Acanthamoeba Keratitis
Romesh K. Gautom
Thomas R. Fritsche
Thomas D. Lindquist
Since 1958, certain species of small, free-living aerobic amebae belonging to the genera Acanthamoeba, Balamuthia, and Naegleria have been recognized as being responsible for causing a fatal disease of the central nervous system (CNS) in humans and laboratory animals.1,2,3,4,5,6,7 These small, free-living amebae are an important component of the protozoal fauna of soil and water, and they are cosmopolitan in distribution.1,8,9,10 Naegleria fowleri is responsible for an acute and uniformly fatal CNS infection known as primary amebic meningoencephalitis, and is most commonly acquired after accidental introduction of amebae into the nasal passageways upon exposure to water. This species is thermotolerant, growing to high densities in warm, stagnant bodies of water, including freshwater lakes, natural geothermal spas, and poorly maintained swimming pools. In contrast to N. fowleri, certain species of Acanthamoeba and Balamuthia mandrillaris are responsible for a slowly progressive infection of the CNS known as granulomatous amebic encephalitis. More than 200 cases of granulomatous amebic encephalitis have been reported worldwide.3,6,11 Although both primary amebic meningoencephalitis and granulomatous amebic encephalitis are uniformly fatal, the latter occurs more commonly in those with immunosuppressive disorders.12 Patients with acquired immunodeficiency syndrome (AIDS) are known to be at increased risk for the development of CNS or disseminated Acanthamoeba infection.13,14,15,16
The more common infection caused exclusively by Acanthamoeba is amebic keratitis. This is a nonfatal but painful and vision-threatening infection of the cornea of an otherwise healthy person.17,18,19,20,21 The earliest reports of Acanthamoeba keratitis were associated with corneal trauma and subsequent exposure to contaminated water. However, a clear association of this disease with contact lens usage has subsequently unfolded.22,23,24,25,26,27,28 Transmission is presumed to occur through contamination of contact lens cases and contact lenses from environmental sources. Hundreds of cases of this disease have been reported worldwide, with estimates of 80% to 90% of cases occurring in contact lens users.6,8,19,29 The actual number of cases of Acanthamoeba keratitis occurring worldwide is undoubtedly much higher because of unpublished data, nonstandardized reporting systems, and misdiagnoses.
BIOLOGY OF ACANTHAMOEBA
MORPHOLOGY AND LIFE CYCLE
The life cycle of Acanthamoeba consists of growth and replication by simple binary fission with two alternating morphologic forms: (1) trophozoite and (2) cyst. In the trophozoite stage, amebae are actively feeding and phagocytosing a variety of other microorganisms, especially bacteria and yeast. Mitotic division occurs at distinct intervals, depending on nutrient availability and conducive environmental conditions. Depending on the species, trophozoites range in length from 10 to 50 μm and usually display a broad, clear hyaline zone at the anterior end. Locomotion is slow, usually directional, and is caused by the flow of cytosolic contents from the endoplasm into the ectoplasmic region. During locomotion, the anterior hyaline region produces a large number of slender, needlelike pseudopodial projections. These projections are known as acanthopodia, and are a defining characteristic of the family. Cytoplasmic vacuoles are prominent and mostly concentrated in the posterior half of the ameba. A single, large contractile vacuole, important for osmoregulation, is usually seen. Amebae are usually uninucleate, but multinucleate forms are not rare. The nucleus contains a large, dense, and centrally located nucleolus surrounded by a clear halo. During mitosis, the nuclear membrane and nucleolus disappear, and a typical spindle is formed.30
A variety of adverse environmental or nutritional changes may trigger the transformation of the trophozoite into the double-walled cyst characteristic of the genus.31 Acanthamoeba cysts readily survive cold or dry environmental conditions, as well as exposure to many antimicrobial agents and disinfectants. They are variable in shape and size (range, 15 to 30 μm), depending on the species. The inner wall (endocyst) varies in shape from circular to polygonal or stellate, whereas the outer wall (ectocyst) is usually wrinkled. The ectocyst usually follows the contour of the endocyst, with intermittent junctions (ostioles) appearing between the two, giving rise to the polygonal to stellate appearance of the cyst. These ostioles remain plugged by opercula until excystation is initiated. During excystation the ameba detaches itself from the inner cyst wall and dissolves the operculum, escaping through the ostiole.
TAXONOMY
Considerable confusion exists regarding the taxonomy of those free-living amebae that have been implicated as opportunistic pathogens. N. fowleri is unique among this group in that it is an ameboflagellate; it can be readily differentiated from the others by its ability to produce a motile, flagellated stage, a feature typical of the order Schizopyrenida (Table 1).32 Pathogenic amebae that do not produce a flagellate stage have been grouped within the order Amoebida, and within either the Hartmannella or Acanthamoeba genus, depending on characteristics such as nuclear division and cyst morphology.30,33,34,35,36 More recently, Page37,38 separated these two genera on the basis of locomotive form, behavior, and cyst characteristics. The two have also been shown to be distinct antigenically.39 Many species now classified as Acanthamoeba were known as Hartmannella in older publications. The taxonomy of Balamuthia and other amebae in the order Leptomixida is uncertain, awaiting further studies for clarification (see Table 1).
TABLE 1. Taxonomic Classification of Some Free-Living Amebae | |||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||
To date, at least 20 species of Acanthamoeba have been described, based primarily on subtle differences in size and cyst morphology. As a practical exercise, however, it is difficult to differentiate among these species because of the subjective nature and unreliability of the described diagnostic characteristics. Methodologic differences alone are substantial, but even the examination of clonal populations reveals considerable variability in cyst sizes and morphology. Pussard and Pons40 categorized all Acanthamoeba species into three major groups on the basis of cyst morphology and size (Table 2):
| |||||||||||||||||||||||||
Group I consists of four species with large trophozoites and cysts. The cysts usually have smooth ectocysts and are greater than 18 μm in diameter. The endocysts are stellate and the opercula are usually located at the level of the ectocysts.
Group II comprises 10 species whose cysts have wrinkled, rippled, and irregular ectocysts measuring less than 18 μm in diameter. The endocyst may be stellate, polygonal, triangular, or sometimes rounded without prominent rays (arms). The opercula are present within the depressions of the ectocysts. Most of the species implicated in the etiology of Acanthamoeba infection belong to Group II.
Group III consists of five species having thin ectocysts, either gently rippled or smooth, measuring less than 18 μm. The endocysts are usually rounded or may have three to five rays.
Despite attempts to simplify the identification of acanthamoebae, taxonomic status of known species remains questionable. Recent studies employing molecular-based techniques (e.g., isoenzyme profiles, mitochondrial DNA and 18S rDNA restriction fragment length polymorphisms, ribosomal gene sequence analysis) may offer approaches to identification that represent an improvement over traditional morphologic studies.41,42,43,44,45
ECOLOGY
Acanthamoebae are among the most common protozoa in soil and water ecosystems worldwide. They are specialized predators of bacteria, fungi, and other protozoa and play an important role in nutrient cycling in those habitats in which their food sources thrive. Encystation allows the amebae to survive untoward environmental changes, including temperature extremes, desiccation, lack of nutrients, increase in salinity, and disinfection. Acanthamoebae have been isolated from a variety of environmental habitats, although their preferred habitat appears to be soil, which provides a source of oxygen, water, optimum survival temperature, and a continuous bacterial food supply.46,47 Soils high in organic matter content, and subsequently in numbers of bacteria, will contain the greatest numbers of amebae.48,49 Vertical distribution studies50 have shown that they are present in the littoral and profundal sediments of pond and lake waters, respectively. Acanthamoebae are also known to be present in tap water, faucet aerators and shower heads, and well water, among other sources that may be epidemiologically linked to human infections.42,43,45
OCULAR INFECTIONS WITH ACANTHAMOEBA
ACANTHAMOEBA KERATITIS
Among the 20 or more named species of Acanthamoeba that have been distinguished by cyst morphology, immunofluorescent antibody testing, or isoenzyme profiles,51 5 have been repeatedly identified by culture or immunofluorescent antibody testing as being responsible for keratitis: Acanthamoeba castellanii, Acanthamoeba culbertsoni, Acanthamoeba hatchetti, Acanthamoeba polyphaga, and Acanthamoeba rhysodes (see Table 2).
The development of Acanthamoeba keratitis is associated with mild antecedent trauma in the majority of cases.29,52 This can be in the form of vegetable matter, insects, paint thinner, wind-blown contaminants, sawdust, or contact lens wear in which microabrasions of the cornea may develop.53,54 Exposure of the damaged corneal epithelium to amebic trophozoites or cysts may result in their attachment and subsequent invasion.
The earliest manifestation of Acanthamoeba keratitis is frequently the development of a dendritiform epithelial pattern (Fig. 1).55,56,57 This dendritiform keratitis may represent epithelial infection before the development of any stromal involvement. This contention is supported by the rapid resolution of symptoms after wide epithelial débridement.56,58 A dendritiform epithelial pattern presenting early in the course of Acanthamoeba keratitis may explain why the great majority of patients have undergone treatment for herpes simplex keratitis before the correct diagnosis was established.26,56 Dendritiform lesions of Acanthamoeba keratitis do not truly mimic herpes simplex dendrites, which form frank ulcerations of the cornea; rather, amebic keratitis causes an edematous and necrotic appearance of the involved epithelium. Mottled epithelial staining or frank epithelial defects may be seen; however, an intact epithelium is frequently noted. The dendritiform pattern of Acanthamoeba keratitis does share some similarity to that of herpes zoster infection, which is composed of swollen cells, often lined with mucus, that give it a linear, gray, plaquelike character. On initial presentation, the epithelium may be intact despite a mottled or dendritiform appearance, but the epithelium frequently breaks down repeatedly.56,57,59 Variable, persistent, or recurrent epithelial erosions characterize this infectious process.
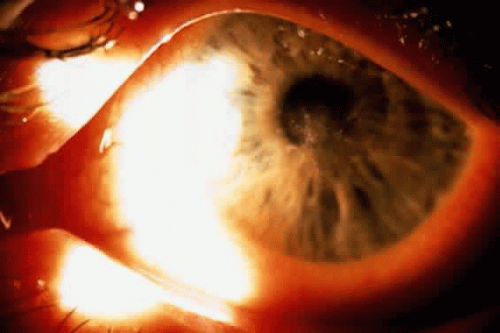 Fig. 1. Early corneal epithelial infection with Acanthamoeba species showing a dendritiform epithelial pattern. |
Moore and associates57 described radial keratoneuritis as a presenting sign in Acanthamoeba keratitis. Radial keratoneuritis is characterized by linear, radial, branching infiltrates found in the midstroma, which appear to be located along corneal nerves. These infiltrates begin paracentrally and extend to the limbus in a radial pattern.
Conjunctival injection and chemosis are present as a rule. Adenopathy may or may not be present. Acanthamoeba keratitis is characterized by a fluctuating, nongranulomatous inflammatory reaction in the anterior chamber. McClellan and Coster60 cultured Acanthamoeba organisms from an anterior chamber paracentesis in a patient with severe keratitis. Elevated intraocular pressure and cataract, presumably secondary to the anterior segment inflammation, may be seen. Mannis and colleagues59 reported that 39% of cases demonstrated sufficiently pronounced anterior segment inflammation to produce hypopyon. Severe pain, often out of proportion to the degree of anterior segment inflammation, characterizes this disorder, particularly as the keratitis becomes chronic.24,57,59,61 Patients who present with epithelial involvement alone may not complain bitterly of pain.56 A distinguishing feature of Acanthamoeba keratitis is the prominent scleral inflammatory component. Although anterior scleritis may be part of the clinical presentation, the severe ocular pain characteristic of Acanthamoeba keratitis suggests that scleritis may occur commonly in chronic cases of Acanthamoeba keratitis. In some reported cases, the ocular pain became so severe that retrobulbar alcohol injections had to be given.62
A ring-shaped stromal infiltrate is characteristic of advanced infection and is nearly pathognomonic of Acanthamoeba keratitis (Fig. 2).61 The infiltrate is often most dense in its peripheral aspects, forming a characteristic ring. This annular infiltrate may be segmental or circumferential, may be progressive, often involves stromal thinning or furrowing, and may be associated with a variable overlying epithelial defect. The arcuate or ringlike infiltrate is due to polymorphonuclear leukocyte infiltrates generated by chemotaxis after antigen-antibody precipitation,63 analogous to the infiltrate described by Wessely64 after injecting horse serum into the cornea.65
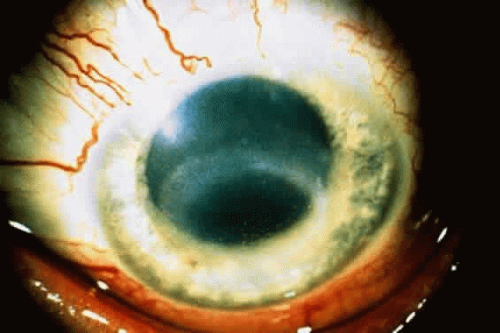 Fig. 2. A paracentral ring infiltrate is shown, characteristic of late Acanthamoeba keratitis. |
NONKERATITIC OCULAR DISEASE
Nodular scleritis has been reported in 14% of cases of Acanthamoeba keratitis.59 Significant scleral ectasia was reported in one patient, who was not treated because of a delayed diagnosis.66 Posterior scleritis and optic neuritis have been noted in association with Acanthamoeba keratitis.59,67,68 Acanthamoeba was seen histopathologically in the ciliary body of one patient, in whom fatal meningoencephalitis developed.23 Amebic organisms have also been implicated as a cause of exudative chorioretinopathy.69
The potential for spread of Acanthamoeba keratitis to the posterior segment appears to be low. There have been many reported cases of corneal perforation or keratoplasty performed in the face of active infection, including penetrating keratoplasty performed in conjunction with cataract extraction, in which posterior segment involvement has not become evident.
EPIDEMIOLOGY
The earliest reports of Acanthamoeba keratitis were associated with penetrating corneal trauma and exposure to contaminated water.67,68,70,71,72,73,74,75,76,77,78,79 However, a clear association with daily-wear or extendedwear soft contact lenses has since unfolded.19,24,53,56,57,59,61,80,81,82,83,84,85 In 1989, Stehr-Green and co-workers19 identified 208 cases of Acanthamoeba keratitis within the United States. Eighty-five percent of patients wore contact lenses, and of those, the majority wore soft contact lenses; only 9% wore rigid gas-permeable or hard contact lenses. Sixty-four percent of contact lens wearers who developed Acanthamoeba keratitis gave a history of using homemade saline prepared by using nonsterile distilled water and salt tablets. Chynn and colleagues52 have since reported that 36% of patients with Acanthamoeba keratitis did not wear contact lenses, suggesting that proper education of contact lens wearers may be changing the epidemiologic characteristics of the disease. In addition to contact lens use, important risk factors for developing Acanthamoeba keratitis now include exposure to contaminated water and corneal trauma from plant materials.
Stehr-Green and associates19 found a nearly equal distribution of Acanthamoeba keratitis cases among males and females. Males, however, account for a minority of soft contact lens wearers in the United States, suggesting that males may adhere less stringently to recommended disinfection procedures or may increase their risk of corneal trauma or exposure to polluted water in some manner.
The presence of bacterial or fungal contamination within the contact lens care system may be an important element for the survival and growth of Acanthamoeba organisms. Donzis and co-workers86 analyzed bacterial and fungal contamination of the contact lens care systems of 10 patients who also had Acanthamoeba species detected within their care systems. Gram-negative bacteria were found in all 10 care systems, and Pseudomonas species were found in 6. Fungi were also isolated in 6 of the 10 care systems. Of interest was the finding that Acanthamoeba organisms were found only in contact lens cases or solutions that also had concomitant bacterial or fungal contamination. Larkin and colleagues87 found that 7% of asymptomatic contact lens wearers had storage cases that were contaminated with free-living amebae; six of seven patients with Acanthamoeba-contaminated storage cases had significant numbers of contaminating bacteria. The most recent assessment of contact lens storage contamination showed that 81% of storage cases were contaminated: 77% grew bacteria, 24% fungi, and 8% Acanthamoeba species.88 Bacterial cocontamination of contact lens systems harboring Acanthamoeba has been well documented by several additional studies.89,90 Acanthamoeba organisms display selective bacterial feeding, particularly nonfermentative gram-negative organisms and coliforms.91 Although Pseudomonas aeruginosa has been found to co-contaminate contact lens cases, this organism produces a toxin that is highly lethal to A. castellanii and A. polyphaga; therefore, Acanthamoeba species and P. aeruginosa may be mutually exclusive eye pathogens.92 The presence of bacteria and possibly fungi within the contact lens care system may be an important food source for acanthamoebae, resulting in their enhanced growth. Clearly, the attack rate of Acanthamoeba keratitis in no way approximates the 7% to 8% incidence of contact lens case co-contamination with Acanthamoeba and bacterial species.
By use of the scanning electron microscope, Acanthamoeba organisms have been shown to adhere to the surface of contaminated hydrogel contact lenses.53 Several subsequent studies93,94,95 have shown that both Acanthamoeba cysts and trophozoites can firmly adhere to unworn soft contact lenses. The adherence of these organisms to contact lenses may play a significant role in the pathogenesis of Acanthamoeba keratitis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


