Accommodating Intraocular Lenses
John F. Doane
Randolph T. Jackson
Although great minds including Leonardo da Vinci and Rene Descartes examined the problem of presbyopia, it was an American, Benjamin Franklin, who invented the first treatment by introducing bifocal spectacles around 1785.1 A surgical solution would have to wait over 200 years until cataract surgery progressed to its current refinement with presbyopic intraocular lenses that can simultaneously improve distance, intermediate and near vision. In the 21st century, intermediate focal points with computer, personal digital assistants, and cellular phones are now at a premium. And so, with the advent of accommodative and multifocal intraocular lenses, ophthalmic surgeons have the opportunity to treat presbyopia and facilitate near, intermediate and distance vision for their patients. At present, there are no less than 13 corporate entities and numerous lens designs that are attempting to commercialize accommodative intraocular lens devices. One FDA approved accommodating and three multifocal lenses are available for clinical use at of the beginning of 2007 in the United States. Ophthalmic surgeons are currently able to improve the range of visual focus in both eyes of a patient to maintain binocular function while avoiding the unwanted mesopic and scotopic visual disturbances experienced with monovision and older style multifocal lens technologies. Presbyopic intraocular lenses are revolutionizing cataract visual rehabilitation and improving the options for refractive lens exchange procedures.
Surgical correction of refractive error cleared two large hurdles in the 20th century. The third hurdle in restoration of visual function is occurring in these first years of the 21st century. In the first step, November of 1949, Sir Harold Ridley implanted the first intraocular lens following cataract extraction. The second revolutionary step was the introduction and now firm foundation created by the excimer laser vision correction era. The third hurdle being cleared is the solution of presbyopia in which a single eye can see clearly at distance, intermediate and near focal points without external visual aid in the form of spectacle or contact lens. This visual function ability is completely different from monovision where one eye is emmetropic and the fellow eye has a myopic refractive error. This third step in refractive correction is a momentous achievement like the first two. In one sense, it may be even more powerful, because surgical correction can now solve for the accommodative process that is lost by all those who live beyond age 40. It is estimated that this includes over 590 million people worldwide.2 Importantly, in the computer age where individuals spend upwards of 8 or more hours per day viewing a computer video monitor, this ability to focus at near and intermediate focal points becomes critical for job performance and leisurely pursuits. In this chapter, it is the hope of the authors to provide the reader with insight into the history, mechanism of action, clinical evaluation, operative technique, and postoperative management of accommodative intraocular lenses.
Sixty Years of Advancement
From refractive and cataract surgery standpoints the state of technology has shown wonderful advancements each decade since the 1940s. Cataract surgery has gone from no intraocular implant to astigmatically neutral small chord-length incisions, limbal relaxing incisions to neutralize astigmatism, foldable intraocular lenses with UV absorbing chromophores and edge designs that reduce posterior capsule opacification. From the refractive surgery perspective, we have taken corneal refractive surgery that had a predictability range of ±2 to 3 diopters to a predictability range closer to ±0.25 diopters, we have gone from procedures that could not treat astigmatism to techniques that can treat upwards of 8 diopters on a single attempt, and we have seen recovery times of weeks to months change to hours. Despite these grand accomplishments, the refractive and cataract surgery fields have not completely answered the presbyopic dilemma. To date, both disciplines have attempted a compromise of binocular function with monovision which certainly takes away maximal visual function at all focal points and requires an adaptation period of days to months for those even able to tolerate the refractive discrepancy. Cataract surgery and to some extent refractive surgery have tried to treat presbyopia with a multifocal approach. Early attempts using a multifocal intraocular lens had mediocre success due to the pitfalls of “splitting” light for various focal points. By theory alone, this appears from the outset to be less than ideal. In practice, a certain percentage of patients will report unwanted mesopic or scotopic symptoms and are subsequently dissatisfied with their operative endpoint.3 There are various methodologies of multifocal implants, diffractive and refractive, that in part circumvent these issues but with theoretic and physiologic constraints.
Multifocal laser ablations of the cornea have been under clinical study for nearly 10 years. Despite international efforts, to date, a technique has not yet evolved to provide a highly predictable, efficacious, and stable result of acceptable vision quality to be embraced by even a small minority of surgeons. Due to corneal epithelial remodeling, as can occur after hyperopic LASIK, relatively minor multifocal contour changes on the cornea may not last.4
Scleral approaches to either weaken or add scleral inserts to facilitate accommodation have been studied with conflicting claims over the past two decades.5 Due to the limited success of corneal and scleral approaches, most research is currently focused on accommodating and multifocal implants. Now, with well-constructed clinical trial outcome data, there are operative approaches that while not perfect can be a successful answer to presbyopia that thus far has eluded the fields of cataract and refractive surgery.
Accommodating IOL History
The genesis for the interest of accommodative intraocular lenses comes from the innovative work of J. Stuart Cumming, MD of California. In the 1980s, Dr. Cumming made an interesting observation of patients who had been implanted with plate haptic silicone IOLs. Some of these patients were able to read exceptionally well through their distance correction. Although part of this could be explained by pseudoaccommodative effects, such as miotic pupil, corneal multifocality via micro irregular astigmatism and corneal curvature steep at 180 degrees, it could not be fully explained by these effects.6 Dr. Cumming began investigations of intraocular axial movement of silicone plate haptic lenses with A-scan ultrasonography by pharmacological induction of ciliary muscle contraction and relaxation with pilocarpine and cyclopentolate, respectively. He noted optic movement of 0.7 mm on average. Encouraged by these findings, he felt there may be opportunity to seek alternative designs to accentuate these early results. He was encouraged when he discovered the work of Bussaca in 1955 as reported in Annales D’ Oculistique, which showed anterior movement of the zonular insertion and the ciliary muscle mass encroaching on the vitreous cavity when young aniridic patients were observed by gonioscopy. He also found D. Jackson Coleman’s work on the “Hydraulic Suspension Theory of Accommodation” of extreme importance from a theoretical and practical sense.7 Cumming’s concept gained more credence when Spencer Thorton in 1986 demonstrated axial movement and shallowing of the anterior chamber with three-piece loop lens with accommodation stimulus as observed with A-scan ultrasonography. Beginning in 1990, Dr. Cumming initiated a series of accommodating intraocular lens designs that were studied in Germany with Professor Jochen Kammann. Seven lens designs were implanted over a 7-year period.8 The seventh and current lens design is the IOL that underwent FDA trials and was approved for commercial usage in late 2003 in the United States. Below is a more detailed description of this hinged optic design.
Accommodating Intraocular Lenses
Single Optic or Shift Optic
Plate Style Accommodating Intraocular Lenses–EyeOnics CrystaLens
The commercially available CrystaLens is the seventh iteration IOL from Eyeonics (Fig. 1). The CrystaLens is intended for primary implantation within the capsular bag. It is not indicated for sulcus fixation. In order to maintain fixation within the capsular bag, polyimide loops are placed across the ends of the plate haptics. The overall length of the lens from loop-tip to loop-tip is 11.5 mm, and the plate length is 10.5 mm. Grooves or hinges which are 50% thickness of the plate are positioned immediately adjacent to the 4.5-mm optic. The lens is available at present in powers of +4.0 to +33.0 diopters. The optic has a square edge and is manufactured from Biosil, a third-generation silicone, and has no internal reflectivity unlike other IOL materials such as polymethylmethacrylate and acrylic. Third-generation silicone is used to attain maximal biocompatibility, strength and flexibility, since the hinge must be capable of unlimited bending. In addition, Biosil allows excellent compressibility so the lens can safely pass through a sub-3 mm-incision. The “A” constant is 119.24. The 4.5 mm optic of the AT-45 was selected, because the optic rests posteriorly on the capsular bag in close proximity to the “nodal” point and, therefore, functions more like a 6.0 mm optic that rests more anteriorly. Eyeonics recently released the CrystaLens AT-50 with a slightly larger optic of 5.0 mm in hopes of reducing any night issues even further for patients with larger pupils. The fact that the length of the plate haptics are directly proportional to the posteroanterior travel or accommodative amplitude, the longer haptics allow for a greater range of travel for a given angle of deflection. So, long haptics and subsequently a smaller optic allow for maximal posteroanterior movement. In 2005, Kevin Waltz, MD, postulated that the thin optic of eyeonics Crystalens, as a secondary mechanism of action, could bend forward and increase the anterior radius of curvature in much the same way the natural crystalline lens functions. He conducted in vivo tests in patients after implantation of the CrystaLens using the Tracey aberrometer (Houston, Texas) and found increased accommodative focus when near stimulus was presented (personal communication, 2005). In 2007, this was corroborated with real-time video of a patient who traumatically lost all of his iris, but maintained and intact posterior capsule. (On file at eyeonics, Aliso Viejo, CA)
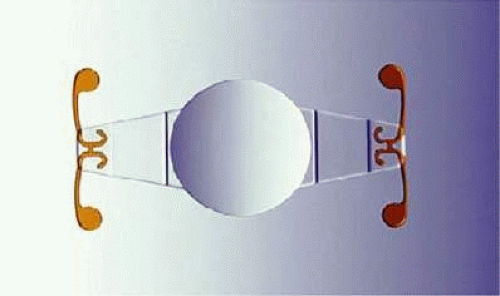 FIGURE 1. EyeOnics CrytaLens. Adjacent to the 4.5-mm optic are 50% thickness grooved hinges in the plates. At the end of the plates are two polyimide haptics that allow 4-point in-the-bag fixation. |
Refractive Results of the CrystaLens
Limited clinical results are available with accommodative lenses to date.9,10,11 The most comprehensive results come from the CrystaLens FDA clinical trials data. At 2 years postoperatively in the FDA clinical trial, monocular uncorrected and distance corrected visual acuities were 58.4% and 87.3% for 20/20 or better, 76.9% and 96.5% for 20/25 or better, 84% and 97.7 % for 20/32 or better, and 91.9% and 98.2% for 20/40 or better, respectively (n = 173 eyes). At 2 years postoperatively, the monocular uncorrected and distance corrected near visual acuities were 48.8% and 28.1% for J-1 or better, 73.3% and 56.7% for J2 or better, and 95.3% and 88.3% for J3 or better, respectively (n = 172 eyes). Binocular uncorrected visual acuities for distance, intermediate, and near at 2 years postoperatively were 96.2%, 98.6%, and 74% for 20/25 or better, 100%, 100%, and 89% for 20/32 or better, and 100%, 100%, and 98% for 20/40 or better, respectively (n = 53 subjects).11 Interestingly, the near visual acuity improves over the course of time and is noticed by patients and clinicians alike (Fig. 2).
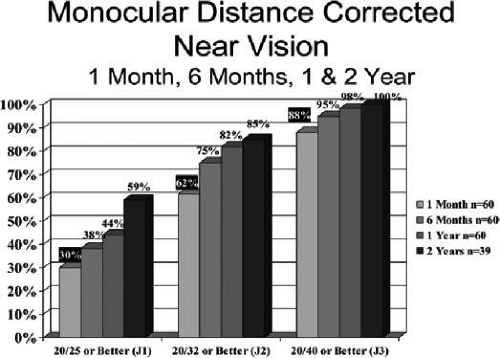 FIGURE 2. (Data from JF Doane, FDA Clinical Trial Data). Note improving distance corrected near vision with serial examination out to 2 years. |



