(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
Amaurosis fugax is a transient brief blindness, dimming, fogging, or blurring of vision, lasting from a few seconds to minutes or even hours, depending upon the etiology. It has also been called transient visual obscuration or blackout. It occurs in many ocular vascular occlusive disorders, i.e., central retinal artery occlusion, branch retinal arteriole occlusion, central retinal vein occlusion alone, central retinal vein occlusion with cilioretinal artery occlusion, hemicentral retinal vein occlusion, branch retinal vein occlusion, ocular ischemic syndrome, and both non-arteritic and arteritic anterior ischemic optic neuropathy. There are a few reports about amaurosis fugax in giant cell arteritis [1–7]. Amaurosis fugax may be the presenting symptom and, if so, always requires urgent evaluation. No comprehensive study on amaurosis fugax in ocular vascular occlusive disorders had been published and no detailed discussion of its pathogeneses in those disorders. Therefore, I conducted a comprehensive, systematic study in a large cohort of patients dealing with prevalence of amaurosis fugax in central retinal artery occlusion, branch retinal arteriole occlusion, central retinal vein occlusion alone, central retinal vein occlusion with cilioretinal artery occlusion, hemicentral retinal vein occlusion, branch retinal vein occlusion, ocular ischemic syndrome, both non-arteritic and arteritic anterior ischemic optic neuropathy, and giant cell arteritis [8]. Various features of all these diseases are discussed in previous chapters. In this chapter, I shall discuss only the amaurosis fugax features in them. The findings of my study are discussed in detail elsewhere [8] and following are the main features.
Prevalence of Amaurosis Fugax
Table 28.1 gives the number of eyes with various ocular vascular occlusive disorders in my study [8] and the prevalence of amaurosis fugax in them. I found that its prevalence varied widely among different ocular vascular occlusive disorders – it ranged from 0.35 % in branch retinal vein occlusion to 37.8 % in central retinal vein occlusion with cilioretinal artery occlusion. In giant cell arteritis, 32.4 % (35 of 108) of patients with ocular involvement had a history of amaurosis fugax or 26.5 % (39 of 147) of the involved eyes. Amaurosis fugax was the presenting visual symptom in 15.4 % of ocular ischemic syndrome cases. There was no difference in the nature of amaurosis fugax between the various ocular vascular occlusive disorders, except in branch retinal artery occlusion, where transient visual loss or blurring was located only in the area of supply by the occluded retinal artery. The time lapse between the development of amaurosis fugax and the occurrence of the vascular occlusion varied widely in different disorders, anywhere from a few hours to several days. There was no definite pattern at all.
Table 28.1
Prevalence of amaurosis fugax in various ocular vascular occlusive disorders
Diagnosis | N (eyes) | With amaurosis fugax | Prevalence (%) | 95 % CI |
|---|---|---|---|---|
CRAO | 271 | 33 | 12.18 | (8.53 %, 16.67 %) |
BRAO | 169 | 24 | 14.20 | (9.32 %, 20.39 %) |
CRVO | 864 | 42 | 4.86 | (3.53 %, 6.51 %) |
CRVO + CLRAO | 37 | 14 | 37.84 | (22.46 %, 55.24 %) |
Hemi-CRVO | 67 | 9 | 13.43 | (6.33 %, 23.97 %) |
BRVO | 285 | 1 | 0.35 | (0.01 %, 1.94 %) |
Ocular ischemic syndrome | 39 | 6 | 15.38 | (5.86 %, 30.53 %) |
NA-AION | 946 | 24 | 2.54 | (1.63 %, 3.75 %) |
Giant cell arteritis | 147 | 39 | 26.53 | (19.60 %, 34.44 %) |
Systemic Abnormalities
The echocardiography and carotid Doppler/angiography on the side of the involved eye was examined for patients with non-arteritic central retinal artery occlusion, branch retinal arteriole occlusion, and non-arteritic anterior ischemic optic neuropathy, because in those conditions embolism can be a causative factor [9]. The findings of these tests in non-arteritic central retinal artery occlusion and branch retinal artery occlusion are given in Table 28.2. This shows that it is essential that all patients with non-arteritic central retinal artery occlusion and branch retinal arteriole occlusion must be fully investigated for the source of embolism, irrespective of whether they have amaurosis fugax or not.
Table 28.2
Carotid Doppler/angiography and echocardiogram findings on the same side as the involved eye with amaurosis fugax in non-arteritic CRAO and BRAO
Test finding | Non-arteritic CRAO (n = 33) | BRAOa (n = 24) |
|---|---|---|
Carotid Doppler/angiography: | (n = 28) | (n = 20) |
Occlusion | ||
0–15 % | 16 (57 %) | 12 (60 %) |
16–49 % | 7 (25 %) | 2 (10 %) |
50–79 % | 2 (7 %) | 2 (10 %) |
80–99 % | 1 (3 %) | 2 (10 %) |
100 % | 2 (7 %) | 2 (10 %) |
Carotid Doppler/angiography: | (n = 26) | (n = 20) |
Plaque present | 15 (58 %) | 8 (40 %) |
Echocardiogram | (n = 16) | (n = 12) |
Normal | 5 (31 %) | 3 (25 %) |
Abnormal, no embolic source | 5 (31 %) | 2 (17 %) |
Abnormal, with embolic source | 6 (52 %) | 7 (58 %) |
Echocardiogram: | (of n = 6 with embolic source) | (of n = 7 with embolic source) |
Abnormal embolic source | ||
Mitral valve | 3 (50 %) | 2 (29 %) |
Aortic valve | 2 (33 %) | 0 (0 %) |
Mitral and aortic valves | 1 (16 %) | 5 (71 %) |
Echocardiogram: | (of n = 4 with mitral valve as embolic source) | (of n = 7 with mitral valve as embolic source) |
Mitral valve lesion types | ||
Calcified valve | 2 (50 %) | 3 (43 %) |
Mitral valve prolapse | 1 (25 %) | 0 (0 %) |
Other types of lesions | 1 (25 %) | 4 (57 %) |
Echocardiogram: | (of n = 3 with aortic valve as embolic source) | (of n = 5 with aortic valve as embolic source) |
Aortic valve lesion types | ||
Calcified valve | 3 (100 %) | 3 (60 %) |
Other types of lesions | 0 (0 %) | 2 (40 %) |
Echocardiogram: | (n = 16) | (n = 12) |
Patent foramen ovale | 0 (0 %) | 0 (0 %) |
Non-arteritic anterior ischemic optic neuropathy can rarely be due to embolism, and such patients can develop amaurosis fugax. Of the 24 eyes with amaurosis fugax in non-arteritic anterior ischemic optic neuropathy in my study [8], 12 had carotid Doppler/angiography performed on the same side as the involved eye, and in them internal carotid artery stenosis was 0–15 % in 5 (42 %), 16–49 % in 3 (25 %), 50–79 % in 1 (8 %), and 100 % occlusion in 3 (25 %). There was plaque in the internal carotid artery in 58 %. Five non-arteritic anterior ischemic optic neuropathy patients with amaurosis fugax showed valvular disease or foramen ovale. Carotid artery disease is well known to cause ocular ischemic syndrome [10, 11]. Doppler/angiography findings of internal carotid artery in ocular ischemic syndrome in my study [11] are described in Table 28.3; the majority of them had 100 % occlusion or severe (80–90 %) stenosis of the internal carotid artery.
Table 28.3
Distribution of internal carotid artery occlusion/stenosis in 32 patients with ocular ischemic disorder
Internal carotid artery disease | Number of patients (%) | |
|---|---|---|
Bilateral 100 % occlusion | 2 (6 %) | |
Bilateral 80–99 % stenosis | 2 (6 %) | |
Bilateral 0–49 % stenosis | 4 (13 %) | |
Unilateral 100 % occlusion | 21 (66 %) | |
Other side in them | 80–99 % stenosis | 5 (16 %) |
50–79 % stenosis | 3 (9 %) | |
0–49 % stenosis | 13 (41 %) | |
Unilateral 80–99 % stenosis | 1 (3 %) | |
Other side in them | 50–79 % stenosis | 0 (0 %) |
0–49 % stenosis | 1 (3 %) | |
Unilateral 50–79 % stenosis | 2 (6 %) | |
Other side | 0–25 % stenosis | 2 (6 %) |
The prevalence of cerebrovascular accident and transient ischemic attack was examined in patients with amaurosis fugax and non-arteritic anterior ischemic optic neuropathy, non-arteritic central retinal artery occlusion, and branch retinal arteriole occlusion [9]. Among 24 patients with non-arteritic anterior ischemic optic neuropathy and amaurosis fugax, two had cerebrovascular accident with a transient ischemic attack associated with 100 % occlusion of the internal carotid artery on the same side as the non-arteritic anterior ischemic optic neuropathy, and one had cerebrovascular accident associated with plaque in the internal carotid artery. Two of 234 patients with non-arteritic central retinal artery occlusion had cerebrovascular accident on the same side as the occlusion and one on the opposite side; in four patients, there was a history of transient ischemic attack, one of them associated with cerebrovascular accident. Among 141 patients with branch retinal arteriole occlusion, one had cerebrovascular accident on the same side as the occlusion and four on the opposite side; transient ischemic attack without cerebrovascular accident was present in two cases.
Pathogeneses of Amaurosis Fugax in Various Ocular Vascular Occlusive Disorders
This is an important topic for the management of these disorders; however, there is little information on it in the literature. Understanding pathogenesis is crucial to management. Based on my basic, experimental, and clinical studies [1, 2, 8–39] on all these ocular vascular occlusive disorders, following is a brief account of the pathogenesis of amaurosis fugax in each of them.
Amaurosis Fugax in Giant Cell Arteritis with Visual Loss
Amaurosis fugax in giant cell arteritis is an ominous sign of impending visual loss and requires immediate and aggressive treatment with high-dose corticosteroid therapy to prevent visual loss [1, 2]. The development of amaurosis fugax in giant cell arteritis has important clinical implications. In the literature, there are several reports of amaurosis fugax in giant cell arteritis with visual loss [1–7]; in those reports the given prevalence varies between 7 and 36 %. In my series, 32.4 % of giant cell arteritis patients with ocular involvement (or 26.53 % of the involved eyes) had a history of amaurosis fugax.
Amaurosis fugax in giant cell arteritis is almost invariably due to optic nerve head ischemia (arteritic anterior ischemic optic neuropathy). In sharp contrast to non-arteritic anterior ischemic optic neuropathy, in arteritic anterior ischemic optic neuropathy, amaurosis fugax is very common (2.5 % versus 32.4 %), and it is due to thrombosis of the posterior ciliary artery caused by giant cell arteritis. Posterior ciliary arteries supply the optic nerve head (see Chap. 5). I had the opportunity to perform fluorescein fundus angiography in a rare patient who happened to present while experiencing amaurosis fugax that revealed markedly impaired posterior ciliary artery circulation, like the following patient.
Case Report
A 74-year-old man one day noticed “floaters” in the right eye at noon for about 5–10 min. Five days later he developed a “curtain” that moved over the temporal side, and he could see only gray vision for 10 min. He saw an ophthalmologist the next day; on ophthalmoscopy she found no abnormality (Fig. 28.1a). In view of that she felt that his amaurosis fugax was due to embolism and planned to do a work-up for that. Two days later, the ophthalmologist talked to me about the case. I suggested that she ask the patient to come immediately to my clinic because the history was highly suggestive of giant cell arteritis. He was seen in my clinic that day in the afternoon. He gave a history of jaw claudication all along. Ophthalmoscopic fundus examination revealed no abnormality (Fig. 28.1a), but fluorescein fundus angiography showed marked impairment of the circulation in the medial posterior ciliary artery and central retinal artery, with delayed retinal blood flows and boxcarring (Fig. 28.1b). This combination was due to the medial posterior ciliary artery and the central retinal artery arising by a common trunk from the ophthalmic artery (Fig. 28.1c). In such a situation, when giant cell arteritis involves the common trunk, that results in involvement of both medial posterior ciliary artery and the central retinal artery. In this patient, marked narrowing of the trunk from thrombosis of the common trunk resulted in marked fall of blood pressure in both arteries, so that even a slight fall of blood pressure (e.g., in orthostatic hypotension) or rise of intraocular pressure (from stooping or even slight pressure on the eyeball) resulted in a fall of perfusion pressure, precipitating transient visual blurring.
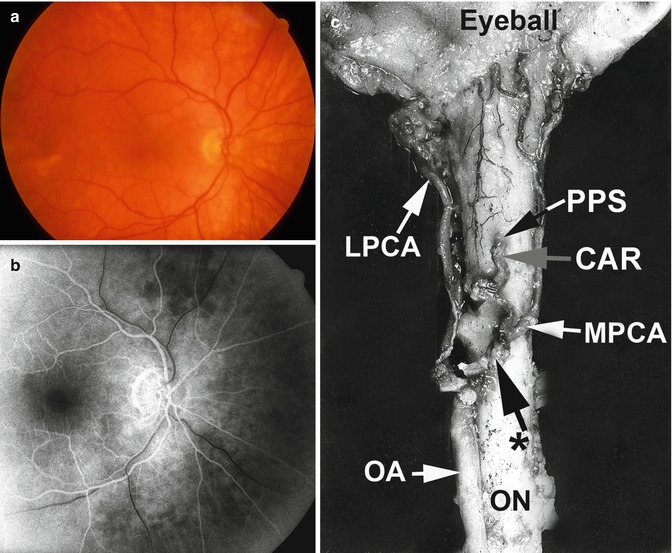
Fig. 28.1
Fundus photograph of the right eye (a) and fluorescein fundus angiogram (b) of a 74-year-old man with giant cell arteritis. (a) Normal fundus. (b) 26 s after the injection of dye, this shows marked impairment of the circulation in the medial posterior ciliary artery and with delayed retinal blood flow and boxcarring of the blood column. (c) The central retinal artery and the medial posterior ciliary artery arise by a common trunk from the ophthalmic artery, as seen from below (Reproduced from Hayreh [39]). Abbreviations: CAR central artery of the retina, LPCA lateral posterior ciliary artery, MPCA medial posterior ciliary artery, OA ophthalmic artery, ON optic nerve, PPS point of penetration into the sheath by CAR, * common trunk of origin of CAR and MPCA
The patient was immediately started on intravenous megadose corticosteroid therapy followed by high-dose oral therapy. His temporal artery biopsy was positive for giant cell arteritis. The day he was started on corticosteroid therapy, he had another episode of amaurosis fugax at 10 PM. The next day he had a couple of short episodes and another one 2 days after that, but those were not as bad as before. After that he had no more episodes. I followed him for 12 years till his death, on a small maintenance dose of 1 mg prednisone, without any ophthalmic or systemic problem.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


