Types
Subtypes
Cystic lesions
Benign
Epidermal inclusion cyst
Sebaceous cyst
Retention cyst
Trichilemmal cyst
Sweat gland tumors
Benign
Apocrine hidrocystoma
Eccrine hidrocystoma
Syringoma
Eccrine spiradenoma
Pleomorphic adenoma
Syringocystadenoma papilliferum
Eccrine acrospiroma
Eccrine cylindroma
Eccrine spiradenocylindromas
Apocrine adenomas
Malignant
Sweat gland adenocarcinoma
Mucinous sweat gland adenocarcinoma
Apocrine gland adenocarcinoma
Hair follicle tumors
Benign
Trichoepithelioma
Trichofolliculoma
Trichoadenoma
Trichilemmoma
Pilomatrixoma
Malignant
Carcinoma of hair follicles
Pilomatrix carcinoma
Sebaceous gland tumors
Benign
Sebaceous gland hyperplasia
Sebaceous gland adenoma
Nevus sebaceous of Jadassohn
Malignant
Sebaceous epithelioma
Sebaceous gland carcinoma
8.3 Clinical Findings
Benign lesions usually respect the anatomical structures and occur as slowly growing, well-confined tumors with a smooth surface. As with all malignant tumors, clinical symptoms include progressive growth, recurrence after incomplete excision, infiltrative growth, and destruction of adjacent tissue (loss of eyelashes). Ulceration and hemorrhage can be present in advanced stages. Pain is an uncommon presenting feature in this location.
8.4 Treatment, Follow-Up, and Prognosis
Management is similar in the majority of these tumors; benign lesions are excised for histologic confirmation, and malignant tumors are removed surgically with a tumor-free margin confirmed by histopathologic evaluation. Follow-up and the prognosis depend on the dignity and on the extremely rare-development of metastases. All benign and malignant tumors of the eyelids, inflammatory lesions, and metastatic lesions.
8.5 Cystic Lesions
8.5.1 Epidermal Inclusion Cysts or Epidermoid Cysts
Epidermal inclusion cysts or epidermoid cysts usually occur as smooth dome-shaped nodules of varying size, frequently revealing a punctum or pore. Occasionally, they appear pigmented. The characteristic feature is a cystic space filled with keratin, lined by regular keratinizing stratified squamous epithelium. In case of keratin extrusion after cyst rupture, a marked inflammatory reaction can develop. Milia are miniature variants of epidermal cysts. Histo-logically, comedonal cyst is similar to an epidermoid cyst in that the lining consists of keratinizing stratified squamous epithelium. Clinically, a comedonal cyst is characterized as “blackhead” (comedo with opening onto the surface) or “whitehead” (comedo with blocked opening).
A “sebaceous” cyst is a clinical misnomer, as despite the yellowish color of many cysts, histologic findings do not qualify any of these lesions as sebaceous. Clinically, the term is used most often for epidermoid or trichilemmal cyst.
8.5.2 Retention Cysts
Retention cysts can develop from all glands with the sudoriferous cyst, originating from sweat glands, as the most frequent type. The typical lining consists of a layer of nonkeratinizing glandular epithelium and a thin layer of myoepithelial cells.
8.5.3 Trichilemmal (Pilar) Cysts
Trichilemmal (pilar) cysts occur frequently in the scalp and appear as intradermal yellowish-smooth intradermal swelling. The cyst lining is composed of basophilic cells surrounded by a rim of fibrous tissue. Towards the lumen the cells develop into squamous epithelium with pale and fairly high keratocytes that abruptly turn into keratin without a granular layer. Sometimes calcification occurs, and often cholesterol clefts are seen.
8.6 Sweat Gland Tumors
8.6.1 Benign Tumors
There are two types of sweat glands: eccrine and apocrine. Eccrine sweat glands are widely distributed in the body and each gland consists of a single duct with a coiled deeper component [3]. By contrast, the apocrine sweat glands are limited to the special regions such as axilla, nipple, external ear, external genitalia, and the eyelids [3]. The apocrine glands and their ductal openings are closely associated with eyelashes [4]. Apocrine hidrocystoma and eccrine hidrocystoma represent the majority of the benign sweat gland tumors. In contrast to apocrine hidrocystoma, the eccrine hidrocystoma does not involve the eyelid margin. This is due to the fact that the eccrine sweat glands are distributed throughout the eyelid skin and are not confined to the eyelid margin unlike the apocrine glands [4].
8.6.1.1 Apocrine Hidrocystoma
Apocrine hidrocystoma (cystadenoma, apocrine tubular adenoma, cyst of Moll) is usually a solitary nodule affecting mostly the head (cheek) or neck in middle-aged people of either sex. It presents as a translucent or bluish-black nodule up to about 1 cm in diameter involving the eyelid margin (\) [5]. In rare instances, it can occur as multiple lesions [6] and can be a feature of Schopf-Schulz-Passarge syndrome [7]. Histopathology reveals an unilocular or multilocular cystic space (Fig. 8.1b) that is lined by a single or double layer of epithelial cells, surrounded by an outer layer representing myoepithelial cells, while the inner layer frequently shows the typical decapitation secretion. In some areas, epithelial proliferations can be found (Fig. 8.1c).
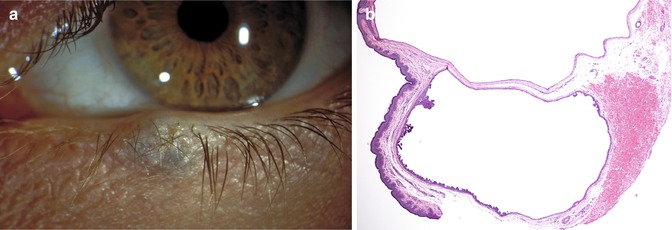
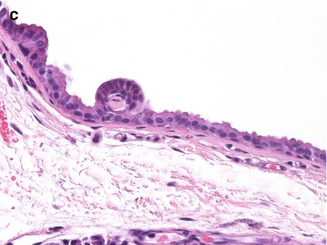
Fig. 8.1
Apocrine hidrocystoma. Note bluish color of the cystic lesion involving the eyelid margin (a). Histology shows cyst lined by a single to double layer of epithelial cells, surrounded by flattened myoepithelial cells. Proliferations of the epithelial lining are characteristic. Typical decapitation secretion is also found (b). Note focal epithelial proliferation (c)
8.6.1.2 Eccrine Hidrocystoma
A typical eccrine hidrocystoma of the eyelid manifests in an adult as a solitary clear cystic lesion (Smith and Chernosky type) [8], although cases with simultaneous bilateral involvement (Robinson type) [9] have also been reported (Fig. 8.2a). The tumor is usually located along the medial or lateral aspect of the eyelid. On average, eccrine hidrocystoma measures 4 mm in the largest dimension and it is rare for them to be larger than 10 mm [10]. Histologically, this tumor probably just represents a markedly dilated sweat gland duct with a presumably functional pathogenesis (Fig. 8.2b). Myoepithelial cells and decapitation secretion are absent (Fig. 8.2c).
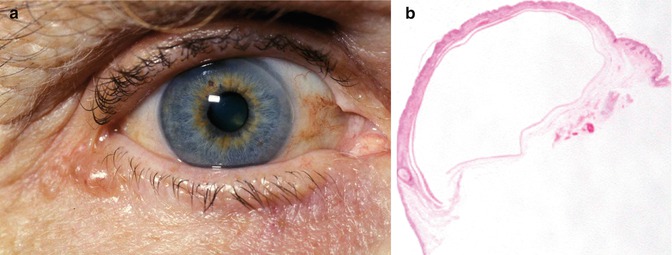
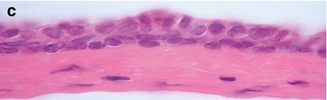
Fig. 8.2
Eccrine hidrocystoma. Note the gap between the tumor and the eyelid margin (a). There is absence of papillary projections into the cystic cavity (b). The lining cuboidal epithelium is double layered and the cells lack decapitation (c) (Reproduced with permission from Singh et al. [10])
8.6.1.3 Syringomas
Syringomas are common lesions on the upper eyelids, especially in females. They usually present as multiple small asymptomatic nodules (2–3 mm) but show a wide variety of clinical pictures (Fig. 8.3a). Histology shows interconnecting eccrine ducts and strands, lined by two layers of flattened cuboidal cells and sometimes giving rise to the characteristic tadpole configuration (Fig. 8.3b). Intracellular glycogen accumulation can cause a clear cell variant.
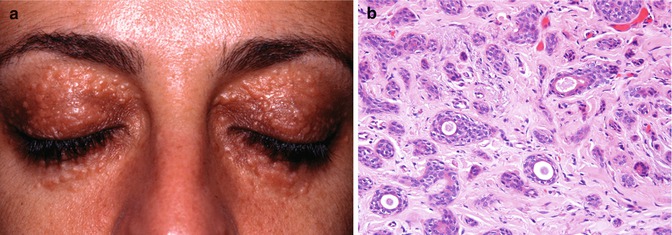
Fig. 8.3
Syringoma. Multiple bilateral syringomas of the upper and lower eyelids in a young woman (a) (Reproduced with permission from [29], Figure 9-45). The histopathology shows interconnecting eccrine ducts and stands which may present in a comma-shaped fashion (b)
8.6.1.4 Eccrine Spiradenomas
Eccrine spiradenomas are uncommon tumors presenting as a mostly tender or painful subcutaneous nodule of fairly characteristic histology. Sharply demarcated aggregations of basaloid cells without connection to the dermis are arranged in a rosette-like fashion. Two types of tumor cells can be distinguished: the more peripheral small basophilic cells with round and hyperchromatic nuclei and the more central cells with larger oval nuclei and a pale-staining eosinophilic cytoplasm. Due to a rich vascular supply, this tumor can resemble an angioma, hemangiopericytoma, or glomus tumor.
8.6.1.5 Pleomorphic Adenomas (Benign Mixed Tumor)
Pleomorphic adenomas (benign mixed tumor) usually occur in the lacrimal or salivary glands but can also occur in accessory lacrimal glands of the eyelid. This lesion presents as a slowly growing either firm or cystic subcutaneous nodule, usually solitary and asymptomatic. Histologically, it is multilobulated and composed of a mixture of epithelial glandular elements embedded in myxoid stroma [11]. The stromal component can become very prominent, sometimes exhibiting a chondroid (pseudocartilaginous) and/or hyalinized appearance [12].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


