Acute Retinal Necrosis and Progressive Outer Retinal Necrosis Syndromes
Caroline R. Baumal
Jay S. Duker
David Fischer
The herpesvirus family includes herpes simplex virus (HSV), varicella-zoster virus (VZV), cytomegalovirus (CMV), and Epstein-Barr virus (EBV). CMV produces a characteristic hemorrhagic necrotizing retinitis in immunocompromised patients. Acute retinal necrosis (ARN) and progressive outer retinal necrosis (PORN) syndrome, which have been described more recently, are two distinct variants of necrotizing herpetic retinopathy.
ACUTE RETINAL NECROSIS SYNDROME
Acute retinal necrosis is a clinical syndrome that has been associated with either HSV or VZV infection.1,2,3,4,5 Features of ARN syndrome include a vaso-occlusive angiitis of both the retinal and choroidal vessels, a necrotizing retinitis that preferentially involves the peripheral retina, and significant intraocular inflammation.6 Rhegmatogenous retinal detachment is a major late sequela.
ARN was originally described in Japan in 1971 by Urayama et al., who studied six healthy patients with acute onset of a unilateral panuveitis and retinal arteritis that resulted in widespread peripheral, confluent retinal necrosis and eventual retinal detachment.7 This entity was first reported in English medical literature in 1977 by Willerson et al., who described two patients with a bilateral necrotizing vaso-occlusive retinitis.8 The term acute retinal necrosis (ARN; or BARN, when bilateral), was coined by Young and Bird in 1978.9 Although this syndrome was initially described in healthy patients, it subsequently has also been reported to occur in individuals with compromised systemic immunity—most notably in those with human immunodeficiency virus (HIV) infection.
ARN can be a visually devastating disease with a poor visual prognosis, although advances in antiviral therapy and vitreoretinal techniques for retinal detachment have improved visual outcomes. Prompt diagnosis and treatment are necessary to limit retinal damage and preserve vision.
Clinical Presentation
Acute retinal necrosis does not appear to have any racial predilection; however, it may be more common in males. Although ARN typically affects individuals between 20 and 50 years of age, cases have been reported in patients as young as 4 years and as old as 89 years of age.10,11,12,13
Initially, patients may complain of mild to moderate ocular or periorbital pain, often accompanied by a red eye. Early visual symptoms may or may not be present and can be insidious. When symptoms are present, these usually consist of floaters, blurred vision, or rarely, decreased peripheral vision. Acute central visual loss is an atypical presentation because the posterior pole usually is spared from the retinopathy until later in the course of the disease. Optic nerve involvement, retinal artery occlusion, and retinal detachment can occur and affect central vision although these are less commonly noted at presentation.7,8,9,10,14,15
External examination may reveal diffuse episcleritis, scleritis, or orbital inflammatory disease. Atypical presentation of ARN with severe inflammatory orbitopathy, proptosis, and optic nerve involvement has been reported.16 Mild to moderate anterior segment cellular reaction is common, and either granulomatous or fine keratic precipitates typically are present10,17 (Fig. 1). A hypopyon typically does not develop.8 The intraocular pressure may be low, even in the absence of retinal detachment; however, elevated intraocular pressure secondary to anterior segment inflammation also may occur. Concurrent herpesvirus infection of the cornea with dendritic or stromal keratitis is not a typical feature of ARN syndrome in healthy individuals, although it has been described in individuals with HIV infection.18,19 One case of simultaneous HSV type 1 keratitis and ARN was reported in a patient with Ramsay Hunt syndrome.20,21
 Fig. 1. Typical anterior segment appearance during active ARN syndrome. Anterior segment cellular reaction with keratic precipitates and episcleral injection are noted. |
ARN is characterized by a retinal vasculitis affecting both the arteries and veins in the fundus and is manifested by sheathing of the larger vessels (Fig. 2).7,8,9,10 Initially, patchy areas of peripheral retinal whitening (“thumbprint lesions”) representing full-thickness retinal necrosis are present or develop shortly after the vasculitis (Fig. 3). During a course that may span days or weeks, these patches coalesce into geographic areas (Fig. 4A). The entire peripheral retina (360°) may be involved, or, more commonly, there are several noncontiguous patches of necrosis, each covering from a half to three clock hours (Figs. 5 and 6). The lesions may not be detected without examination of the peripheral retina.
 Fig. 2. Fundus photograph of the posterior pole in active ARN syndrome showing prominent arterial sheathing and mild blurring of the optic disc margin. |
 Fig. 3. In early ARN, multifocal white patches of retinal necrosis occur in the peripheral retina. |
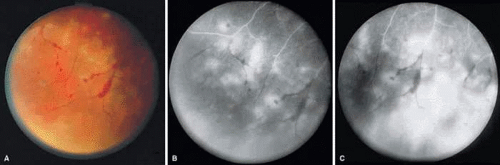 Fig. 4. A: With progression of ARN, the areas of retinal whitening begin to coalesce. Mild perivascular retinal hemorrhages are noted. B: Fluorescein angiography in the venous phase reveals retinal vascular nonperfusion in areas of active retinitis. C: In the late-phase angiogram, fluorescein hyperfluorescence is seen in areas of retinitis and around the retinal vasculature. |
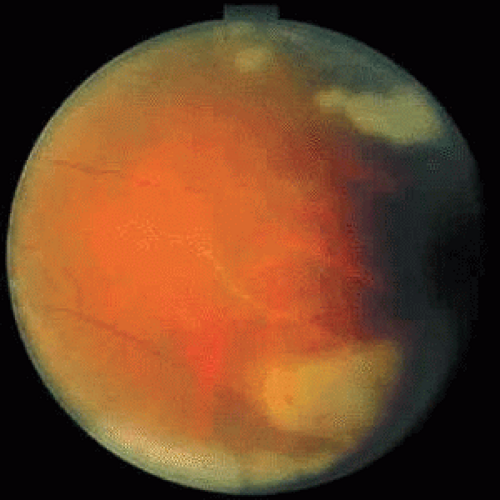 Fig. 5. The peripheral retinal whitening becomes confluent with vascular obliteration. |
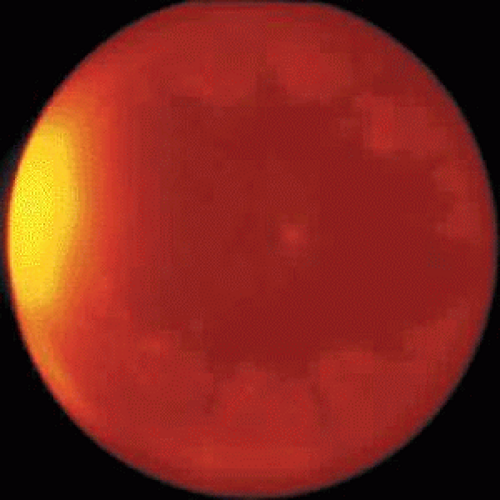 Fig. 6. Equator-plus photograph of a patient with 360° ARN syndrome. |
As the infection progresses, the leading edge of confluent retinal whitening advances toward the posterior pole (Fig. 7A). In some cases, the retinitis may not progress posterior to the vascular arcades, sparing the macula and central vision. It is hypothesized that the retinal necrosis in ARN results from the combined effect of intracellular viral replication with subsequent cell death and vascular occlusion secondary to acute vasculitis. In some patients, the retinal vasculitis component may be much more prominent than the retinal necrosis.7 Optic disc swelling, either hyperemic or pallid, is a common feature of the ARN syndrome.1 Perivascular hemorrhages may be present (Fig. 8); however, widespread areas of retinal hemorrhage are atypical. Retinal vascular occlusion, often involving the arteries, can occur at any point during the clinical course. Without treatment, the inflammatory component of ARN typically burns out in 6 to 12 weeks, leaving behind a thin atrophic retina with associated pigmentary changes.10
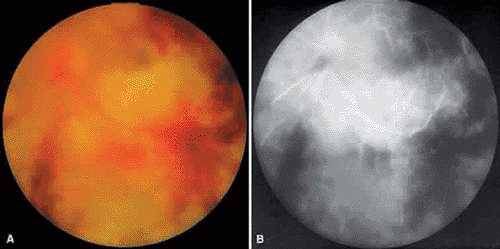 Fig. 7. A: Active ARN with diffuse retinal necrosis progressing into the macula and areas of retinal hemorrhage. The hazy view is secondary to vitreous inflammation. B: Fluorescein angiogram in the venous phase of active ARN syndrome in this eye reveals peripheral vascular nonperfusion, as well as optic nerve and perivascular hyperfluorescence. |
 Fig. 8. Perivascular hemorrhage and optic nerve head swelling with small foci of retinal necrosis inferior to the optic nerve. |
Along with anterior uveitis, a mild to moderate vitreitis is present early in the course of ARN (Fig. 9). As the retina becomes necrotic, increasing amounts of vitreous cells and debris are seen. The vitreitis may impair visualization of the posterior segment. Eventual opacification and organization of the vitreous can occur. Severe vitreous fibrosis with traction resembling proliferative vitreoretinopathy is not an uncommon late complication.1,8,9,10,11,12,14,15,17 Other features described in ARN include exudative retinal detachment, macular edema, glaucoma, and cataract.4
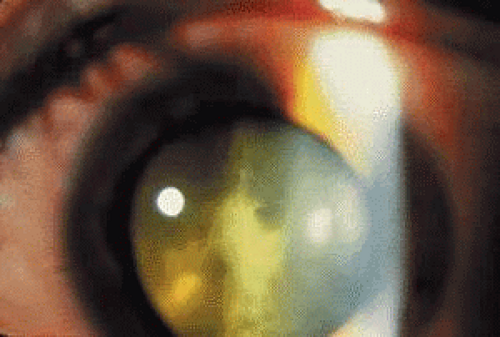 Fig. 9. Prominent vitreous reaction and a mild cataract are noted in ARN. |
As the active retinal inflammatory process recedes, either spontaneously or with treatment, the retinal areas previously infected appear thinned and atrophic, with underlying retinal pigment epithelial alterations (Fig. 10). These pigmentary changes usually begin to develop around 4 weeks after the onset of the infection.22 Often a distinct scalloped pattern can be seen that clearly demarcates previously involved and spared retina (Fig. 11). The pigmentary alterations result from both retinal pigment epithelial (RPE) cell death by direct infection and secondary inflammatory changes and hyperplasia induced by the adjacent retinal necrosis. Full-thickness retinal breaks are a prominent feature of ARN syndrome and often develop during the recovery stage of ARN. Retinal breaks may be large, irregular, and multiple and classically occur at the junction of normal and affected retina (Fig. 12).23 However, breaks can occur elsewhere in the retina, with or without accompanying vitreous fibrosis and traction. Clarkson et al. noted traction-associated retinal tears in uninvolved retina.14 Rhegmatogenous retinal detachment is a major cause of visual loss and occurs in 50% to 75% of cases not treated with prophylactic laser photocoagulation.1,10,14 Retinal detachment caused by ARN usually develops several weeks after the onset of inflammation; however, retinal detachment has been reported as early as 6 days or as late as several months after the onset of symptoms.24 These detachments are often complicated because of the combined effect of vitreous organization and multifocal retinal breaks. Unusual late sequelae of ARN syndrome include neovascularization of the retina and optic disc with vitreous hemorrhage (Fig. 13).25,26 In contrast to other uveitic syndromes, chronic or relapsing episodes of intraocular inflammation are not common in ARN.27
 Fig. 10. Healed phase of ARN syndrome in same eye as in Figure 2 after 4 weeks shows optic atrophy with retinal pigment epithelial changes. |
 Fig. 11. Venous phase of fluorescein angiogram demonstrating the healed stage of ARN syndrome. Classic retinal pigment epithelial alterations in a scalloped pattern clearly separate previously involved retina from spared retina. |
 Fig. 12. Complicated retinal detachment secondary to multiple, posterior retinal holes and PVR associated with ARN syndrome. Despite pars plana vitrectomy with silicon oil injection, the retina could not be reattached. This photograph was taken 6 weeks after Figure 10. |
 Fig. 13. Peripheral retinal neovascularization may occur on occasion as a sequela of ARN syndrome. |
In the absence of direct macular involvement, arterial obstruction, or retinal detachment, decreased central vision that is inconsistent with the associated retinal findings is most likely secondary to optic nerve involvement.28 The presence of optic disc swelling with ARN was noted by early investigators.10 Histopathologic studies have confirmed the presence of intraneural inflammation and necrosis.1,29,30,31 Both direct inflammation of the optic nerve substance and a secondary ischemic component are believed to produce ARN optic neuropathy, paralleling the pattern of visual dysfunction in the retina. When optic nerve involvement occurs in ARN, an acquired dyschromatopsia, a relative afferent pupillary defect in disproportion to the amount of retinal necrosis, central or arcuate visual field defects, and an enlarged optic nerve sheath can be detected with neuroimaging (Fig. 14).28,31 It often is difficult to distinguish whether visual loss is caused by optic neuropathy or retinal disease in these severely affected patients. An accurate assessment of the incidence of ARN optic neuropathy has not been made. Clinically, optic nerve swelling occurs in a significant number of patients with ARN and may resolve rapidly with therapy.
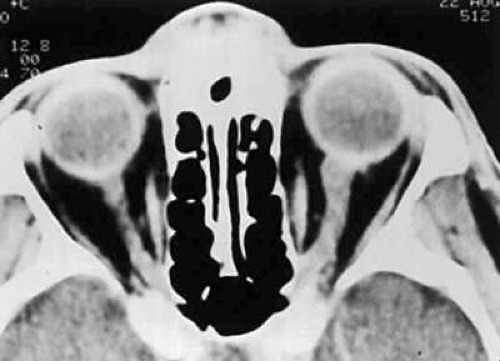 Fig. 14. Computed tomography scan of a patient with unilateral ARN syndrome showing enlarged left optic nerve ipsilateral to the affected eye. (From Sergott RC, Belmont JB, Savino PJ et al: Optic nerve involvement in the acute retinal necrosis syndrome. Arch Ophthalmol 103:116, 1985, with permission from the American Medical Association.) |
Bilateral involvement in ARN eventually occurs in up to 65% of patients.10,23 There is no correlation between the severity of ARN in the first eye and severity of the disease in the fellow eye. Involvement of the second eye may not be apparent initially; there may be a delay of several weeks. Thirty-four years is the longest reported interval for involvement of the contralateral eye in ARN.32 Although this is an atypical scenario, it emphasizes the need for long-term ophthalmologic examinations in patients with ARN.
Initial reports indicated that the long-term visual prognosis in ARN syndrome was poor; 60% of eyes had a final visual acuity of 20/200 or worse.10,31 Potential causes of visual loss in ARN syndrome include the following:
Media opacity
Retinal cell necrosis, infection, ischemia, retinal detachment, macular pucker
Optic neuropathy
A modified classification of the stages of ARN syndrome is presented in Table 1. However, not all cases of ARN have a fulminant course and result in a poor outcome. Mild cases of ARN with limited peripheral retinitis and good visual outcomes have been reported, and some cases rarely resolve spontaneously without treatment.33 In a recent study of eyes with limited retinal involvement at the time of diagnosis, final visual acuity was 20/40 or better in 50% and 20/400 or better in 92% of eyes after treatment with acyclovir and prophylactic laser photocoagulation.34 The growing number of ARN cases with a good visual outcome is likely owing to increased physician awareness of this disorder, which leads to earlier diagnosis and aggressive therapy. The features of ARN may vary in severity depending on the specific etiologic agent and the immune status of the individual. For example, ARN associated with primary VZV infection (chickenpox) may have less severe features and a better visual prognosis.35
TABLE 1. Stages of ARN | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
Central nervous system abnormalities occasionally have been associated with ARN syndrome. Cerebrospinal fluid pleocytosis is well documented.10,28,36 One case of labyrinthine deafness in association with diffuse cerebral atrophy has occurred.37 True viral encephalitis usually is not concomitant with ARN syndrome; however, posterior segment inflammatory conditions that resemble ARN have been reported in association with florid viral encephalitis.38,39 A rapidly progressive, bilateral retinal necrosis caused by HSV has been described in two patients with concomitant HSV encephalitis and acquired immunodeficiency syndrome (AIDS).5 Due to the potential findings of central nervous system abnormalities and ARN optic neuropathy, it has been suggested that ARN be reclassified as a “uveo-meningeal syndrome” instead of an isolated retinitis.28
Initial reports of ARN were in healthy patients with normal systemic immunity who lacked extraocular manifestations of herpetic infection. This continues to be true in most ARN cases. Most cases of ARN are believed to be secondary to reactivation of a latent herpetic infection, and often patients have a prior history of dermatomal VZV (herpes zoster) or primary VZV (chickenpox) infection, or perioral blisters, presumably caused by HSV infection. Reactivation of the viral genome from the trigeminal ganglion may result in the development of ARN after transneural spread. Trauma-induced reactivation of latent congenital HSV type 2 infection has been reported in ARN.13 ARN secondary to VZV was reported following ocular contusion in a patient initially treated with corticosteroids and vasoactive drugs for presumed ocular ischemic syndrome. It was hypothesized that ocular trauma may have induced and corticosteroid treatment promoted reactivation of this latent viral infection.40 It is uncommon for healthy individuals to develop ARN simultaneously with cutaneous VZV or HSV infection.41 Concurrent aphthous ulcers have been reported in two patients with ARN.42 Rare cases of ARN have been described in immunocompetent individuals (primarily adults) with primary VZV infection and in those who have had close contact with an individual with chickenpox but who did not experience skin lesions.35,43
The clinical features of 11 cases of HSV-2 related ARN were retrospectively reviewed. HSV-2 DNA was detected by polymerase chain reaction in intraocular fluids (aqueous and/or vitreous), and no sample was positive for more than one virus. All patients were immunocompetent, ranging in age from 10 to 57 years (mean 36 years). Past medical history revealed neonatal herpes (n = 1), previous ARN (n = 3), trauma (n = 1), and systemic corticosteroids prior to developing ARN (n = 3). As well, pre-existing chorioretinal scars were noted in three cases. The further support that HSV-2 retinitis may result from reactivation of HSV-2 infection.44
ARN subsequently has been reported in immunocompromised patients with HIV infection, autoimmune disorders, cancer, and organ transplants.45,46,47 It has been recommended that ARN syndrome be defined by its ocular features rather than by the immune status of the affected individual.4 In patients with HIV infection and ARN, the CD4+ T-lymphocyte count generally is greater than 60 cells/μL, although ARN is sufficiently infrequent in these patients to allow any conclusions to be drawn regarding the CD4+ count. HIV-infected patients are more likely to have simultaneous or recurrent VZV or HSV infections. Bilateral ARN after unilateral herpes zoster ophthalmicus has been reported as a presenting sign of AIDS. In a study of patients with VZV involving the ophthalmic division of the trigeminal nerve, 5 of 29 (17%) patients with HIV infection developed ARN within 9 months of follow-up, but there were no cases of ARN in immunocompetent individuals.47 ARN syndrome associated with HIV infection is typical in that it is rapidly progressive, peripheral in location, and responsive to acyclovir treatment. However, the retinitis often is more severe and bilateral and often results in a worse visual outcome than in immunocompetent individuals.5,47
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


