Acute Proptosis in Adults
David R. Jordan
Louise Mawn
Bernard Hurley
Proptosis that occurs over several minutes, several hours, or 1 to 2 days is considered acute. When the onset is over a period of weeks, proptosis is considered subacute, and proptosis with a more insidious onset over several months is defined as chronic. The globe can shift forward acutely with the accumulation of blood, air, infectious or inflammatory material, mass effects secondary to tumor, structural changes (orbital fractures, spontaneous globe luxation, etc.), or with a variety of other traumatic events.
This chapter highlights the clinical features of several common as well as uncommon disease processes that may cause acute proptosis in adults and provides a framework for diagnosis and management.
PATIENT EVALUATION
Evaluation of the patient with acute proptosis is similar to that performed for any orbital disease. The goal is to establish a diagnosis based on a thorough history and physical examination.This clinical analysis sets the stage for further investigations and is a valuable tool.1 There are several basic patterns of disease presentation that provide a framework for the study of each case. The history should elicit the following information: rapidity of onset, progression (intermittent or gradually progressive), accompanying symptoms (pain, diplopia, loss of vision), duration of symptoms, current medications, past disease (thyroid, sinus), trauma history, current or past systemic disease (cancer history), and family history. The temporal sequence of events preceeding the acute proptosis may act as a clue to the responsible disease process. Evidence of a temporal variation such as diurnal fluctuation or relapsing and remitting symptoms in the days, weeks, or months prior to presentation may be extracted from the patient’s history. The rapidity of development of acute proptosis is also important. A catastrophic change occurring over a matter of minutes suggests a vascular event (e.g., a high-flow carotid-cavernous sinus fistula), hemorrhage into a preexisting lesion (e.g., lymphangioma) or air accumulation (e.g., after a nose blow or sneeze in patient with an orbital fracture). A change that is somewhat less rapid, occurring over several hours or 1 to 2 days, but progressive, suggests an inflammatory or infectious process. An intermittent nature of the proptosis, pulsation, or alteration with a Valsalva maneuver in the weeks or months prior to the acute event suggests either a bony defect in the orbit or a vascular lesion such as an orbital varix. It is important to determine where the disease process is located and how the process has affected the orbital structures.1 When a process shifts the orbital structures, the direction of shift may be a clue to the location of the disease. The effect can be viewed as positive if the lesion occupies space and pushes orbital structures away, negative if it draws structures toward, or both. The physical examination should provide information about the degree and direction of displacement of the affected orbital structures.1
The patterns of orbital involvement with various disease processes can be divided into four basic clinically discernable categories. These are not necessarily independent but provide a working framework for characterization of the orbital problem1:
Inflammatory effect: inflammation may be either infectious or noninfectious in nature and is associated with signs and symptoms of redness, swelling, pain, heat, and loss of function. There is often a mass effect present.
Mass effect: displacement with or without signs of involvement of sensory or neuromuscular structure. Displacement points to the location of the diseases and may help to characterize its nature.
Vascular change: features suggesting vascular disease include venous dilation, pulsation, expansion with straining (Valsalva), and hemorrhage.
Infiltrative change: infiltrative diseases are usually associated with evidence of destruction, entrapment, or both. These include effects on ocular movement or neurosensory function (e.g., optic neuropathy, pain, or paresthesia).
The history and physical examination should allow the clinician to discern whether the disease process is characterized by features of inflammation (infective or non-infective), mass effect, vascular change or infiltrative effect as well as the location of the disorder. Subsequent investigations are used to confirm clinical suspicion about the disease process and may include visual function assessment (e.g., color vision, visual fields), orbital imaging (computed tomography, magnetic resonance imaging, echography, arteriography, venography), systemic survey (complete blood cell count, white blood cell count, erythrocyte sedimentation rate, thyrotropin, etc.) and pathologic study (cytology, immunohistochemistry, electron microscopy, etc.) of a biopsy specimen. In the final analysis it is generally a combination of the historical features, clinical presentation, and investigative results that confirms a diagnosis and leads to the rationale management of the process affecting the orbit.
ORBITAL INFECTIONS
ORBITAL CELLULITIS
Orbital cellulitis is the model for acute inflammation and a major cause of orbital inflammation in adults.2 It is characterized by a rapid development (over 1 to 2 days) of inflammatory signs and symptoms. These include: eyelid swelling, redness, warmth, pain, conjunctival injection, chemosis, proptosis, and mobility impairment with or without reduced vision. These patients generally feel unwell (malaise) and are febrile (Fig. 1A and 1B). The malaise and fever are key features in differentiating cellulitis from a rapid-onset nonspecific orbital inflammation (pseudotumor) and should be obtained from the patient’s history.
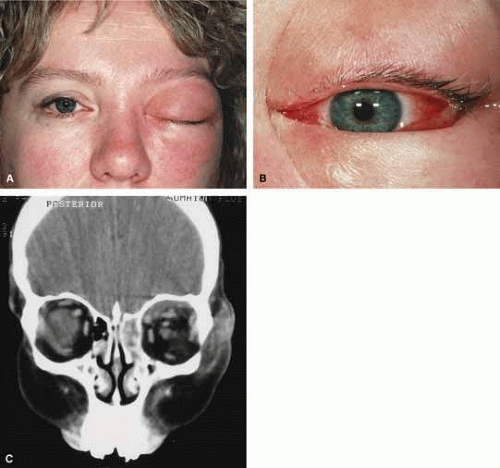 Fig. 1 A. A 25-year-old patient presented with proptosis, lid swelling, conjunctival chemosis/injection, pain, malaise, and fever. B. Conjunctival chemosis. C. Ethmoid sinus opacification is present with a superior subperiosteal abscess. |
The majority of orbital cellulitis is secondary to extension from an adjacent sinus infection (Fig. 1C). Organisms gain access to the orbit directly through the thin ethmoidal bone, through congenital or acquired dehiscences in the thin orbital walls, pass through preexisting orbital foramina, pass retrogradely through the valveless venous orbital system, or along the veins as a periphlebitis. Orbital cellulitis may also be secondary to an endophthalmitis, systemic bacteremia (e.g., after dental work), infection of a nearby skin wound, dacryocystitis, or penetrating trauma.
The history and physical examination are crucial in distinguishing between preseptal and true orbital cellulitis. The orbital septum delineates the anterior eyelid soft tissue from the orbital soft tissue. Infections anterior to the septum are classified as preseptal cellulitis while those posterior to the septum are termed orbital cellulitis. Recognition of true orbital involvement is important not only because of the threatened visual loss associated with the orbital involvement but also because of the potential for central nervous system complications including cavernous sinus thrombosis, meningitis, and death.
Preseptal cellulitis is characterized by lid edema, erythma, and discomfort. Inflammation posterior to the orbital septum (orbital cellulitis) is heralded by the development of pain, chemosis, proptosis, motility disturbance, and visual deterioration. The extent of ocular involvement in preseptal and orbital cellulitis can be determined by assessing visual acuity, extraocular motility, pupillary reaction, color vision, confrontation visual fields, intraocular pressure, and optic nerve head appearance. Evidence of facial/head trauma or surgical wounds may be apparent. Constitutional signs such as fever, lethargy, and irritability should be sought. The examiner should assess for meningeal signs and neurologic defects. After the initial examination, the physician should follow patients with orbital cellulitis with at least daily assessments of visual acuity, motility, and pupil reaction.
Progression of the disease process despite appropriate antibiotic therapy suggests abscess formation. Orbital abscesses may be either localized, diffuse, or subperiosteal (Fig. 1C). Subperiosteal abscesses most commonly occur along the medial wall and may expand rapidly, compromising optic nerve function even in the absence of many signs of infection.3,4,5,6 Several mechanisms may contribute to visual deterioration including direct optic nerve compression, elevation of the intraorbital pressure, and proptosis causing a “stretch” optic neuropathy. Clinically, the eye typically is displaced away from the subperiosteal abscess, and orbital imaging shows a convex mass adjacent to the involved sinus.
Orbital infection with potential orbital abscess formation occurs when bacteria break through the periorbita and gain access to the extraoconal or intraconal space. Diffuse or localized orbital abscess formation may also lead to visual loss through an increase in intraorbital pressure, posterior ischemic optic neuropathy, optic nerve inflammation, or vasculitis. Acute visual loss in the presence of an orbital infection is almost always a surgical emergency in which immediate drainage of the abscess is required to save vision. Continued posterior extension of the infection may result in an orbital apex syndrome, decreased function of cranial nerves,2,3,4,5,6 thrombosis of the cavernous sinus, and even death. Hallmarks of cavernous sinus thrombosis include cranial neuropathy and central neurologic impairment.7
Organisms responsible for orbital cellulitis vary widely and may include Staphylococcous aureus, Streptococcus species, as well as a mixture of aerobes and anaerobic organisms. Recent studies indicate that streptococcus is the most common cause of orbital cellulitis associated with sinusitis in children.8 With increasing age the pathogens increase in complexity. In patients older than 15 with subperiosteal abscesses, polymicrobial infections are typical with anaerobes cultured in every case.5
Orbital imaging in the axial and coronal plane should be obtained in all patients suspected of having orbital cellulitis. Computed tomography (CT) is preferred to magnetic resonance imaging (MRI) because the orbital tissues have higher contrast and bone is well visualized. Axial CT views allow evaluation of the medial orbit and ethmoid sinuses, whereas coronal scans image the orbital roof, floor, frontal, and maxillary sinus. A subperiosteal abscess appears as a homogeneous opacification between the orbital wall and the displaced periorbita.6 Contrast agents are not necessary to visualize a subperiosteal abscess.
Management of orbital cellulitis is dictated by the rapidity of onset. Oral antibiotics may be appropriate for mild cases whereas intravenous antibiotics are required for more fulminant cases. Antibiotic coverage should be broad spectrum and include coverage for gram-positive organisms and anaerobes. Examples include cloxicillan and clindamycin or a late-generation cephalosporin and clindamycin. In those patients allergic to penicillin agents, erythromycin and clindamycin or vancomycin and clindamycin are considerations.
Most patients with orbital cellulitis also benefit from a nasal decongestant as well as an oral decongestant and warm compresses to the affected site (10 minutes out of every hour). Daily or more frequent reexaminations are required depending on the fulminancy of the disease. Once antibiotics are initiated, a 24-hour wait-and-watch period is generally observed (unless the process is aggressive and rapidly developing). If there is no progression at 24 hours and the vision is stable, continued observation is appropriate. If the orbital cellulitis is rapidly developing and fulminant, frequent assessments (every 2 to 4 hours) are required. If the vision, motility, or neurologic status is deteriorating, immediate surgical intervention may be required.
The indication for surgery in a patient with orbital cellulitis has been controversial over the years. The simple presence of a subperiosteal abscess (SPA) was at one time an indication to drain but this is no longer always the case. Providing the vision is normal, the SPA may resolve with medical management. The clinical course, and not the radiographic appearance should dictate management.5,6,9 Surgical therapy may be influenced by many factors including the visual status, size, and location of the SPA; intracranial complications; the sinus involved; the presumed pathogenesis, and the anticipated bacterial response to antibiotic treatment.10 Immediate drainage of SPAs and sinuses is recommended for patients of any age whose vision is compromised. Urgent drainage (as soon as practical) should be considered for large SPAs, extensive superior or inferior abscesses, intracranial complications at the time of presentation, frontal sinusitis where the risk of intracranial extension is increased, and in those suspected of having anaerobes (postdental procedures). However, cookbook approaches should never take the place of good clinical judgement and therapeutic decisions regarding early drainage versus medical management with observation are ultimately up to the managing physician.10 Older children (older than 9 years of age) and adults benefit from early surgical drainage. Although surgical treatment does not guarantee rapid resolution, a complicated course is more likely without it.10
Abscesses may also develop within the intraconal space. The prescence of an abscess within the orbital tissue coupled with any signs of visual loss, afferent pupillary defect, or a significant motility defect should prompt emergent surgery. If visual acuity is stable and extraocular motility essentially full, initial treatment may consist of empiric antibiotic therapy and close observation with serial CT scans.
The prescence of neurologic symptoms such as altered mental status or seizures implies intracranial extension with potential intracranial abscess. Infection may spread from the sinuses to the intracranial cavity via retrograde thrombophlebitis, directly through osteitic bone or from congenital or acquired bony defects. In the past, intracranial abscess formation had a poor prognosis with a high mortality rate. Successful management of suppurative abscesses requires early recognition of the disease process, intravenous antibiotics, serial neuroimaging, and surgical management of at least the orbit and sinus disease and often the intracranial disease.11
PHYCOMYCOSIS (RHINO-ORBITAL MUCORMYCOSIS AND ORBITAL ASPERGILLOSIS)
Rhino-orbital mucormycosis, a fungal infection of class Phycomycetes and order mucorales, is notable for its high morbidity and mortality.12,13 Orbital involvement is an acute, aggressive, and often lethal infection if not recognized early. Phycomycetes (common bread molds) are ubiquitous fungi occurring in soil, air, skin, body orifices, manure, and food including fruit.13 Inoculation occurs by inhalation reaching the nasopharynx and oropharynx. At this stage most patients are able to contain the disease. However, individuals whose cellular and humoral defense mechanisms have been compromised by disease or immunosuppressive treatment may not be able to generate an adequate response. The fungus may then spread to the paranasal sinus, orbit, meninges, and brain by direct extension.13 Mucormycosis preferentially involves blood vessel walls resulting in vascular occlusion, thrombosis, and infarction.14 This frequently affects the ophthalmic artery and in more serious cases may involve the internal carotid artery and cavernous sinus.
Although there have been a few reports of mucormycosis occurring in healthy individuals, virtually all other patients have had previous severe underlying disease. The patient most vulnerable to this infection is an one with uncontrolled diabetes with ketoacidosis. A host of other conditions also predispose patients to the disease including: multiple myeloma, lymphoma, organ transplantation with immunosuppresion, chemotherapy, corticosteroid treatment, acquired immunodeficiency syndrome, etc.(Fig. 2A).12,13,14 Mortality is extremely high for patients with phycomycosis infection, and successful treatment is contingent on early recognition and prompt treatment.
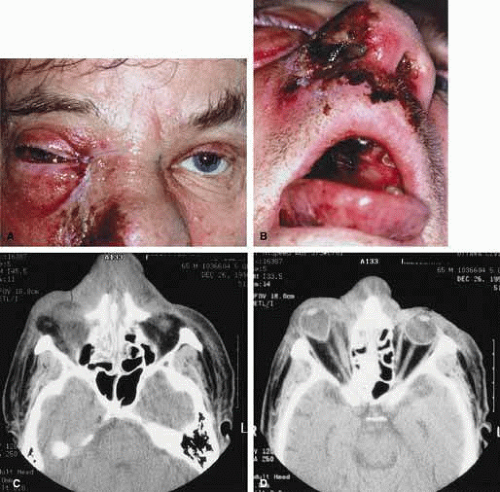 Fig. 2 A. A 65-year-old man with a myelodysplastic disorder and pancytopenia developed a pimple on the side of his nose followed by rapidly developing cellulitis and skin necrosis. The patient developed a frozen globe and loss of vision over a matter hours. Despite aggressive surgical debridement of the necrotic areas and intravenous, amphotericin, the patient died. B. Black eschar (necrosis) along right side of nose, ala, upper lip, and hard palate. C. Right orbital infiltration is seen along with opacification of the right ethmoid sinus and nasal passage. D. The optic nerve is on stretch with tethering of the globe, extensive soft tissue swelling anteriorly, ethmoidal opacification, and enlargement of the right medial rectus muscle. |
A characteristic pattern of clinical symptoms and signs occurs, the recognition of which should lead to the immediate institution of antifungal treatment and possible surgical intervention to increase the patient’s chances of survival. Early diagnosis while the disease is still somewhat anatomically confined is essential for a more favorable outcome.12,13,14
Characteristic features of orbital mucormycosis include an immunocompromised patient with sinusitis, pharyngitis or nasal discharge who develops cellulitis of the face or lid. Signs and symptoms include orbital/periorbital pain, acute proptosis, abrupt visual loss, orbital apex syndrome with acute motility changes (external ophthalmoplegia), pupillary changes (internal ophthalmoplegia), ptosis, and decreased corneal sensation. Infarction of tissue results in black eschar formation of the skin, nasal mucosa and hard palate (Fig. 2A and 2B).12,13 With intracranial extension, the patient generally become obtunded, develops convulsions, contralateral hemianaesthesia or hemiplegia, and lapses into coma.
CT scanning demonstrates an orbital mass often with bone destruction and sinus involvement (Fig. 2C and 2D). The diagnosis is confirmed by biopsy of involved tissue with demonstration of characteristic nonseptate, large, branching hyphae, which can be seen on routine hematoxylin and eosin stains. Material should be submitted for both frozen and conventional paraffin-embedded sections. Frozen sections are not always definitive and the surgeon must have considerable confidence in the skill of the pathologist.13 Management includes: (1) early definitive diagnosis; (2) correction of any underlying metabolic disturbance; (3) wide local excision with debridement of all involved and devitalized oral, nasal, sinus and orbital tissue; (4) establishment of adequate sinus and orbital drainage; (5) daily irrigation and packing of the involved orbital and paranasal areas with amphotericin B; and (6) intravenous amphotericin B.12,13,15
The extent of surgical excision should balance the degree of morbidity and mutilation against the life-threatening risk this organism represents. In limited cases, surgical excision may be confined to those tissues clearly infarcted. Should infection be extensive as demonstrated by widespread necrosis, then aggressive surgery, including exenteration of the orbit and any involved paranasal sinuses, may prove necessary and lifesaving.13
ORBITAL ASPERGILLOSIS
Aspergillus, a fungus of the Ascomycetes class, is a common environmental organism that may colonize the aerodigestive tract. Although widespread, the fungus has a low intrinsic virulence and clinically apparent aspergillosis is rare in the immunocompetant host. Invasive aspergillosis, similar to mucormycosis, occurs more often in the immunocompromised host, including patients undergoing transplantation or steroid therapy, neutropenic patients undergoing chemotherapy, alcoholics, patients with diabetes, and patients with acquired immune deficiency syndrome (AIDS).16,17,18,19,20 Orbital involvement may be slowly progressive or abrupt in onset with orbital inflammation, proptosis, pain, ophthalmoplegia, and sudden loss of vision.16,19 Fulminant aspergillus infection of the nose, paranasal sinus, and orbit often associated with intracranial extension has been reported with increasing frequency in immunocompromised individuals.17,18 In these patients, local invasion of the sinus mucoperiosteum produces a rapidly progressive gangrenous necrosis.18 With bone destruction, infection may extend into the orbit and intracranial cavity; the latter has a poor prognosis. The fungus may also spread by hematogenous routes.17 Imaging studies reveal sinus involvement, heterogenous soft tissue masses with bony erosion, and calcification.16 A definitive diagnosis of aspergillosis is based on tissue biopsy and fungal cultures.
Treatment of invasive sino-orbital aspergillosis involves aggressive surgical debridement combined with a systemic antifungal agent. Intravenous amphoticin B has been the mainstay of medical therapy but toxic side effects, especially renal, require discontinuing the medication in some patients. Newer systemic antifungal agents include liposomal amphotericin B (fewer renal toxic effects) and oral intraconazole.21,22,23,24 Adjuvant local irrigation of amphotencin B has also been recommended.24 For patients unable or unwilling to undergo surgery, intralesional injection of amphotericin B has been used successfully as palliative treatment.25 Despite aggressive therapy, the mortality in those with invasive sino-orbital aspergillosis remains high.17
INFLAMMATORY DISEASE OF THE ORBIT: (NONINFECTIVE, NONTHYROID)
Orbital inflammatory processes can be viewed as either nonspecific or specific.26 The nonspecific orbital inflammatory diseases were previously known as inflammatory orbital pseudotumor. The frequency of diagnosis of nonspecific orbital inflammation appears to be decreasing as we improve our understanding of the various types of clinical specific orbital inflammation.26
The definition of nonspecific inflammation remains clinical and consists of processes that are acute and subacute and have characteristic anatomic localization within the orbit. Although the exact mechanism of the inflammation is unknown, an immunologic disorder of some sort is most likely the cause.26,27 Histopathologically, the spectrum of disease is characterized by a nonspecific polymorphous infiltrate of inflammatory cells.26,27 In contrast to nonspecific inflammations, specific inflammations represents three possible types of processes:
Those identified on the basis of a specific pathogen (i.e., infections) and infestations (e.g., orbital cellulitis).
Those that have specific local and/or systemic constellations of findings that identify them as distinct, e.g., Wegener’s granulomatosis.
Those diseases that have a specific histopathology that identifies them such as some of the granulomatous diseases, e.g., sarcoidosis.
This section examines the nonspecific orbital inflammations (noninfective and nonthyroid) as well as some of the specific types of inflammations (vasculitis, collagen vascular disorders).
NONSPECIFIC INFLAMMATION OF THE ORBIT
The common feature of nonspecific inflammation of the orbit (previously known as orbital pseudotumor) is the acute or subacute presentation of orbital inflammation. The etiology undetermined. There are several clinical categories of disease, defined by the location of the inflammation. The nonspecific inflammatory syndromes can be divided into a myositic, lacrimal, anterior, diffuse or apical pattern. Imaging reveals an irregular margin adjacent to the primary focus of disease with evidence of tissue swelling and contrast enhancement. Each pattern may present acutely over 24 to 48 hours with orbital pain, tenderness, lid swelling, conjunctival injection, chemosis, proptosis, and decreased extraocular motility. In contrast to patients with orbital cellulitis, these patients are afebrile and do not have malaise. Myositis is the most common pattern of presentation. Patients are usually young (mid 30s) but the age of presentation may range from 9 to 84 years.27 They characteristically present with the acute onset of periorbital pain aggravated by extraocular movement. Signs include eyelid edema, redness, chemosis, conjunctival injection, and motility restriction (Fig. 3A and 3B). The areas over the involved muscles are generally tender to the touch. Most (68%) present with one muscle involvement (horizontal recti > vertical recti) but some present with two or three muscles involved.27,28 Bilateral involvement is rare.27 CT shows muscle enlargement associated with tendon involvement (in contrast to thyroid associated enlargement) and a fuzzy border to the contrast-enhancing muscle (Fig. 3C). Echography is usually pathognomic showing a thickened tendon and a low reflective muscle belly.27
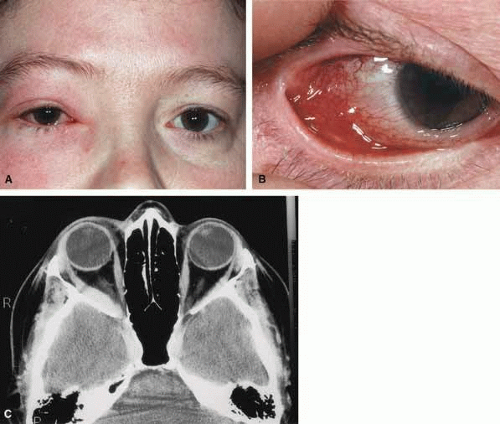 Fig. 3 A. A 22-year-old female presented with a 24-hour history of lid swelling, conjunctival chemosis/injection, pain with abduction, and double vision in horizontal fields of gaze. B. Conjunctival injection was most noticeable over the insertion site of the lateral rectus muscle. C. An axial computed tomography (CT) scan revealed an enlarged lateral rectus muscle on the right. |
Lacrimal gland involvement (dacryoadenitis) presents with pain, tenderness, injection of the temporal portion of the upper lid and conjunctival fornix with an associated tender palpable gland and an s-shaped contour deformity of the upper lid. There may be mild proptosis and a slight shift of the globe inferonasally. Imaging shows an enlarged gland with irregular margins. Other causes of dacryoadenitis, such as viral/ bacterial infections, Sjögren’s syndrome, Wegener’s granulomatosis, or sarcoidosis must be ruled out.29 A significant number of patients have the potential for some type of associated systemic disorder.29
In those with anterior nonspecific orbital inflammation the main focus of inflammation is the globe and adjacent orbital tissue (Fig. 4A and 4B). Features include pain, proptosis, lid swelling, injection, and occasionally decreased vision. Scleritis and uveitis may also be present. In those with diffuse involvement there are extraocular and neurosensory structures involved as well. Imaging shows an irregular orbital infiltrate adjacent to the globe with scleral thickening in the anterior group (Fig. 4C) and more extensive involvement with the diffuse group (Fig. 5A, 5B and 5C).
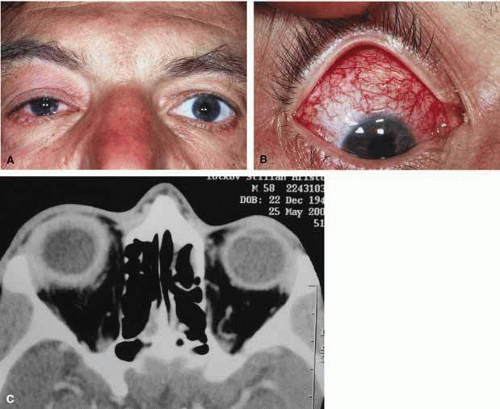 Fig. 4 A. A 45-year-old male presented with a 24-hour history of increasing eye pain and conjunctival injection. B. Diffuse scleral and episcleral injection is present. C. An axial computed tomography (CT) scan revealed diffuse enhancement of the sclera and adjacent orbital tissues. |
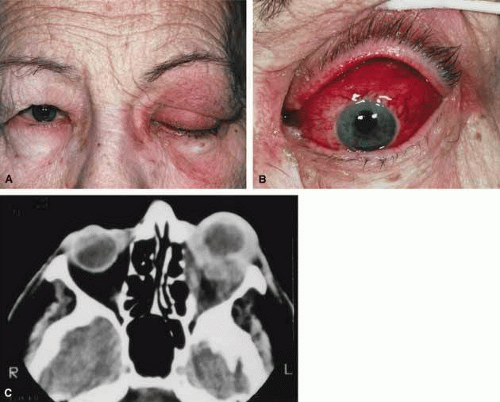 Fig. 5 A. A 72-year-old female presented with a 36-hour history of ptosis, conjunctival injection, pain, double vision, and proptosis. B. Diffuse conjunctival injection and chemosis is seen. C. Diffuse orbital inflammation is present with a mass effect anteriorly, adjacent to the globe. |
Apical involvement with nonspecific orbital inflammation is uncommon but may present with pain, decreased vision, restricted motility, mild proptosis, and chemosis. The functional abnormality is typically more than the degree of inflammation would suggest.26 These patients require careful consideration as a wide variety of disorders can present with these findings (including neoplastic processes, cavernous sinus thrombosis, etc.).
Treatment for the acute nonspecific orbital inflammatory syndrome include nonspecific anti-inflammatory medication. In mild cases nonsteroidal anti-inflammatory agents (NSAIDs) such as ibuprofen21 may help but most cases require steroids.26,27 A rapid steroid response, especially for the associated pain, is typical and most patients notice a significant improvement of symptoms over 24 hours. If the presentation is typical, as is generally the case with the myositic and anterior varieties of nonspecific orbital inflammation, a course of steroids without biopsy is common. Because a large number of the lacrimal inflammations are associated with a systemic disease, a biopsy is recommended prior to steroid use. For diffuse and apical inflammations, and those that fail to respond to steroids or have recurrent disease, a biopsy is wise to confirm the disease process.
SPECIFIC INFLAMMATIONS OF THE ORBIT
In addition to the nonspecific orbital inflammatory syndromes there are a number of more specific inflammations that may present with acute proptosis. These can be divided into those with specific local and/or systemic findings and those with specific histopathology that identifies them.26
Vasculitis
Vasculitis includes a wide range of inflammatory angiodestructive processes that involve varying calibers of vessels and diffuse types of infiltrates ranging from polymorphonuclear to necrotizing granulomatous.26 The unifying feature is evidence of vessel inflammation with varying degrees of destruction. Clinically, patients may present with acute inflammatory changes similar to the nonspecific orbital inflammation patients. The various entities are classified on the basis of symptoms related to the organs or tissue affected, as well as their principle histopathologic features.26
Although many of these disorders have relatively distinct systemic symptoms and signs, it may be difficult to diagnose them and differentiate them from nonspecific inflammatory disease if the process is restricted to the orbit during the early stages.
Wegener’s granulomatosis
Wegener’s granulomatosis (WG) is a disease of presumed autoimmune origin that in its pure form is characterized by necrotizing granulomatous inflammation of the upper and lower respiratory tract, vasculitis involving small to medium vessels, and a focal glomerulonephitis.30 It has a broad range of presentations and may occur as a systemic or localized (limited) disease. When systemic, it is characterized by widespread inflammatory effects with multisystemic damage, upper and lower respiratory tract involvement followed by renal involvement.26,30,31,32,33 In the more localized form involving the orbit, the patient may present with proptosis, periorbital inflammation, an orbital mass, and associated ocular inflammation (iritis, episcleritis, scleritis, retinal vasculitis). Bilateral orbital involvement is not uncommon.26,31
The vasculitis is necrotizing and the process is progressive and associated with destruction. Imaging may show a unilateral or bilateral poorly outlined orbital mass, infiltration and destruction of fat planes, involvement of sinuses, and bone erosion. Cytoplasmic antineutrophil cytoplasmic antibody (C-ANCA) laboratory testing is useful even in limited disease where the results are said to be positive in 60% to 70% of cases,34,35 however, it may initially be negative.31,34 Biopsy of involved tissue is essential for a diagnosis. The three classic histopathologic features of WG are vasculitis, granulomatous inflammation, and tissue necrosis. The diagnosis should be based on a combination of clinical (orbital involvement, scleritis, respiratory tract involvement, renal and sinus disease) laboratory, radiologic, and pathologic features. A specific diagnosis is essential before initiating the necessary aggressive treatment (corticosteroids and cyclophosphamide).
Polyarteritis nodosa
Polyarteritis nodosa is also a vasculitis of the medium to small arteries. Orbital involvement, although unusual, presents with nonspecific orbital inflammatory features. This entity is distinguished as a specific orbital inflammatory disorder by the pattern of involvement and histopathology. Sites of predilection are kidney, heart, liver, and gastrointestinal tract.36 It may also involve the skin, peripheral nerves, pancreas, testicles, and skeletal muscles. Clinically, the patients often have fever, malaise, leukocytosis, and evidence of multisystem involvement. Other ophthalmologic features include retinal and choroidal infarcts, corneal and scleral necrosis. Definitive diagnosis requires a biopsy of involved tissue. Treatment, similar to that for WG, involves corticosteroids and cyclophosphamide.
Collagen Vascular or Connective Tissue Disorders
Any of the connective tissue disorders may also be associated with a systemic vasculitis including systemic lupus, rheumatoid arthritis, and dermatomyositis.26,37,38 Orbital involvement is uncommon. The clinical picture may be identical to the nonspecific orbital inflammations previously discussed and may be treated as such. A definitive diagnosis is based on the pattern of systemic disease, laboratory testing and/or radiologic and pathologic features.
THYROID ORBITOPATHY
Thyroid-related eye disease (Grave’s disease) has been recognized by the medical community for more than two centuries. The eye signs of Grave’s disease are a symptom complex that describes the response of the eyes to an inflammatory disorder within the orbital tissues. It is therefore best thought of as an infiltrative orbitopathy rather than an ophthalmopathy.38,40
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


