noted that 20 minutes per day was effective in improving the vision of 83% of children to 6/12. These authors reported that vision can improve rapidly following brief periods of occlusion, especially when combined with concentration on hard tasks.32
The dosages prescribed by clinicians during the last few decades vary greatly and seem to be largely a matter of region or training.33 For instance, more hours are prescribed in German speaking countries than in the United Kingdom, yet the same outcome is expected.34 Several clinical trials have evaluated various patching dosages and the outcome of amblyopia treatment.21,35 These are the Amblyopia Treatment Studies, which are prospective multi-center randomized controlled clinical trials, being conducted by PEDIG in North America. The studies have included only patients with strabismic and anisometropic forms of amblyopia. The first randomized controlled study compared occlusion to atropine treatment. The dosage of occlusion prescribed was a minimum of 6 hours up to full-time, but the investigator chose the actual occlusion dosage. Patients with acuity of 6/24 to 6/30 improved faster when more hours of patching were prescribed, but after 6 months the improvement was not significantly greater than that occurring with fewer hours of patching or with atropine (Fig. 70.1).35
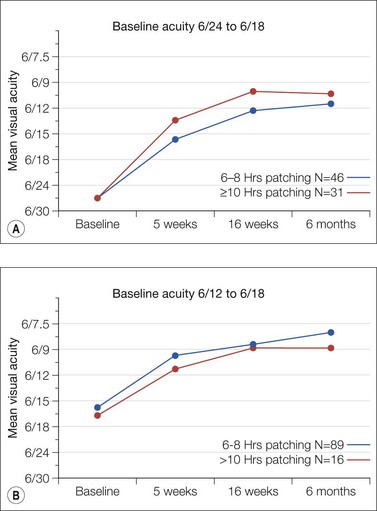
Fig. 70.1 Initial prescribed dosage of patching versus mean visual acuity from a randomized controlled trial.21 Eighty percent of patients remained on their initial dosage throughout the study. Unsuccessful patients in each subgrouping had patching of 12 or more hours prescribed at the 17-week visit. (A) Patients with amblyopic eye acuity of 6/24 and 6/30. The patients initially treated with 10 or more hours compared to 6 or 8 hours per day had a faster rate of improvement, but by 6 months there was no significant difference in outcome. (B) Patients with amblyopic eye acuity of 6/12 to 6/18. There is no difference in the rate or magnitude of improvement between those initially treated with 10 or more hours compared to those with 6 or 8 hours.
Additional prospective randomized trials compared the efficacy of different occlusion dosages. There are two distinct studies, one for moderate amblyopia 6/12 to 6/24, and one for severe amblyopia 6/30 to 6/120, caused by strabismus, anisometropia, or both.36,37 The studies found that 2 hours of daily patching produces an improvement in visual acuity of similar magnitude to the improvement produced by 6 hours of daily patching in treating moderate amblyopia in children aged 3 to less than 7 years.36 Each treatment group improved 2.4 lines over 4 months. More interesting was the lack of any benefit in terms of the rate of improvement (Fig. 70.2). The visual acuity gain after 4 months probably does not represent the maximum improvement possible.
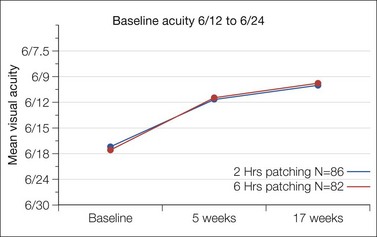
Fig. 70.2 Occlusion dosage of 2 versus 6 hours compared in a randomized controlled trial.36 No increase in therapy was allowed by the protocol. There was no difference in the rate or magnitude of improvement during the 4 months of prescribed treatment.
The study for severe amblyopia found the improvement in the amblyopic eye acuity from baseline to 4 months averaged 4.8 lines in the 6-hour group and 4.7 lines in the full-time group (P = 0.45).37 In a recent study, children with severe amblyopia improved a mean of 3.6 lines with just 2 hours of daily patching for 17 weeks.38
Children’s dislike of occlusion therapy is well known.39 Reported compliance rates range widely. Parents have used coercion and clinicians have prescribed punitive measures such as elbow splints to enhance compliance. Lack of parental understanding seems to play a large role. In the United Kingdom, failure to comply with the prescribed regimen at least 80% of the time occurred in 54% of patients:40 the failure to comply related to the parents’ lack of understanding that there is a “critical period” for effective therapy.
Side effects from occlusion are uncommon, usually minor skin irritation or the social stigma of a patch.21 Adhesive sensitivity to the patches does occur. The clinician should discontinue the patch and treat with an emollient facial cream. Rarely, topical hydrocortisone may be needed.
More serious is occlusion amblyopia, a decrease in vision in the fellow (patched) eye of more than one line. It is more common with more intense therapy and longer treatment intervals, especially if the patient is lost to follow-up. In one prospective study in which the majority of patients were treated with 6 or 8 hours of occlusion per day,21 only 1 of 204 patients was diagnosed with reverse amblyopia. In most cases occlusion amblyopia is reversible simply by stopping the treatment. Rarely, amblyopia therapy is needed for the originally non-amblyopic eye.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


